

Review Article
Volume-1 Issue-1, 2021
Is Using Wire and Screw Technique Aid Reduction During Open Treatment of Condylar and Subcondylar Fractures
-
Received Date: June 20, 2022
-
Accepted Date: July 13, 2022
-
Published Date: Sept 09, 2022
Journal Information
Abstract
Objectives:To evaluate the use of wire and screw technique to aid reduction during open treatment of condylar and subcondylar fractures.
Methods: This study consisted of 10 patients divided into two groups, (five for each group). First group, the reduction was assisted through the use of (6 mm length - 2 mm diameter) screw, 26-gauge stainless steel wire, and 16-gauge needle. Second group, the reduction was performed using a towel clip and bone hook without stripping the lateral pterygoid muscle from its condylar insertion. The time of operation was calculated and clinical evaluation of complications had been done for both groups. Computed Tomography (CT) was taken to confirm the position of the reduced condylar fractures.
Results: All fractures had reduced into their normal position without developing series of complications in the 6-month follow-up period.
Conclusion: Using wire and screw technique for reduction of subcondylar fractures during the open treatment gives the surgeon the ability to move the fractured mandible as a bony anchorage through the reduction screw with minimal or no postoperative complications related to that technique of reduction.
Key words
Open Reduction; Wire and Screw Technique; Condylar Fracture
Patient No |
Operation time |
|
Study Group |
1 |
60 |
2 |
50 |
|
3 |
65 |
|
4 |
70 |
|
5 |
75 |
|
Control Group |
6 |
70 |
7 |
85 |
|
8 |
90 |
|
9 |
80 |
|
10 |
70 |
|
Patient No |
MIO |
Lateral extrusion to the right |
Lateral extrusion to the left |
Protrusion (mm) |
|
Study Group |
1 |
45 |
10 |
9 |
8 |
2 |
33 |
8 |
8 |
7 |
|
3 |
53 |
10 |
9 |
9 |
|
4 |
36 |
11 |
9 |
6 |
|
5 |
46 |
11 |
8 |
4 |
|
Control Group |
6 |
37 |
10 |
10 |
7 |
7 |
45 |
10 |
9 |
4 |
|
8 |
37 |
9 |
10 |
6 |
|
9 |
42 |
10 |
9 |
5 |
|
10 |
35 |
10 |
10 |
8 |
|
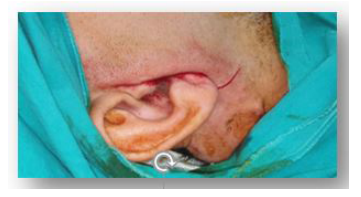 |
| Figure 1: photograph showing lazy (s) incision for the transmassetricanteroparoid approach |
 |
| Figure 2:photograph showing the intact parotid gland capsule after incision |
 |
| Figure 3:photograph showing the screw–wire system held with a wire twister then used to deliver traction to the |
 |
| Figure 4: photograph showing fixation of the condylar fracture using titanium mini plates and screws aided by the screw and wire system |
 |
| Figure 5: Photographs showing postoperative facial nerve testing immediately after surgery |
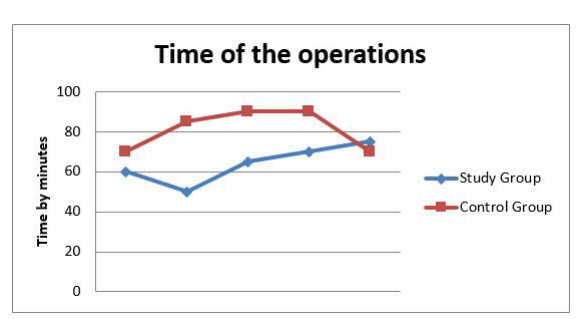 |
| Chart 1: The operation time starting from incision to internal fixation of the condylar fractures |
 |
| Figure 7: Photographs showing postoperative facial nerve testing two months after surgery |
Introduction
Mandibular condylar fractures remain to be one of the most controversial issues in maxillofacial trauma with regards to classification, diagnosis, and treatment despite the high incidence of these fractures. The debate continues over how to best manage subcondylar fractures and the question of which fractures should be treated surgically has yet to be answered Most condylar fractures are a result of blunt trauma to the anterior mandible. Forces are transmitted to the condylar region, where the posterior movement of the mandible is limited by the glenoid fossa, the TMJ capsule, and the insertion of the lateral pterygoid muscles. When the force is sufficient to overcome the strength of the condylar region, fracture follows trauma involving the open mouth leads to flexion fractures of the condyle. Trauma involving the open mouth leads to flexion fractures of the condyle [1, 2].
