

Case Report
Volume-3 Issue-1, 2026
Subarachnoid Haemorrhage (SAH) from Traumatic Head Injury in a Rugby Player
-
Received Date: January 05, 2026
-
Accepted Date: January 13, 2026
-
Published Date: January 30, 2026
Journal Information
Switch to Full Text Menu
Abstract
Key words
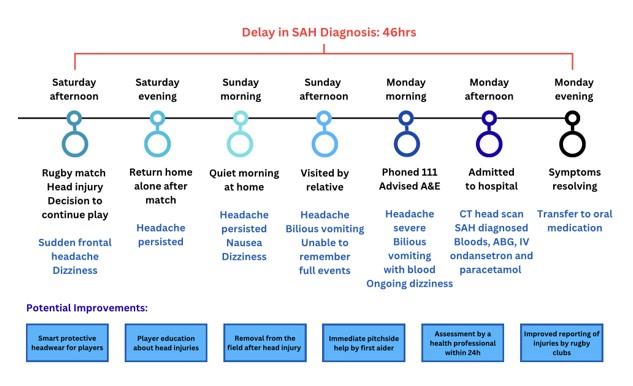 |
| Figure 1: Timeline of Events |
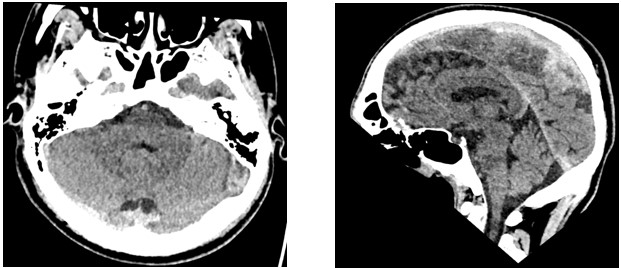 |
| Figure 2: CT Head Images |
Traumatic head injuries in rugby are a significant and growing health concern. Amateur players appear particularly vulnerable, with higher match injury rates than professionals [16] and tackling responsible for up to two thirds of head injuries Roberts, 2014. This report describes a case of traumatic subarachnoid haemorrhage (tSAH) sustained following a head injury secondary to tackling in an amateur game. It highlights concerns regarding rugby safety standards and underscores the importance of immediate pitch-side assessment, early healthcare evaluation and improved player education regarding the risks of continued play after head injury, in preventing morbidity and complications from traumatic subarachnoid haemorrhage.
Introduction
Traumatic head injuries in rugby are an increasingly prominent public health concern. An incidence rate of 37.8 per 1000 player-hours is reported [6], with longer-term risks of chronic traumatic encephalopathy (CTE) and dementia linked to rugby career length and repeated trauma [20]. CTE is reported in 68% of those with an 18-year playing history [21], raising concerns of a hidden epidemic of neurotrauma [13]. Recent litigation involving more than 1100 former players against rugby authorities [24] has increased scrutiny and public awareness of such risks. This report examines a case of tSAH following head injury in a club rugby player, exploring how rugby safety standards may fall short in the amateur game, causing delayed hospital presentation and increased morbidity.
Traumatic subarachnoid haemorrhage is a rare, potentially life threatening complication of head injury. It may arise from bleeding associated with cerebral contusions, arterial dissection, direct injury to small cortical vessels, or via a sudden increased intravascular pressure leading to vessel rupture and accumulation of blood between the arachnoid and pia mater. While prognosis from traumatic SAH is more favourable than aneurysmal SAH [11], cognitive deficit may occur [10] with rehabilitation required. Early recognition and neurosurgical assessment are therefore critical.
Case Report
A 25-year old rugby union player sustained a blow to his head from another player’s knee in a legitimate tackle, in a local league match. He experienced a sudden frontal headache without loss of consciousness and was encouraged to continue playing. His symptoms persisted throughout the afternoon and evening, and by the next morning he felt dizzy and nauseous. 24 hours after the match he began vomiting and was unable to recall fully events of the game. He had no photophobia, diplopia, neck stiffness or muscle aches (meningismus). He presented to A&E 46 hours after his injury due to persistent headache and vomiting, as shown in the timeline in Figure 1.
On arrival at A&E, the player was haemodynamically stable with a Glasgow Coma Scale (GCS) of 15. No other musculoskeletal injuries were present and a past history included only previous rugby concussions treated with conservative measures. He had no genetic, metabolic or hypertensive co-morbidities that increased his SAH risk, nor family history of SAH or aneurysm. He was a non-smoker, with normal body mass index and no history of excess alcohol or illicit drug use. He reported six previous episodes of concussion but without lasting consequences.
