

Review Article
Volume-1 Issue-1, 2021
Anticancerous Properties of Pterocarpus santalinus
Received Date: November 28, 2021
Accepted Date: December 28, 2021
Published Date: December 30, 2021
Journal Information
Abstract
Cancer is a group of diseases, characterized by uncontrolled cellular growth with frequent cancer cells invasion to different body parts and spreading to other organs, a process referred to as metastasis. Cancer is a leading cause of death worldwide. Chemotherapy is the main approach used currently for the treatment and management of this disease especially disseminated malignant tumors. Unfortunately, most patients often relapse or have reduced responses to initial chemotherapy.
Current therapeutic strategies are known to have substantial adverse effects, necessitating further study into alternate strategies, such as those derived from natural resources. Pterocarpuss species have been extensively used in folk medicine for thousands of years. However, there is a paucity of information on the cytotoxic properties of these plants. Therefore, the present study was undertaken to evaluate the cytotoxic and apoptotic activity of the selected Pterocarpuss species, namely Pterocarpuss santalinus.
Cytotoxic activities were screened using an in vitro assay system of growth inhibition against human cancer cell lines. s. Cytotoxic activities were screened using an invitro assay system of growth inhibition against human cancer cell lines. The plant extract demonstrated selective cytotoxic activity and apoptosis in cancer cells. The results demonstrated that Pterocarpuss santalinus has strong cytotoxic effect by inducing apoptotic cell death, and causing arrest of cancer cells at different growth phases. Hence, Pterocarpuss santalinus has the potential to be further exploited for the discovery and development for new anticancer pharmaceuticals.
Key words
Pterocarpuss Santalinus, Cancer, Cytotoxix Activities, Anticancer Pharmaceuticals
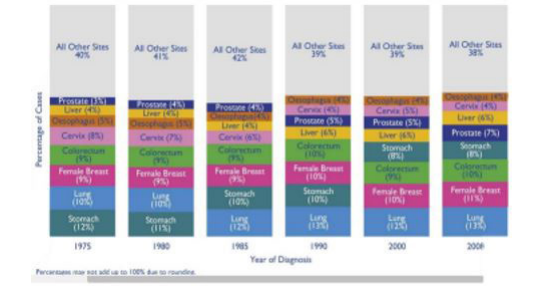 |
| Figure 1.1: The most common cancers diagnosed worldwide between 1975 and 2008, from Cancer Research UK (2011a) |
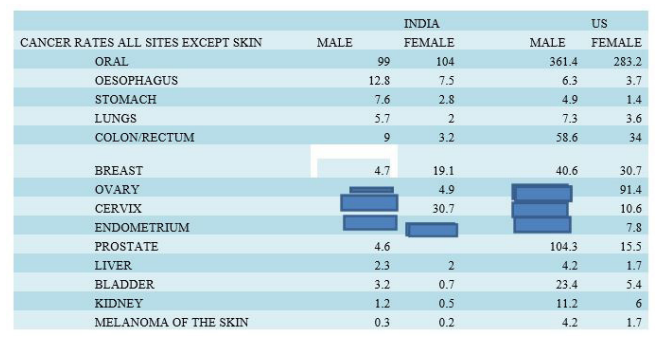 |
| Figure 1.2:The most common cancers diagnosed in females worldwide and in the India and UK, from Cancer Research UK (2011b) |
 |
Introduction
In the more recent history, the use of plants as medicine has involved the isolation and characterization of pharmacologically active compounds (Balunas and Kinghorn, 2005). [1] Today there are at least 120 distinct chemical substances derived from plants that are considered as important drugs and active ingredients in the pharmaceutical industry (Prasanna et al., 2009). Plant-derived natural products still remain as an essential component in the search for medicines and continue to provide new and important leads against various pharmacological targets including cancer, HIV/AIDS, Alzheimer’s, malaria, and pain (Balunas and Kinghorn, 2005) In present time, the cancer treatment by chemotherapeutic agents, surgery and radiation have not been fully effective against the high incidence or low survival rate of most cancers (Moongkarndi et al., 2004. The search for new anticancer agents from plant sources is one of the realistic and promising approaches in the field of cancer chemoprevention and this led to the discovery of many novel anticancer drugs. (Rowinsky et al., 1992)
Pterocarpus santalinus (Fabaceae) is one such herbal drug which finds its place in Ayurveda. Numerous important bioactive phytocompounds have been extracted and identified from the heartwood of P. santalinus. Bioactive compounds naturally occur in small amounts and have more subtle effects than nutrients. These bioactive compounds influence cellular activities that modify the risk of disease rather than prevent deficiency diseases. However, it is not known which compound of the P santalinus leads to cytotoxicity, metastasis, and apoptosis.