The symmetrical impact is said to cause bilateral fractures. The unilateral impact causes contralateral condylar fractures, and shearing forces are thought to produce intracapsular fracturesClosed-mouth fractures tend to distribute some of the energy to the occlusal surface of the teeth, and capsule fractures are common. Under the influence of the masticatory muscles, the mandibular ramus may shorten vertically and produce premature occlusal contacts distally. Various surgical approaches have been described for open reduction internal fixation (ORIF) of condylar fractures with different combinations of approaches that have been used. Each has its advantages, disadvantages, and complications. Most surgeons prefer extraoral over intraoral approaches because they provide better visualization of the surgical field. However, there is a risk of surgical complications associated with extraoral approaches, including salivary fistulae, visible scars, and facial nerve damage or palsy. Condylar fracture treatment aims to achieve pain-free mouth opening with good interincisal distance, good movement of the jaw in all excursions, good facial and jaw symmetry, restoration of the pre-injury occlusion, and stable TMJs. Many methods of osteosynthesis of condylar fractures have been described, including fixation of fragments with Kirschner wires, intraosseous wiring, miniplate osteosynthesis, and lag-screw osteosynthesis. Rigid fixation with mini plates is the preferred technique today. Miniplateosteosynthesis provides rigid fixation that may be easily adapted to the curvature of the bone, and requires only a simple operation. So, this study was conducted to evaluate the use of wire and screw technique to aid reduction during open treatment of the condylar and subcondylar fractures [3-8].
Patient and Method
The clinical case material of this study consisted of 10 patients who attended the Department of Oral And Maxillofacial surgery, Alsayed Jalal University Hospital – Cairo- Egypt.
The patients were divided into two groups. (Five for each group). First group, the reduction was assisted through the use of (6 mm length - 2 mm diameter) screw, 26-gauge stainless steel wire, and 16-gauge needle. In the second group, the reduction was performed using a towel clamp and bone hook without stripping the lateral pterygoid muscle from its condylar insertion.
Surgical ProcedureTransmassetric anteroparotid approach was performed in all cases. A preauricular incision was made and extended downwards in a curvilinear fashion in the cervical mastoid skin crease. The great auricular nerve was preserved and the flap was raised in the subdermal fat plane, superficial to the superficial musculoaponeurotic layer to allow access to the masseter adjacent to the anterior edge of the parotid gland [9].
The masseter is split in the direction of its fibers, which in the superficial plane run parallel to the anterior edge of the parotid. It is not necessary to sever the fibers to gain adequate access, but this may be necessary as the fibers change direction in the deeper parts of the muscle. The periosteum overlying the lateral aspect of the ramus in the region of the condylar neck is incised and the fracture site is exposed. MMF was performed. Followed by fixation of the fractured segments titanium 2.0 mm miniplate used to fix each fractured condylar segment in this group and applied on the lateral surface of the condylar neck using 2.0 mm bicortical screws for each. The length of plates and the number of screws were controlled by the position and inclination of the fracture line. Release of MMF and check occlusion several times to confirm correct anatomical and functional reduction and fixation. Wound closure was performed in layers using 3-0 vicryl for deep layers and 4-0 prolene for skin in an interrupted fashion. Application of sterile piece of gauze protecting the wound and a suction drain left in place for 48hrs to minimize edema.
