

Review Article
Volume-1 Issue-1, 2021
Intra-tissue Endoscopic Exploration Under the Skin of Living Patients. An Invitation to Rethink the Nature of Human Living Matter
Received Date: May 12, 2024
Accepted Date: June 12, 2024
Published Date: June 15, 2024
Journal Information
Abstract
The organization and architecture of living matter has never been definitively described and fully confirmed.
Intra tissue endoscopy provides novel, real-time observations of living tissues. It offers insights unavailable from traditional cadaveric studies, and provides valuable new information about the microanatomy, dynamics and organization of living tissues. This article meticulously documents the appearance, behavior, and mechanical properties of connective tissues within the living body. This challenges conventional anatomical teachings and offers a new perspective on the dynamic nature of human connective tissue. The authors hope that this original research will help identify specific areas for future research to build on these findings, such as exploring the implications for tissue engineering, regenerative medicine, surgical innovations, offering a new perspective on the dynamic nature of human connective tissue and opening the debate on a post-Vesalian anatomy.
Key words
Fiber; Intra Tissue Endoscopy; Living Matter; Cells; Mobility; Architecture; Extra Cellular Matrix; ECM; Fascia ; Connective Tissue; Network; Microanatomy; Tissue Continuity
 |
| Figure 1: (Top) A display of material used during surgical endoscopy: an endoscope with a high-definition Full HD camera, a flexible fiber optic cable with a cold light source, -(middle) Use of the endoscope during surgery. -(bottom) Viewing the video in real time on a screen in the operating theatre during surgical endoscopy. |
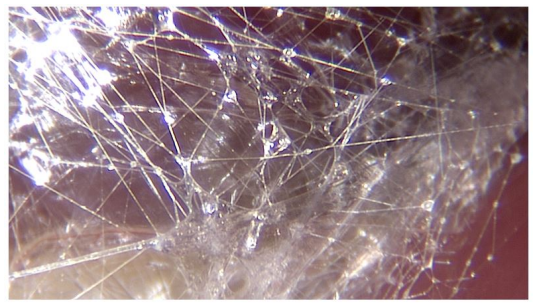 |
| Figure 2:A world of fibers. Fibers are everywhere, in every nook and cranny and by their intersecting create microvolumes |
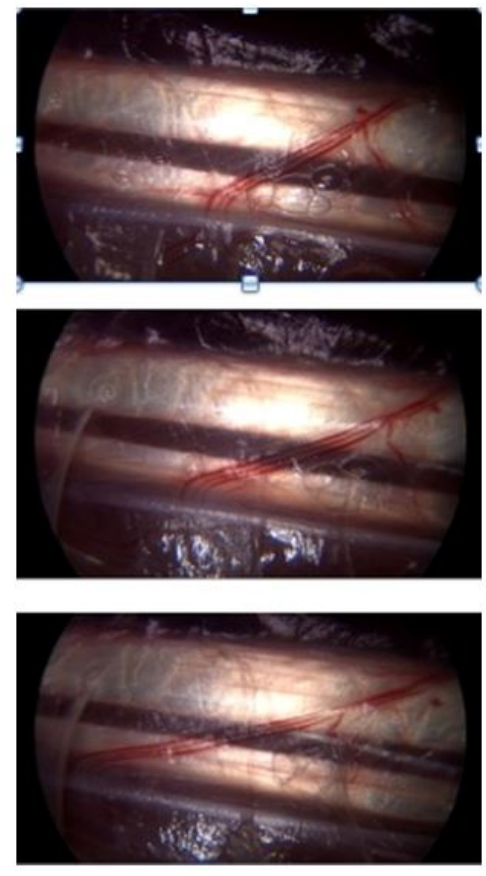 |
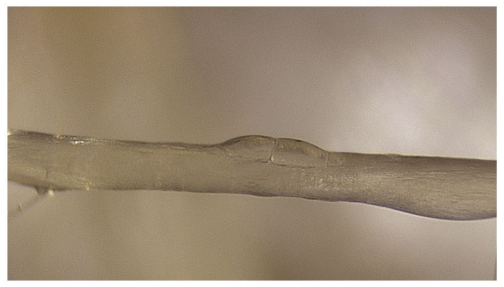