Cancer
Cancer is a collection of disorders involving aberrant cell growth. In normal circumstances, cell division is a highly controlled process in which an error, such as an unrepaired genetic mutation, is detected during the cell cycle and leads to programmed cell death, also known as apoptosis. [2] When cancer cells become uncontrollably proliferate, they usually form a tumour. Some tumours have the ability to infiltrate or spread to other areas of the body, resulting in secondary tumours or metastases, these tumours are called malignant tumours. In contrast to benign tumors, they do not spread to other parts of the body. Increased exposure to mutagens such radiation and DNA reactive compounds, combined with the ageing population in developed countries, has dramatically increased the likelihood of developing cancer over one's lifespan.
Cancer Epidemiology
Cancer Incidence
Cancer incidence refers to the number of new cancer cases occurring in a defined population within a given time period (Last J.M., 2011). [3] The cancer incidence rate is the rate at which new cases of cancer occur within the population. The numerator is the number of new cancer cases that occur in a defined time; the denominator is the population at risk of developing cancer during this time, sometimes defined using person-time (Last J.M., 2011).
Global Trends
It is estimated that 12.7 million cancer cases were diagnosed worldwide in 2008. (Cancer Research UK, 2011a). As shown in Figure 1.1, between 1975 and 2008, there were changes in the pattern of incident cases, are thought to be due to an association between lifestyle changes and the progression of the cancer diagnostic tests (Cancer Research UK, 2011a). In 1975, gastrointestinal (12%), lung (10%), and female breast cancer (9%), were the first of the three forms of cancer are diagnosed around the world. In 2008, the picture has changed, lung cancer (13%) was the most common type of cancer diagnosed worldwide, and is followed by female breast cancers (11%), and colorectal cancer (10%). [4] The high incidence of cancer cases is evident in developed countries such as Australia. The lowest rates are observed in the less developed countries in Africa and Central America (Cancer Research UK, 2011b)
India Trends and Risk Factors
According to the World Health Organization (WHO), cancer incidence rate in India is much lower than in more developed countries such as the United States (Fenley J, 2001). [5] Data from the population cancer registries in India, illustrate that the most frequently reported cancer sites in males are lung, esophagus, stomach, and larynx. Cervical, breast, ovarian, and esophageal cancers are the most common in females. (Gajalakshmi V, 2001) Oral cancer rates in India are among the highest in the world, 5 most of them are related to diet, weight, and other lifestyle factors. One of the important lifestyle risk factors, is betel quid (paan) chewing, a practice that has been prevalent in India. Oesophageal cancer is the second most common form of cancer in men and the fourth most common cancer in women, according to combined data from the cancer registries in India. 6 Among the risk factors for oesophageal cancer in India and the chewing of betel quid is carrying a relative risk of 1.5 to 3.5. The female genital tract cancer has a high incidence among Indian women. [6] Types of the human papilloma virus (HPV) is the most common risk factor for cervical cancer, and is associated with ovarian and endometrium. Cervical cancer is the most common cancer of the female genital tract, in India, with more than 100,000 new cases per year.