Post-Operative EvaluationClinical evaluation of complications had done for both groups. The pain was evaluated postoperatively by asking the patients about the pain severity after surgery, all patients experienced slight to mild pain at the surgical site. Five had slight pain and showed mild edema which subsided totally by the 4th post-operative day. Four patients had mild pain and mild edema which also disappeared completely by the 4th post-operative day. Only one patient had severe pain and edema after surgery because he had other facial fractures and he was reserved into the intensive care unit for 5 days. Branches of the facial nerve were tested by asking the patients to crease up their forehead (raise their eyebrows), close their eyes and keep them closed against resistance, puff out their cheeks and reveal.
Results
The time of operations was calculated for each patient chart (1). This study included ten male patients. The patient's age ranged from 19-37 years with a mean of 28 years. Nine of the included patients had unilateral subcondylar fractures. Only one patient had a bilateral subcondylar fracture. The fractured condyles occurred on the right side in 7 cases, 2 left side fractures, and one patient had bilateral subcondylar fracture. Eight of the fractured condyles were medially displaced and two laterally displaced. Seven patients had other facial or mandibular fractures that were first repaired using ORIF before the condylar fractures were addressed. The mechanism of injury was motor vehicle accidents in 8 patients and 2 car accidents. The maximum operating time with the transmassetricanteroparotid approach was 90 minutes with a mean of 64 minutes for the study group and 79 minutes for the control group .Table 1.
No facial nerve injury was observed in all patients. All patients experienced a limited mouth opening and lateral extrusion in the early postoperative phase (1-2 weeks) that improved by mouth exercises. Paraesthesia of the great auricular nerve, or Frey's syndrome were not encountered in any case. None of the patients had deviation, pain on chewing, pain during maximal mouth opening, or lateral protrusion, post-operatively. Maximum individual-centric occlusion (MIO) ranged between 33-53 mm without deviation and with stable individual-centric occlusion, all had returned to a normal diet. Computed Tomography (CT) was taken to confirm the position of the reduced condylar fractures. Nine of the included patients enjoyed an acceptable MIO except for only one patient who had a relatively limited MIO of 33 mm at 3 months. Table 2.
At 3 months postoperatively, the lateral extrusion ranged between 8-11 mm to the right and 8-10 mm to the left and the protrusive movement ranged between 4-9 mm. None of the patients showed any signs of TMD postoperatively in terms of pain or TMJ sounds.
Discussion
No area of facial trauma elicits as much debate as to the treatment of fractures of the condylar region. Optimal treatment seems to vary as much by surgical subspecialty as by treating surgeons themselves. Some of this variability is derived from surgeon comfort with different surgical techniques and approaches as well as concern for vital surrounding structure. The surgical repositioning of the mandibular condyle in fractures with dislocation of the small fragment is a rather controversial subject among maxillofacial surgeons [10].
The problems of repositioning are the following: (1) The difficulty of working on the neck of the condyle without damaging the facial nerve; (2) Scanty bone contact in the area of the fracture; and (3) The dislocating force of the external pterygoid muscle. The condyle of the mandible constitutes the mandibular area most involved in fractures as mentioned this is because the condylar neck constitutes the weakest area of the whole mandible [11, 12].
The debate between the supporters of open or closed reduction is still continuing and the issue has not been resolved. At present, except for the highly located intraarticular fractures, open surgery appears to be the mainstream approach for treating mandibular fractures at the condylar neck or subcondylar level. However, the final choice of treatment modality for each individual patient should take into account several factors, including the position of the condyle, location of the fracture, age of the patient, presence or absence of other associated injuries, presence of other systemic medical conditions, history of previous joint disease, the cosmetic impact of the surgery, and desires of the patient [13-14].
Open reduction means principally, the exact anatomical reduction under direct vision, and at the same time retention and internal fixation of the fracture utilizing functionally stable osteosynthesis.
Spezia and patrone [15] summarized the indications for The treatment of subcondylar fraction by open reduction as absolute and relative:
Absolute Indications:- Displacement into the middle cranial fossa.
- Impossibility of obtaining adequate occlusion by closed reduction
- Lateral extracapsular displacement of the condyle.