| Figure 3:The vessels of the peritendinous sliding network display different non-linear progression during movement within a homogeneous substance |
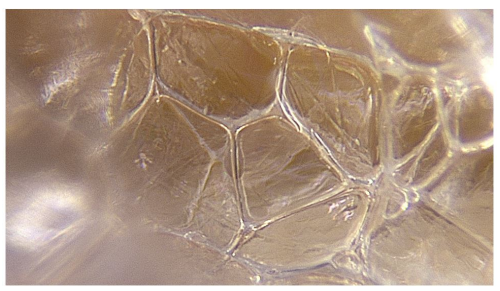 |
| Figure 4: The light emitted by the endoscope is reflected from the glistening facets of the microvolumes |
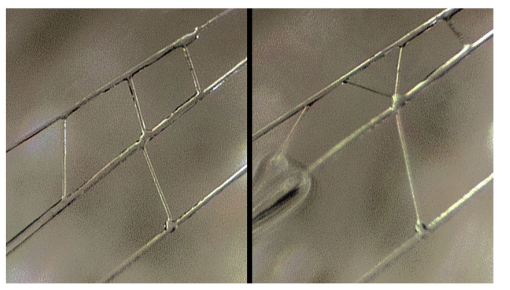 |
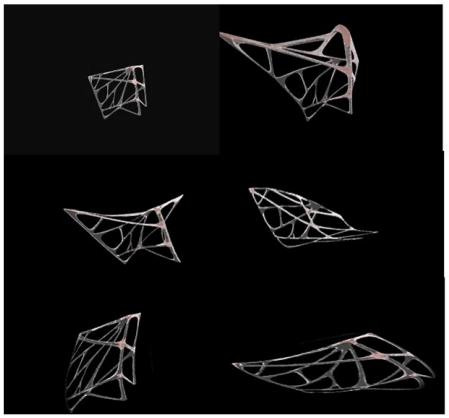
| Figure 5: The combined action of these three distinct, yet closely related, types of fibrillar behaviour enables the fibrillar network to adapt to the constraint in three dimensions |
 |
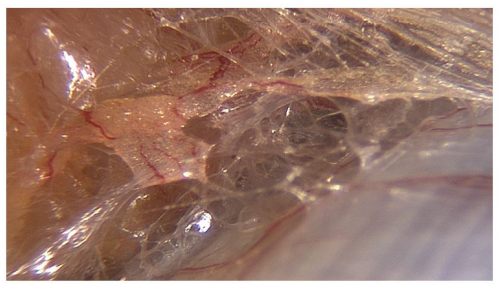
| Figure 6: Arterioles, capillaries, venules and nerves all make use of the multimicrovacuolar system for support. This accounts for their seemingly random pattern of distribution |
 |
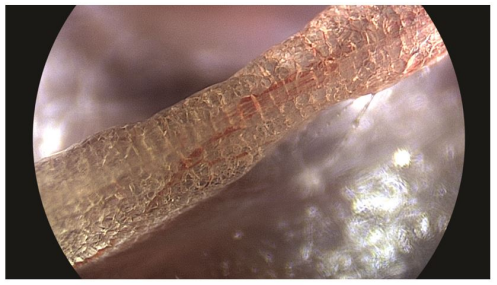
| Figure 7: Along the fibers, cells are found either in pairs, like ladybirds on a blade of grass, or in small groups |
 |
| Figure 8: Sometimes we see groups of cells called clusters and they contain several million cells |
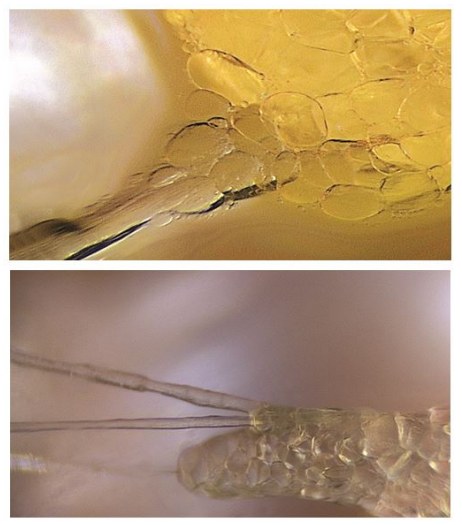 |
| Figure 9: Top. Cells appear to engulf and swallow the fiber -Bottom. Fibers penetrate inside the cluster of cells connecting the intracellular network. |
 |
| Figure 10: The fibrils are stretched under stress, the microvacuoles adapt to the constraint, and change shape The constraint is gradually diffused, dispersed and absorbed by the fibrillar network due to the capacity of the fibers to distend, divide and slide along each other |
Introduction
For centuries, the human body has been described in all its nooks and crannies, but anatomical research has been performed on cadavers, or by studying tissue samples under the microscope. This means that the study of living matter has been carried out on dead and inert structures.
The use of intra-tissue endoscopes with miniaturised high-- magnification cameras during surgical procedures has introduced a new method of observation with surprisingly different microanatomical conclusions. This unique and innovative exploration of the human living being covers 1305 cases.