Examination revealed that he was conscious and orientated, with stable vital signs, a patent airway and full neck movements without pain. His cardiovascular, respiratory and abdominal examinations were unremarkable. Neurology assessment revealed bilateral brisk pupillary reflexes but no altered consciousness, meningismus, extraocular findings or focal neurological features. The motor exam was unremarkable in all four extremities, and he had intact sensation to light touch in his upper and lower extremities. Cranial nerves were intact, limb power was full bilaterally, and there was no aphasia or loss of visual field.
An initial full blood count, serum electrolytes, liver function tests and blood gases were normal. 1g IV paracetamol, ondansetron 4mg IV and NaCl 0.9% was administered via a cannula, with oral codeine 30 mg subsequently once vomiting had subsided. A CT head scan revealed small volume hypertense collection of blood at the left posterior vertex, in keeping with SAH. No mass lesions or midline shift was seen, and there was no evidence of overlying fracture. There was no hydrocephalus or acute infarct, and imaged orbits were normal. Paranasal sinuses and mastoid air cells were aerated with no calvarial fracture.
The player was admitted to hospital. Neurological observations were undertaken every four to six hours, and his pain was managed with paracetamol and dihydrocodeine. He remained alert and orientated, with a GCS of 15. His headache and vomiting resolved conservatively and he was fit for discharge the following day with oral analgesia and antiemetics, and safety netting to return if he became unwell, with worsening headache, vomiting, numbness, paraesthesia, reduced limb function or visual disturbance.
SAH prognosis is variable according to its cause, severity and the presence of complications or other injuries. Isolated mild traumatic SAH has a lower mortality rate (0-2.5%) compared to severe traumatic brain injury with SAH (15-40%) and aneurysmal SAH (30-50%) [16]. Traumatic SAH is typically managed conservatively with neurosurgical intervention rare (<1%) [15]. Seizures, vasospasm, hydrocephalus, raised intracranial pressure and death may occur, with age, lower initial come scale, extensive SAH, intraventricular haemorrhage, anticoagulation or antiplatelets predicting poorer outcomes [8]. Traumatic SAH in the basal cistern or Sylvian fissure carries a higher risk of late deterioration [6].
Discussion
Rugby remains one of the most widely played contact sports worldwide, yet traumatic head injury continues to pose a substantial clinical burden. Head and neck injuries account for 12-33% of rugby injuries (Brooks, 2008, Bathgate 2002), with higher rates reported in amateur players. Each year of rugby play adds 14% chronic traumatic encephalopathy (CTE) risk due to repeated brain damage [21].
Four types of intracranial haemorrhage occur after head trauma; epidural haematomas between the skull and the dura mater are associated with a skull fracture and an arterial tear, typically the middle meningeal artery. In subdural haematomas bleeding between the dura and arachnoid mater, occurs from torn bridging veins. Subarachnoid bleeds arise due to injuries to surface vessels on the brain and can be treated conservatively unless vascular anomalies are present. Intracerebral haematoma or cerebral contusion is characterised by bleeding in the parenchymal brain tissue itself. Contusions or bruises of the brain coalesce to form larger haematomas. All intracranial bleeds may be fatal and require prompt recognition and assessment, as death from bleeding may occur before the athlete reaches hospital.
This case highlights the importance of listening to athlete’s symptoms [14] and of urgent neuroimaging for key symptoms after head trauma: persistent headache, vomiting, dizziness, memory loss, altered consciousness, dizziness, seizures and subtle clinical signs, including brisker pupillary reflexes. It demonstrates how delayed symptom recognition, continued play after injury, and delayed hospital presentation may increase clinical morbidity.
England Rugby Guidance stipulates that every rugby club and event organiser must have a first aider per match or that live risk assessment must occur, with injuries reported via the Reportable Injury Event Form, via the Proactive App or RFU Injury Reporting Helpline [17]. The Rugby Safe HEADCASE guidelines [17] state that players should be removed from the field after head injury and assessed immediately by an appropriate healthcare professional or via 111. Where ‘red flags’ exist, urgent medical assessment via hospital A&E calling 999 is encouraged. Pitch-side support was absent at this match, full, immediate assessment was not undertaken and presentation to A&E was markedly delayed, increasing clinical risk, and raising concerns about safety standards in amateur rugby settings.
Conclusion
Head trauma and intracranial haemorrhage occur in rugby despite adherence to correct tackling techniques. This case highlights a delayed presentation of traumatic SAH and the importance of pitch-side assessment, mandatory removal from play, early medical evaluation and consistent safety provision in amateur rugby, to prevent complications.
This player reported multiple traumatic head injuries involving others at his club in the preceding week before his injury. He advocates for lower permitted tackling heights, advanced protective headwear technologies, improved head injury player education and club reporting of injuries to drive rugby safety standards. He has retired from rugby playing after his experience.
References
- Bjelanovic L, Mijatovic D, Sekulic D, Modric T, Kesic MG, et al. (2023) Injury Occurrence in Amateur Rugby: Prospective Analysis of Specific Predictors over One Half-Season.