- Invasion of a foreign body (e.g.: gunshot wound).
- Bilateral condylar fracture in edentulous patients when splinting is impossible.
- Unilateral or bilateral condylar fractures when splinting is not recommended for medical reasons or adequate post-operative physiotherapy is impossible.
- Bilateral condylar fractures associated with comminuted midfacial fractures.
- Bilateral condylar fractures associated with significant pre-injury malocclusion.
According to Spinzia and Patrone(15) these fractures are most often treated with internal rigid fixation because of some unquestionable advantages of this technique, including high osseous stability, avoidance of intermaxillary fixation, rapid functional recovery, and good short-term results. In recent years, the application of plates over the condylar neck has been the subject of much critical review, which has pointed out that rigid internal fixation, presents many problems, such as difficult surgical access, with possible facial nerve injuries and or its ramifications and facial skin scars; a small surgical area; and the possibility of secondary plate removal.
A few concerns remain to be clarified regarding surgical treatment. The first is which and how many fixation devices should be used; however, this was beyond the scope of the present report. A second concern involves the choice of the approach method for treating condylar fractures. The ideal surgical approach should be the least invasive method available, allow a comfortable and easy solution to the surgical problem, be versatile, allow satisfactory vision, have the lowest rate of surgical complications, and be rapidly performed [16,17].
Conventional approaches to the mandibular condyle can be divided into 2 categories, intraoral and extraoral. The intraoral approach was first performed by Kang [18] in 2012 and was subsequently used by Beza [19] in 2016. It is less invasive than extraoral approaches and is free of some of the complications associated with extraoral approaches, such as facial nerve injury and unsightly scars. However, the intraoral route can be technically complex, especially for fractures at higher levels or with medial luxation of the proximal stump. Even with the aid of an endoscope, the procedure requires specific instruments, practitioners with specific training, and a longer operative time. Moreover, some investigators have reported a greater degree of complications with the intraoral approach compared with extraoral approaches. These complications include fragment malposition, condylar head resorption, persistent postoperative malocclusion, and temporomandibular joint functional problems. Many extraoral approaches have been described, with the preauricular, submandibular, and retromandibular approaches most frequently used [20, 21].
Conclusion
According to this study, we concluded that:
Using wire and screw technique for reduction of subcondylar fractures during the open treatment gives many benefits:
1-Allow the surgeon to locate and move the fractured segment of the mandible as a bony anchorage through the reduction screw.
2-Minimal or no postoperative complications related to that technique of reduction compared to using hard surgical instruments to aid reduction and reduce the operative time.
The transmassetericanteroparotid approach provides good accessibility to do open reduction, the final cosmetic outcome is satisfactory, reduces the risk of facial nerve injury, and other salivary complications as fistula and Frey's syndrome as it eliminates the dissection through the parotid gland.
References
- Pickrell BB, Serebrakian AT, Maricevich RS (2017) Mandible Fractures. SeminPlast Surg 31: 100-7.
- Ortiz-Gutiérrez AL, Belinda Beltrán-Salinas B, Cienfuegos R (2019) Mandibular condyle fractures: A diagnosis with controversial treatment. Cirugía y Cirujanos 87: 587-94.
- Kanno T, Sukegawa S, Furuki Y (2009) Our treatment strategy for mandibular condylar fracture-retromandibular approach vs intraoral approach. Jpn J Oral Maxfac Surg 55: 58.
- Singh V, Bhagol A, Goel M, Kumar I, Verma A (2010) Outcomes of open versus closed treatment of mandibular subcondylar fractures: a prospective randomized study. J Oral Maxillofac Surg 68: 1304-9.
- Neff A (2019) Open reduction and internal fixation in temporomandibular joint traumatology: current concepts and future perspectives.Stomatological Dis Sci 3: 2-14.
- Özkan H, Sahin B, Görgü M, Melikoglu C (2010) Results of transmassetericanteroparotid approach for mandibular condylar fractures. J Craniofac Surg 21: 1882-3.