This research allows us to conclude that the study of the living being, and the movement of living tissue introduces new perspectives because we are confronted with the global nature of the being and its vital processes. The traditional notion of the organisation of human living matter associating separate organs with a connective tissue packaging is transformed into a very different vision of a global fibrillar architecture extending from the surface of the skin to the cell nucleus, in which specific cells carry out specific functions.
The implications of this complete change of paradigm are multiple, especially in the fields of anatomy and therapeutics. It offers a new perspective on the organization of living matter and opens up the study of living matter by other scientific disciplines, while pointing towards a “post-Vesalian” period of anatomical research. Future scientific theories must be consistent with in vivo observation.
This article is the fruit of many years of surgical experience, of hours and hours of endoscopy, video-screenings, trying to understand how flexibility, sliding between organs, and fluid distribution can be explained.
When we massage, stretch, or lift the skin, we feel a little resistance to traction but the skin does not tear, and when we let go, as if by memory, it returns to its initial position. This ability to restore body shape and maintain our integrity tends to be taken for granted and does not get much attention.
In the twentieth century, anatomical studies have even tried to explain elasticity and plasticity from a mechanistic point of view by alluding to notions of virtual space, tissue layers and stratification of “connective tissue” [1-3].
Now, thanks to new technology, we can learn more about this connective tissue which has been neglected for so long.
The introduction of endoscopic exploration changes our perception of connective tissue and we are confronted with an unexpected microanatomy, new situations, colours, and a new perspective of life in motion
One conclusion of this unique exploration of human living matter at high magnification could be that attempting to understand the anatomy of a body by dissecting cadavers or isolated tissue fragments under the microscope in a histology laboratory would appear to be at times erroneous. In vivo observations are neither more nor less important, but complementary, and, in the light of this research, cannot be ignored.
Material and Methods
The authors lead an observational case series study comprising of two arms: human and animal subjects.
Intra-tissue endoscopy was performed using a video endoscope STORZ reference 26120BHA HOPKINS system 30° diameter 2.9mm, length 30 cm, HAMOU, magnifying respectively 60 times with a Karl Storz camera Image One connected to an associated cold light source Xenon Nova 201315.
The sequences were recorded with a video recorder KIPRO AJA HDV 10 codecs Linear PCM, Timecode, Apple ProRes 422.With this new technology, it is possible to obtain levels of detail never achieved before.
The time set aside for filming was limited to 10 minutes so that the work of the surgical team was not disturbed. These surgical interventions were performed either with or without a surgical tourniquet. The use of a tourniquet provides a bloodless field, which allows detailed observation. Many factors can disturb the filming process, namely, bleeding. The use of a tourniquet for the limbs is the solution but the pressure must not exceed 18 mmHg. Maximum stability is required to avoid jerking of the endoscopic lens.
The endoscope and the camera are not heavy, but the 20cm long endoscope transmits small vibrations of the operator, creating tremors. It is therefore necessary to stabilize the arms of the operator by leaning them on sterile rolls of Velpeau strips placed on the operating table. This provides stability and a certain flexibility with a plumb line that gives a better image quality. Finally, it is necessary to ensure the proper functioning of the recording material during filming, thus avoiding disappointment.
Some tissues are more opaque than others and while some provide the surgeon with superb images, others are totally unusable. It is necessary to clean the optical lens regularly because lipid particles, fog or droplets appear in certain patients very quickly. Finally, adjustment of the focal length with this equipment is done by means of a manual dial, and the depth of field being very small, images become easily blurred.
Statistics
First arm of the study: Human subjects.
The inclusion criteria were:
● Men and women aged 18 years or over.
● Scheduled for routine elective upper limb, lower limb, abdominal, lumbo-sacral or scalp surgery in a conventional surgical setting.
● Affiliation to a social security scheme
● Signature of informed consent prior to any studyrelated procedures
● Ability to answer questionnaires and to communicate freely in French.
The exclusion criteria were:
● Any significant disease or disorder which, in the opinion of the investigating surgeon, may put the participant at risk because of participation in the study, or may influence the result of the study
● Pregnant or breastfeeding women
● Adult under guardianship, curatorship, or other legal protection,
100% of all patients accepted with written consent.
Given that the time allowed for endoscopic exploration was limited to approximately 10 minutes, the majority of surgical interventions selected - 95% of the cases - were those planned in advance. The consent of the aneasthiologists was always requested.
This intra tissue endoscopy thechnique is easily reproducible by any surgeon with the apropriate endoscope and a high-definition camera. To begin with, we recommend cases requiring surgery using a tourniquet on one of the limbs, to produce a bloodless field.
-Endoscopic exploration was carried out on a total of 1305 patients over a period of 15 years. An average of 90 intra tissue explorations were performed each year, spread over an average of 40 days a year. A total of 120 hours of recordings were made during this period.