- Bmj com (2025) Subarachnoid haemorrhage - Symptoms, diagnosis and treatment | BMJ Best Practice US. [online] .
- Cantu RC (1996) Head injuries in sport. British Journal of Sports Medicine, 289-96.
- Cantu RC, Mueller FO (2003) Brain Injury-related Fatalities in American Football, 1945-1999. Neurosurgery. 846-853
- Cleveland Clinic (2022) Subarachnoid Haemorrhage (SAH) | Cleveland Clinic. [online] Cleveland Clinic.
- Cooke R, Strang M, Lowe R, Jain N (2022) The epidemiology of head injuries at 2019 Rugby Union World Cup. The Physician and Sportsmedicine, 51:1-7.
- English Rugby Union (2025) Pitch Side First Aid Immediate Care | Rugby Football Union. [online] Rugby Football Union. [Accessed 6 Dec. 2025].
- Griswold DP, Fernandez L, Rubiano AM (2021) Traumatic Subarachnoid Haemorrhage: A Scoping Review. Journal of Neurotrauma, [online] 39.
- King D, Hume P, Gissane C, Clark T (2016) Semi-Professional Rugby League Players have Higher Concussion Risk than Professional or Amateur Participants: A Pooled Analysis. Sports Medicine, 47: 197-205.
- Kwok G, Ngai K, Wong A, Lam SW, Vincent Yeung, et al. (2011) Long-term cognitive dysfunction in patients with traumatic subarachnoid haemorrhage: prevalence and risk factors. Acta Neurochirurgica, 154.105-111.
- Lee JJ, Segar DJ, Asaad WF (2014) Comprehensive Assessment of Isolated Traumatic Subarachnoid Haemorrhage. Journal of Neurotrauma, 31: 595-609.
- Marcolini E, Hine J (2019) Approach to the Diagnosis and Management of Subarachnoid Haemorrhage. Western Journal of Emergency Medicine, 20.
- Marshall SW, Spencer RJ (2024) Concussion in Rugby: The Hidden Epidemic. Journal of Athletic Training, [online] 36.
- NAGAHIRO S and MIZOBUCHI Y (2014) Current Topics in Sports-related Head Injuries: A Review. Neurologia medico-chirurgica, 54: 878-886.
- Nassiri F, Badhiwala JH, Witiw CD, Mansouri A, Davidson B, et al. (2017) The clinical significance of isolated traumatic subarachnoid haemorrhage in mild traumatic brain injury. Journal of Trauma and Acute Care Surgery. 83: 725-731.
- Rau CS, Wu SC, Chien PC, Kuo PJ, Chen YC, et al (2017) Prediction of Mortality in Patients with Isolated Traumatic Subarachnoid Haemorrhage Using a Decision Tree Classifier: A Retrospective Analysis Based on a Trauma Registry System. International Journal of Environmental Research and Public Health, 14.
- RFU (2023) Headcase Extended Guidelines. [online] RFU.
- RFU (2024) HEADCASE | Rugby Football Union. [online] Englandrugby.com.
- Roberts S, Trewartha G, England M, Goodison W, Stokes K, et al. (2014) EPIDEMIOLOGY OF HEAD INJURIES IN ENGLISH COMMUNITY LEVEL RUGBY UNION. British Journal of Sports Medicine, 48: 654-654.
- Roxby P (2023) Longer rugby careers linked to higher risk of brain injury - study. BBC News,24 Oct.
- Sobey R, Herald B (2023) Chronic traumatic encephalopathy risk increases with longer rugby careers, study finds. [online] Medicalxpress.com.
- Sousa Nanji L, Melo TP, Canhão P, Fonseca AC, Ferro JM, et al. (2015) Subarachnoid Haemorrhage and Sports. Cerebrovascular Diseases Extra, 51:46-151
- Stewart W, Buckland ME, Bobak Abdolmohammadi, Affleck AJ, Alvarez VE, et al (2023) Risk of chronic traumatic encephalopathy in rugby union is associated with length of playing career. Acta Neuropathologica, 146.
- Telfer A (2025) Rugby concussion lawsuit has more than 1,100 former players involved. BBC Sport. [online] 2 Jun.
- Ziu E, Mesfin FB (2023) Subarachnoid Haemorrhage. [online] Nih.gov.
Article Information
Case Report
Received Date: January 05, 2026
Accepted Date: January 13, 2026
Published Date: January 30, 2026
Subarachnoid Haemorrhage (SAH) from Traumatic Head Injury in a Rugby Player
Volume 3 | Issue 1
Citation
Catherine James, Nebil Behar (2026) Subarachnoid Haemorrhage (SAH) from Traumatic Head Injury in a Rugby Player. Eur J Case Rep 3: 1-6
Copyright
©2026 Catherine James. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: ejcr.2026.3.101