- Schneider M ,Eckelt U (2006) Open versus closed treatment of fractures of the mandibular condylar process–a prospective randomized multi-centre study. J Cranio-Maxillofac Surg 34: 306-14.
- Valiati R, Ibrahim D, Abreu M, Heitz C, de Oliveira R, et al. (2008) The treatment of condylar fractures: to open or not to open? A critical review of this controversy.Int J Med Sci 5: 313-8.
- Rajasekhar G, Sathya K, Kishore K, Sridhar R, Chaithanyaa N, Mallikarjuna D (2016) Preauriculartransmassetericanteroparotid approach for extracorporeal fixation of mandibular condyle fractures .Indian J Plast Surg 49: 59-65.
- Klatt J, Pohlenz P, Blessmann M, Blake F, Eichhorn W, et al. (2010) Clinical follow-up examination of surgically treated fractures of the condylar process using the transparotid approach. J Oral Maxillofac Surg. 68: 611-715.
- Sagiura T, Yamamoto K, Murakami K (2001) Comparative evaluation of osteosynthesis with lag-screws, miniplates, or Kirschner wires for mandibular condylar process fractures. J Oral Maxillofac Surg 59: 1161-8.
- Goyal MA (2012) Comparative Evaluation of Fixation Techniques in Anterior Mandibular Fractures Using 2.0 mm Monocortical Titanium Miniplates Versus 2.4 mm Cortical Titanium Lag Screws.J Maxillofac Oral Surg 11: 442-50.
- Jensen TH , Jensen J, Nørholt SE, Martin Dahl, Lone Hansen L, et al. (2006) Open reduction and rigid internal fixation of mandibular condylar fractures by an intraoral approach: a longterm follow-up study of 15 patients. J Oral Maxillofac Surg 64: 1771-9.
- Choi B, Yi C, Yoo J (2001) Clinical evaluation of 3 types of plate osteosynthesis for fixation of condylar neck fractures. J Oral Maxillofac Surg 59: 734-7.
- Spinzia A, Patrone R, Belli E, Ungari C, et al. (2014) Open reduction and internal fixation of extracapsular mandibular condyle fractures: a long-term clinical and radiological followup of 25 patients. BMC Surgery 14: 2-10.
- Meyer C, Zink S, Chatelain B, WilkA (2008) Clinical experience with osteosynthesis of subcondylar fractures of the mandible using TCP plates. J. Cranio-Maxillofac. Surg 36: 260-8.
- Trost O, Abu El-Naaj I, Trouilloud P, Danino A, Malka G (2008) High cervical transmassetericanteroparotid approach for open reduction and internal fixation of condylar fracture. J Oral Maxillofac Surg 66: 201-4.
- Kang DH (2012) Surgical Management of a Mandible Subcondylar Fracture. Arch Plast Surg 39: 284-90.
- Beza SA, Attia S, Ellis E, Omara LA (2016) Comparative Study of Transbuccal and Extraoral Approaches in the Management of Mandibular Angle Fractures: A Systematic Review.Maced J Med Sci 4: 482-8.
- Rozeboom A, Dubois L, Bos R, Spijker R, de Lange J (2018) Open treatment of condylar fractures via extraoral approaches: a review of complications. J Craniomaxillofac Surg 46: 1232-40.
- Mohamed FI (2020) Three Dimensional Accuracy of Mandibular Reconstruction by Pre-Bent Reconstruction on Plate Using Intra Oral Versus Extra Oral Approaches Following Mandibular Resection in Patients With Extensive Ameloblastoma.EDJ 66: 905-17.
Artcle Information
Review Article
Received Date: June 20, 2022
Accepted Date: July 13, 2022
Published Date: Sept 09, 2022
Journal of Dental Research and Oral Health
Volume 3 | Issue 1
Citation
Ahmed AH El-Feky (2022) Is Using Wire and Screw Technique Aid Reduction During Open Treatment of Condylar and Subcondylar Fractures. J Dent Res Oral Health 1: 1-15
Copyright
©2022 Ahmed AH El-Fek. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jdro.2022.3.102