10% of the explorations were interrupted due to the presence of steam or droplets at the end of the endoscope. No links were correlated with the pathology, sex, age or ethnicity of the patients.
-Tissue analyses were performed by Institut de Biologie et de Chimie des Protéines (IBCP)Université Claude Bernard Lyon 1. https://www.univ-lyon1.fr.
-Sex: Male 65%. Female 35%. Age: 10 to 82 years old
-Localisations:
● Forearm 28% • Elbow18% • Abdomen• 15% • Hand 19% • Thorax 13%
● Lumbar and sacral part of the back 4% • Lower limb 3% • Scalp 1%
Second arm of the study: animal subjects.
42 dissections.
Rats: 23 cases dissected in lower limbs and thorax.
Rabbits: 11 cases in face and lower limbs.
Turkeys: 8 cases in lower limbs. All cases were performed in an accredited university experimental anatomy laboratory.
Informed Consent
Patients
Internal ethics committee of the Institut Aquitain de la main, 56 Allée des Tulipes Pessac 33600.
A consent form was signed by each patient authorizing the taking of images not subject to the first and second paragraphs of article 9 of the Civil Code, article 226-1 of the Penal Code and other points of the Public Health Code, insofar as these images concern the inside of the person at the meso and microscopic level.
The person is not recognizable or identifiable. All patients (100%) gave their consent.
Animals
Department of Applied Surgical Techniques and Research. DETERCA
Victor Segalen University of Bordeaux 2 146 rue Léo Saignat 33076 Bordeaux cedex. Regulated by European Council Directive no. 86-609-CEE of 24 November 1986. Implementing decrees: 1st Order of 19 April 1988.
Observations
We now describe what we observe during intratissular endoscopy at different levels of magnification [4-9].
Naked Eye
a) Colors and Moistering
Living matter is beautiful and you can see a vast range of colors such as bright reds, navy blues, pale or golden yellows, silvery or pearly whites, mauves, and purples.
Another striking feature is the moistening of the tissues as soon as a surgical incision is made. Without a tourniquet, bleeding occurs immediately and hinders observation of the tissues. But even when a pneumatic tourniquet is applied so as to obtain a clear bloodless field, fluid exudes from the wound and trickles along the sides of the incision. This is evidence that the underlying tissues are permanently hydrated.
b) Tissue Tension
The edges of a surgical skin incision draw apart spontaneously and a phenomenon of retractile invagination of the epidermis can be seen. This illustrates that our body structures are under permanent, endogenous tension.
When you cut through skin or aaponeurosis, the edges are drawn away and it is difficult to bring them together again to repair the incision with sutures.
We observed the same phenomenon with tendons, muscles, and even nerves and arteries. All surgeons observe tissue tension in living organisms when it comes to suturing.
c) Fibers
To the naked eye, connective tissue seems at first to be fairly uniform, whitish and of little interest to the anatomist. But we are struck by a real entwining and interweaving of opalescent fibers at the microscopic level of observation. It is important to emphasise that this tissue is present everywhere within the body, linking separate structures.
It is called « packaging tissue » or SubSynovial Connective Tissue (SSCT). It could also be called “fascia”, described by Still [Ref.10-11] and by osteopaths. Another important observation is that you cannot distinguish areas of "virtual space" between anatomical structures, as described in anatomy textbooks. Everything is connected.
Magnification X 10
a) Disorderly Pattern
If one grasps and pulls the tissue with tweezers, we immediately find this multi-fibrillar organization, surprising because it is a network arranged in a completely disorderly fashion with no apparent logic.
Sharp traction causes curious movements to occur due to the bursting of microvacuoles at atmospheric pressure, demonstrating the existence of hydraulic systems under different levels of pressure.
b) Diversity
These fibers and fibrils may have quite large diaphanous surfaces, reflecting sharp edges but they can also be narrow, long or short, swollen or cylindrical. Diversity is everywhere and there is endless variety.
The fibers divide into smaller-diameter fibrils of a few microns to a few dozen microns in diameter with extremely variable lengths of 20 to 100 microns and of irregular thickness, giving a disordered and chaotic appearance – like a latticework of stems. We observe long or short fibrils, that are either vertical, oblique, or transverse; close together or far apart, and of varying density.
c) Force Absorption System
This fibrillar network seems to favor optimal sliding.
If we look for example, closely at the flexor tendons in the palm of the hand, we can observe two things; the wide variety of vessels around the tendons and the fact that, during movement of the tendon, there is no dynamic repercussion of the movement at the skin surface or in neighboring tissue, which remains stable.
If we analyse the images in figure 3 more closely, we observe that during flexion, the two large vessels diameter (150 microns) are indeed moving apart. However, compared to the smaller vessel, (30 microns) not only does the larger vessel move faster, but the two vesssels move at different speeds. We know this because the distance between them has doubled.