Cancer Mortality
Global Trends
Mortality is another measure of disease occurrence. It is measured using the mortality (death) rate, which is an estimate of the number of deaths occurring in a defined population during a specified period, i.e., the death rate per 10n person-years (Last J.M., 2001). [7] The cancer mortality rate is the number of deaths due to cancer in the defined population during a specified period of time; it is a form of incidence rate – i.e., new events occurring in a population (MacMahon &Trichopoulos, 1996). India Trends
Risk of dying from cancer before the age of 75 years is 7.34% in males and 6.28% in females. Cancer of oral cavity and lungs account for over 25%. An estimated 0.44 million died due to cancer during the year 2011, while 0.51 million and 0.60 million persons are likely to die from cancer in 2016 and 2021. [8] In the year 2011 male mortality was estimated to be 0.23 million and female mortality to be 0.20 million. The estimated cancer mortality would increase to 0.70million by the year 2026 as a result of change in size and composition of population. In males increase will be to 0.38 million and in females to 0.32 million. Among women, cancer of the breast, cervical and ovary account for 34 percent of all cancer deaths. The leading sites of cancer mortality in males are lung, oesophagus, prostrate and stomach. (Neevan DR Dsouza, 2011)[9]
Current Treatment for Cancer
There are several approaches for cancer treatment and management, which include mainly surgery, radiotherapy, photodynamic therapy and chemotherapy. It is the case that most often more than one approach is used depending on the nature and stage of the cancer. The treatment also depends on the patient’s general health condition, age and lifestyle.
1. Surgery
2. Radiotherapy
3. Photodynamic Therapy
4. Chemotherapy
Pterocarpuss santalinus
Selection of Pterocarpus santalinus Extracts
Pterocarpus santalinus (Sanskrit: Raktachandan; Family: Fabaceae) commonly called as red sander is the evergreen tree found in the dry regions of south India and in north India. It is an endangered plant species endemic to the state of Andra Pradesh in India (Pandey, 1980; Anuradha et al, 1999). It is described in Ayurveda for its wide spectrum of medicinal properties [10].
The heartwood of P. santalinus is used as astringent tonic as external application for wounds, cuts and inflammation, in treating headache, 5 skin diseases, fever, boils, scorpion sting and to improve sight (Jain, 1996; Chopra et al, 1956). Santalin, is a natural dye from red wood that is used as a colouring agent in pharmaceutical preparation, foodstuffs. It is also used as a cooling agent in pharmaceutical preparations. Fruit extract is used as astringent, diaphoretic, in inflammation, headache, skin diseases, and bilious infections and chronic dysentery. The P. santalinus contains a larger no. of such compounds as alkaloids, phenols, saponins, glycosides, flavonoids, triterpenoids, sterols and tannins [11].
Methodology
Cytotoxicity screening of Pterocarpuss santalinus via MTT Assay
Cell lines used SKOV3 cell line
It is a human ovarian cancer cell line having epithelial-like morphology. Its growth temperature is 37 degrees Celsius and its doubling time is 35 h. (source –ATCC)
• Cells were seeded into 96-well micro titer plates at a density of 5 x 103 per well and allowed 24 h to adhere before drugs were introduced (final concentration 0.1 nM -100 mM, n = 8).
• Serial drug dilutions were prepared in medium immediately prior to each assay and the cells was treated with respective drugPS765008A for next 24h.
• Following 24 hours’ exposure, the old media was discarded and l-(4,5-dimethylthiazol2-yl)-3,5-diphenylformazan (MTT) was added to each well (final concentration 400 mg/mL).
• Incubation at 37 °C for 4 h allowed reduction of MTT by viable cells to an insoluble formazan product. Well contents were aspirated and formazan solubilized by addition of DMSO.
• Absorbance was read on an Anthos Labtech systems plate reader at 570 nm as a measure of cell viability; thus, drug toxicity was determined. ROS determination in Pterocarpuss santanlius
• The Total Reactive Oxygen Species (ROS) Assay Kit includes the necessary reagent and buffer for flow cytometry in the FITC channel to identify ROS in cells. The production of reactive oxygen species (ROS) in cells, is dramatically elevated during stressful situations, resulting in oxidative stress.