We can conclude two things.
- There is therefore obviously some kind of force absorption system.
- There are several forms of speed and progression.
How can this be explained?
Due to the influence of reductionist linear thinking, the only rational explanation was that of annular layers sliding together, necessitating the existence of a hierarchical tissue distribution. In vivo observation has rendered the notion of distinct laminated layers with stratified strips neatly stored next to each other unacceptable.
d) Flux of the blood and extracellular liquids
Droplets observed at this level of magnification are due in part to the condensation of the fluid atmosphere of the tissues under the cold light of the endoscope and the illumination of the surgical headgear, but this explanation is not sufficient because it is not observed in all patients.
The majority (65%) of cases provide superb photos and videos. However, about 25% of patients emit a fog a few seconds before the appearance of droplets, and about 10% are found to have more opalescent tissues. These phenomena alter both the quality of photos and their colors.
e) Ubiquity
This fibrillar chaos is found throughout all our surgical exploration fields. It is observed in, the abdominal wall, in contact with the thorax, in the retro-orbital area, lower limbs, upper limbs, back, scalp, and so on. All tissue types are concerned; skin, hypodermis, aponeurosis, tendons, nerves, arteries, veins, periosteum, bones.
The resulting fibrillar continuity ensures simultaneous movement and sliding in the fingers, hands, legs and shoulders, ensuring the return of anatomical structures to their resting position after movement, while at the same time modulating nervous or vascular input and constantly maintaining the pre-ordained shape of our bodies.
Magnification X60
This level of magnification provides further valuable – and at times - surprising information.
a) Architectural continuity, fibrillar intertwining and microvolumes
We have already observed strange displays of sparkling, scintillating, mobile mirrors and ephemeral lights which can change shape during movement at the mesoscopic level.
This gives rise to the notion of microvolumes or “microvacuoles”; volumetric units that exist within a continuous architectural network of intersecting irregular fibrils chaotically disposed, framing liquid-filled three-dimensional volumes.
They are revealed because air at normal atmospheric pressure has entered them, diffusing across their walls. This concept is fundamental because it introduces the idea of a pressurised volume. This phenomenon is not observed in a cadaver or in preserved tissue.
The exploration of these microvolumes reveals a world constructed solely of interlacing fibrils - a real tangle of threads of different sizes, with apparently no directional coherence - giving an overall disorganized chaotic aspect.
These micro-fibrils framing microspaces have a diameter of about 10 to sixty microns.
The sides are composed of collagen fibers, mostly type 1 (23%), 3 and 4.
These microspaces contain a hydrated proteoglycan gel (70 %). Their lipid content (4%) is high. As a result of their strong negative charge, glycosaminoglycans attract counter-ions and water molecules into the tissue.
In the sliding areas, the multi-micro-volumes ensure two dynamically opposed roles; an absolute dynamic role and total absorption, combined with the inherent ability that allows the tissues to return to their original form.
How does this readily observable fibrillar chaos ensure tissue cohesion, preserve volume, while ensuring adaptability and mobility, including the accuracy and precision of movement?
The answer could be found in the following endoscopic observations:
b) Mobility of Fibers
These videos are fundamental because they show the morphodynamic capacity of the fibrils. In an instant, under a slight constraint, three types of fibrillar movements takes place: sliding, division, and stretching.
To be achieved, these three types of movements involve the intrinsic properties of the fibrils.
Closer scrutiny reveals that ringed superpositions between the fibers become distended just before the overall movement ensues. This could be the first stage. Secondly, the biomechanics of the fibers are assisted by the capacity to migrate around a nodal point, along another fiber.
Finally, fibers also seem to be able to dissociate into several branches, appearing to split and then reform.
And when one considers that all these myriads of seemingly random micro movements occur instantly on millions of fibers, it becomes clear that these properties of living matter and its spatial organization, offer an infinite potential of movements.
Highly effective, pre-stressed, flexible fibrillar structures are undoubtedly advantageous due to their ability to adopt various forms, being more stable and more adapted to sliding between themselves. However, not all these fibers are mobile. Form has to be maintained. Some are fixed, with stable junctions.
c) Fibers Instant Dynamic Fractalisation
Furthermore, there is another observation that is unavoidable during endoscopic exploration. This is the observation of the phenomenon of fractalization. Fibers and fibrils are able to divide into sub-fibrils. In this way, force is dispersed throughout the structure rightdown to the molecular level. A fractal structure looks similar whatever the scale under which it is examined. This property is called self-similarity. Fractal structures display regularity within their irregularity, and this adds another dimension to the chaotic aspect of living matter.
Fractalisation is a widespread phenomenon in anatomy. In this way, a large surface can be contained within a small volume, thus providing a larger surface area for exchange.
This the case with the alveoli in the lungs but also the intestinal villi. We find similar arrangements in tendons. It is important to note that the irregular fractalisation within this network is not inert; it is dynamic.
d) Cells and fibers
It is not easy to observe cells in the epidermis and the dermis. Muscle cells are also difficult to observe. Melanocytes which are easily identified by their brown colour, can be seen deep inside the epidermis just above the papillary ridges.
It is in the hypodermis that the cells become more obvious. The adipocytes within the fatty lobules are easy to see. Fibrocytes can also be easily observed in the sliding areas around the tendons where the tissue is less dense and more supple. The fibers are woven more loosely in these areas and clusters of cells can be identified between or on the fibers. Cells in their millions can be seen in these areas on the surface of the muscles, tendons, nerves and veins. We have not been able to discern any apparent logic in their arrangement. The disposition of these fields of cells is perplexing. The outer limits of the groups of cells are sometimes regular, but sometimes not at all, often spreading over large distances with areas completely devoid of cells.
Cells tend to concentrate around the vascular axes leaving unoccupied spaces elsewhere. Nevertheless two things are certaint. The cells move with the vessels during movement and exhibit tropism towards the vessels.
The cells fit into this fibrillar network perfectly, and have similar dimensions, ranging from 10 to 60 μm within the microvolumes. Cells are sensitive to external conditions and need some kind of architectural support in order to survive and function. Cells do not exist in isolation.
e) Cell migration
During exploration, the endoscope sometimes reveals a small group of cells that seem to be gathered at a distance from the main group. They appear to be nomadic. Cells thus observed are located along the axis of the fibers of the network and seem to use the fibrillar network to migrate.
f) Cells and energy distribution
Cell nuclei have never been observed as they are naturally transparent.
At the cellular level we sometimes see a pericellular capillary network. Each cell is surrounded by a tiny capillary vessel of a few microns in diameter. Surprisingly, in some areas this applies to all cells but in others only a few cells are encircled in this way.
The vascular supply follows the path of the multimicrovacuolar structures. The enormous advantage of this arrangement is that the cellular and extracellular elements receive a continuous, uninterrupted supply of energy and information, even during movement, because when the fibrillar scaffolding moves, the vessels move with it. There is no rupture in the supply line.
g) Sub-aponeurotic Clusters of cells
Clusters of cells can be easily identified in this sliding area situated beneath the hypodermis and above the aponeurosis. The grouping together of cells in this way is a captivating discovery. They are often oblong in shape, and generally well vascularized by a central arterial branch and its ramifications but this is not a constant observation. There is a large variety of shapes and sizes, ranging from about 500 to 1500 microns. The number of cells in each cluster depends on the its length. A cluster of 2 mm contains at least 5 million cells.
h) Relationship between fibers and cells
This does not appear to be a simple contiguous relationship. The cells do not simply sit on the fibers. Things seem to be much more complex.
The cells are as wrapped within this network. But the term wrapped or swathed, implies a physical separation whereas in fact there is total continuity. A mesh of interlacing fibrils penetrates a group of cells and the fibrils extend into the intercellular membranes. There is a real and total histological fusion between these two elements. Cells appear to engulf and swallow fibrils.
These two elements, the cell and the fibrillar architecture form a structural continuum.
However, not all fibers are colonized by cells. The relationship between fibers, cells and vessels is undeniable and can be perceived as fusional and global.
i) Fibrillar network has a mechanical influence on cells
This has two essential consequences. The first effect is on the behavior of the cells whose shape and position depend on the mechanical behavior of the fibers.
Cells move, change their appearance, dilate, or sag a little in reaction to the slightest mechanical impulse.
The endoscopic observations made in vivo show structural elements that are difficult to identify during cadaveric dissection or the study of preserved tissue samples, and lends support to conclusions which question our academic certainties. 8 films showed this new world being explored. [15] and a specific website [16]
Discussion
General Anatomical Conclusions
1) Tissue continuity - no layers, no empty spaces
Ubiquitous Fibrillar architecture -
Contrary to conventional teaching [1.2.3] we now discover that there are no empty spaces, no separate layers of tissue sliding over each other. This continuum of fibers, which is present in all spaces throughout the body, is what we call connective tissue or extracellular matrix, ground substance and interstitial spaces. The connective tissue network exists throughout the body, from the macroscopic to the microscopic level, providing both fibrillar and histological continuity. It is a true architecture.
The global and continuous nature of connective tissue within the body is evident from these endoscopic observations. But does this tissue, which we call connective, have only a connective role?
2) The organization of living matter in separate layers is an obsolete perception.