• Adherent cells were plated overnight in growth medium at a density of 5 x 105 – 10 cells/mL.
• Cells were treated with test compounds in PBS or HHBS. For untreated cells, equivalent amount of compound buffer was added.
• ROS production was induced by incubating cell plate at room temperature or in a 37ºC/5% CO2 incubator for at least 15 minutes, or required time for compound.
• ROS Deep Red Stock Solution 1 µL of 1000X was added to 1 mL of cells and was mixed well
• Fluorescence increase was monitored with a flow cytometer at Ex/Em = 650/675 nm (FL4 channel).
Cell Apoptosis DAPI Detection Kit DAPI
(4, 6-Diamidino-2-phenylindole) is a kind of specific dye for binding DNA. The ability of permeability for dye is increased during apoptosis, and apoptotic cells exhibit a high blue fluorescence. At the same time, for normal cells, nucleus is homogeneously stained and have a distinct edge. However, the nucleus edge is abnormal in apoptotic cells, and the condensed chromosome is easily stained.
• DAPI was diluted to 2 µg/ml work buffer by adding 90 ml of methanol.
• For Adherent cells, cell media was discarded on the cover slip. DAPI work reagent 500 µl was added to wash once. Then, DAPI work reagent was discarded.
• DAPI work reagent 500 µl was added and incubated at 37o C for 15 minutes
• The work reagent was discarded and cells were fixed using methanol.
• Glycerol or buffer A on cells was placed.
• Wavelength at 340/380 nm of excitation was observed by fluorescent photometer.
Conclusion
The phytocompounds present in P. santalinus has anticancer and wound-healing properties. The therapeutic properties of phytocompounds present in P. santalinus extract appear to have a concerted mode of action and conferred protection against various disease complications. Finally, the current review provides the evidence to enable other researchers to use P. santalinus as an efficacious natural drug. Further preclinical and clinical studies for adequate evaluation of the safety and therapeutic efficacy of P. santalinus are recommended. However, our findings are on benign tumour, the antitumorigenic property of P santalinus extract on malignant tumour still needs to be validated.
References
- Actis ML (2016) Identification of the first small-molecule inhibitor of the REV7 DNA. Bioorganic & Medicinal Chemistry 8.
- Agarwal R (2003) Ovarian Cancer: Strategies for Overcoming Resistance to Chemotherapy. Nature.
- Alahari S (2013) Micro-RNA in cancer.
- Budiana IN (2019) Ovarian cancer: Pathogenesis and current recommendations for Prophylactic surgery.
- Calin G (2006) MicroRNA signatures in human cancers. nature review cancer.
- Cui T (2015) XPC inhibits NSCLC cell proliferation and migration by enhancing ECadherin expression. oncotarget.
- Han C (2014) DDB2 suppresses tumorigenicity by limiting the cancer stem cell population in ovarian cancer. Molecular Cancer.
- JS Berek (2003) Epithelial ovarian cancer, In holland cancer medicine.
- Kang J (2011) miRNA-99b act as a tumor suppersor in nonsmall lung cancer by directly targeting. Experimental and therepeautic medicine.
- Khan A (2019) Role of miRNA-regulated cancer stem cells in the pathogenesis of human malignancies. Cells 8: 840.
- Khan S (2013) miR-379 Regulates Cyclin B1 Expression and Is decreased in breast cancer. plos one.
Artcle Information
Review Article
Received Date: November 28, 2021
Accepted Date: December 28, 2021
Published Date: December 30, 2021
American Journal of Cancer Research and Oncology
Volume 1 | Issue 1
Citation
Rashi Srivastava, Stuti Bhatnagar, Rajesh Saxena (2021) Anticancerous Properties of Pterocarpus santalinus. Am J Cancer Res Oncol 1: 1-7
Copyright
©2021 Rashi Srivastava. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: ajco.2021.1.101