The body cannot be considered as a machine made up of separate parts, or like a cake with icing between separate layers. The concept of layers, strata, separate planes is obsolete and needs to be replaced by the observable reality of a single, common fibrillar network inhabited by cells with different densities that gather together to perform specific functions. Our anatomy textbooks still describe highly stratified layers of tissue. The anatomy described by Vesalius and our elders must now be reconsidered in the light of current scientific thinking that integrates life sciences with modern physics and new mathematics.
3) We are made of microvolumes at all scales
The concept of irregular polyhedral network
The observation of living structures at a magnification of X10 or X25 [Figure 5.6.7.8] reveals a mesh, a woven network, resulting from the intercrossing of fibres in three dimensions, creating repetition of an irregular polyhedral volumetric unit that could be named “the microvacuole”. The shape of the microvacuole is polyhedral; completely irregular, yet simple. Each microvacuole has its own form. It is important to emphasise that everything in this extracellular world tends to be irregular and polyhedral. However, these are simple shapes. This is a constant, unvarying observation.
These microspaces are variable in size, ranging from 10 microns in the peritendinous region to 100 microns in the abdominal preaponeurotic region can be filled with fluids for a shock absorbing role or by cells.
4) Cells are not the only ones responsible for tissue continuity and form [12]
The cell is sensitive to external conditions and needs some kind of architectural support in order to live and function. Sometimes cells are too scattered to influence the shape of anatomical structures and are not responsible for tissue continuity and form. The fibrillar network is ubiquitous, found everywhere in the body. It is a global system and not only one more organ. All the organs in the body share the same basic fibrillar framework, of course with different architectural features.
5) We are a global fibrillar architecture. Connective tissue is the Constitutive tissue
A new paradigm and not a new organ
So, if there is total fibrillar continuity from the cell to the surface of the skin, and if this is true throughout the body, it is logical to see a relationship between this continuous fibrillar network and the resulting form, and to consider human ontology from a new perspective, thereby proposing a new paradigm. Connective tissue is in fact the constitutive tissue. It does not link the different parts together. It is the global frame, in which the parts develop.
The concept of tissue layers, neatly arranged in strata, compartments and sheaths, is helpful when learning and teaching anatomy but in reality, these layers do not exist. A real structural ontology can be worked out with a basic functional unit, which is the micro-vacuole, the micro-volume responsible for the form and the dynamics of the living body.
6) A hitherto unobserved optimal fibrillar biomechanical behavior [13]
This mechanical behaviour has two aspects: ensuring complete movement and preserving peripheral tissue stability while at the same time accommodating both these parameters.
The fibrillar framework - a flexible, pre-stressed, polygonal architecture, is able to assume many shapes without rupture, thereby enabling stability and sliding, leading to a more efficient metabolism and therefore prolonging life. This tendency to irregular geometric forms is intriguing since it is to be found at all levels of living matter, and would seem to be the building block that has developed in nature during the course of evolution.
- A combined, transmitted and absorbed stress mechanism
We refer to this notion as “combined transmitted and absorbed stress” i.e., each fiber is prestressed and connected to its neighboring fiber. When tension is applied to the link, the adjacent element undergoes tension and decreases in size little by little until deformation occurs. All of the component parts then align themselves so as to be oriented as far as possible in the direction of the applied force, which during this research was controlled in order to avoid rupture.
The fibers rearrange themselves in response to the local stress, thereby explaining the final linear stiffening resulting from the application of the stress: as the stress increases, the fibers become more aligned in the direction of the stress. However, the energy stored in the fibers under tension gradually becomes lower, the greater the distance from the stress, so the forces resulting from the linear stiffening are absorbed and the structures become stabilized. The fibrils are stretched under stress, the microvacuoles adapt to the constraint, and shape change. The constraint is gradually diffused, dispersed and absorbed by the fibrillar network due to the capacity of the fibers to distend, divide and slide along each other.
7) Unpredictibility, irreversibility, complexity. Mechanical behavior seems to be optimal, but is unpredictable, prepared to deal instantly with any constraint imposed on it, and so each movement is unique.
The fibrillar movements within the multifibrillar network clearly have a functional finality, which is mobility.
Fibers undergoing mechanical stimulation can stretch, become longer by adjusting their contours. The fibers can also divide into several other fibrils, which themselves disperse and absorb forces efficiently.
Moreover, some fibers are able to glide along each other. This indicates the existence of a three- dimensional mechanical system in constant search of equilibrium. This is a completely new discovery of the movement of fibers and fibrils in 3 dimensions, providing unexpected solutions for the required movement in an instant and a previously unobserved mechanism. It appears to be constant and never ending. It is also flexible, adaptable and interactive. There is no tearing or sectioning of fibers.
The system is prepared to deal instantly with all internal or external mechanical constraint and is impossible to anticipate or predict. This brings to mind quantum mechanics.
If we think about it, the combination of these movements at a specific time and place will never be repeated.
On the other hand, it is impossible to ignore the role of Glycoaminoglycanes in response to traction. Their role is no doubt lubrication and nutrition but also to absorb pressure.
Conclusions
In vitro observations are obviously not the same as in vivo microanatomical endoscopic observations of living tissue.
The body seems to be an ideal mesh, made of fibres, fibrils and micro-fibrils, and micro-volumes, in which different cellular specificities are embedded. A real structural ontology can be proposed. In this way, the global and continuous living form can be described and interpreted.
These explorations and this concept open the world of living matter to new areas in physics. This embraces fractal organisation and non-linearity, and enters the realms of disordered systems, self organisation and the science of complexity. They encourage us to attempt to understand fibrillar dynamics, initiating new mechanical perspectives through a model of intervector exchanges that has never been tested or described. From a medical perspective, they encourage surgeons to reduce surgical incisions and develop surgical endoscopy.
Through our work, we believe that we are participating in the search for a new rational explanation of human nature and are paving the way towards a new, postVesalian anatomy [14].
No Conflict of Interest
Financial Support
No funding was received for this work. It was carried out entirely on a voluntary basis.
References
- Gray H (1858) Anatomy Descriptive and Surgical. London: John W Parker and Son
- Ragan C (1952) The physiology of the connective tissue (loose areolar). Annual Review of Physiology, 14: 51-72.
- Richet A (1877) Traité pratique d’anatomie 5th ed. Paris: Chamerot et Lauwereyns.
- Guimberteau JC (2005a) La mécanique du glissement des structures sous cutanées chez l’homme. Mise en évidence d’une unité fonctionnelle: la microvacuole. E-Mem. Acad. Natl. Chir. 4: 35e42.
- Guimberteau JC, Delage JP, Wong J (2010) The role and mechanical behavior of the connective tissue in tendon sliding. Chir Main, 29: 155-66
- Guimberteau JC, Delage JP, Wong J (2010) New views about the skin. Ann Chir Plast Esthet, 55: 255-66
- Guimberteau JC, Delage JP, Sawaya E, The architectural behavior of the skin. Measuring the Skin. Springler.
- Guimberteau JC, Armstrong C, Architectures of Human Living Fascia The extracellular matrix and cells revealed through endoscopy. Hand Spring Editing. 13: 978-1-909 141-11-7.
- Still AT (1899) Philosophy of osteopathy. Indianapolis, In diana, US: American Academy of Osteopathy.
- Armstrong Colin (2020) The architecture and spatial organization of the living human body as revealed by intratissular endoscopy .An osteopathic perspective. Journal of Bodywork & Movement Therapies 24: 138e146
- Ingber DE, Prusty D, Sun Z, Betensky H, Wang N (1995) Cell shape, cytoskeletal mechanics, and cell cycle control in angiogenesis. J. Biomech, 28: 1471-84.
- Kapandji A (2011) Qu’est ce que la Biomécanique? Montpelier: Sauramps Médical.
- Vesalius Andreas (1543). De humani corporis fabrica libri septem.
- Films:
Guimberteau, J.-C., 2004. Promenades sous la peau ; Strolling
under the skin.
Elsevier-Masson, London.
Guimberteau, J.-C., 2005b. Strolling under the Skin. Endovivo Productions.
Guimberteau, J.-C., 2009. The Skin Excursion. Endovivo productions.
Guimberteau, J.-C., 2010. Muscle Attitudes. Endovivo productions.
Guimberteau, J.-C., 2012a. Interior Architectures. Endovivo
productions.
Guimberteau, J.-C., 2012b. Skin, Scars and Stiffness. Endovivo Productions.
Guimberteau, J.-C., 2017. Of Cells, Fibers and the Living Human Body. Endovivo Productions.
Guimberteau, J.-C., 2018. Homofasciaticus. Endovivo Productions. - s16. Endovivo . htpp//www.endovivo.com
Artcle Information
Review Article
Received Date: May 12, 2024
Accepted Date: June 12, 2024
Published Date: June 15, 2024
Journal of Bone Research and Orthopaedic Surgery
Volume 1 | Issue 1
Citation
Jc Guimberteau MD, T. Sawaya MD, C. Armstrong DO (2024) Intra-tissue Endoscopic Exploration Under the Skin of Living Patients. An Invitation to Rethink the Nature of Human Living Matter. J Bone Res Orthop Surg 2: 1-16
Copyright
©2022 Jc Guimberteau MD. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jbos.2022.2.103