

Review Article
Volume-1 Issue-1, 2021
Vitamin D and SARS-CoV-2 Infection in IBS Patients The Role of Vitamin D and the Impact of SARS-CoV-2 Infection in Irritable Bowel Syndrome Patients
Received Date: January 26, 2022
Accepted Date: February 26, 2022
Published Date: February 28, 2022
Journal Information
Abstract
Background: Irritable Bowel Syndrome (IBS) is one of the common intestinal diseases reducing quality of life. Its global prevalence varies between 7-21%. Changes in intestinal microbiome, permeability, immune function, motility and visceral sensitivity, brain-intestinal interactions and psychosocial status are suggested to be effective in the pathogenesis of IBS. Variability of symptoms in IBS including chronic abdominal pain with diarrhea or constipation separately or both resulted in different strategies to be carried out in the treatment of the disease.
Summary: In the treatment of IBS patients, a holistic approach consisting of diet, lifestyle changes and drugs is required. Recent studies shown that vitamin D deficiency is common in IBS patients and supplementation of vitamin D can be effective in the treatment of IBS. The immunomodulatory, anti-inflammatory and antimicrobial properties of vitamin D and its association with psychosocial status are related to its role in IBS. Since IBS is a stress-sensitive disorder, impact of SARS-CoV-2 infection on IBS symptoms can not be ignored. In addition, IBS patients have a high risk of vitamin D deficiency resulting more severe symptoms during the pandemic. In this study, the role of vitamin D in IBS and the impact of SARS-CoV-2 infection in IBS patients were reviewed.
Key points: The intervention studies on vitamin D supplementation do not provide strong and generalizable evidence. SARS-CoV-2 infection could effect IBS symptoms. Vitamin D supplementation may be effective for IBS patients during COVID-19 pandemic since IBS patients are prone to infection and have a risk of more severe symptoms.
Key words
İrritable Bowel Syndrome; Vitamin D; Vitamin D Deficiency; Microbiota; SARS-Cov-2 İnfection
 |
| Figure 1: (Top) A display of material used during surgical endoscopy: an endoscope with a high-definition Full HD camera, a flexible fiber optic cable with a cold light source, -(middle) Use of the endoscope during surgery. -(bottom) Viewing the video in real time on a screen in the operating theatre during surgical endoscopy. |
 |
| Figure 2:A world of fibers. Fibers are everywhere, in every nook and cranny and by their intersecting create microvolumes |
 |
| Figure 3:The vessels of the peritendinous sliding network display different non-linear progression during movement within a homogeneous substance |
Introduction
Irritable bowel syndrome (IBS) is one of the most common functional bowel disorders which affects 7 to 21% of general population worldwide [1]. It is characterized by chronic and intermittent abdominal pain or discomfort with altered bowel habits [2]. Depending on to predominant bowel habit, IBS is divided into four categories which are diarrhea-predominant (IBS-D), constipation- predominant (IBS-C), a mixed symptomology (IBS-M) and unclassified IBS (IBS-U) [3]. IBS has a significant cost to society due to its high prevalence, since it impairs daily activities and reduces quality of life [4]. Pathophysiology of IBS is unclear and multifactorial but altered gastrointestinal motility, visceral sensation, brain-gut interactions, and psychosocial distress have become prominent among the host and environmental factors [2]. Drugs for IBS such as antispasmodic drugs, antidepressants, antibiotics, antidiarrhea, anticholinergic drugs, alosetron, lubiprostone, behavioral therapies, exercise and diet interventions are included in the treatment [3].
Vitamin D is a fat-soluble steroid hormone which participates in many cellular mechanisms particularly in calcium-phosphorus metabolism and bone mineralization. Its deficiency is associated with inflammatory bowel disorders, colorectal cancer, depression, sclerosis, and some other pathologies [5]. Being a crucial hormone for the organism, vitamin D aids the calcium and phosphate absorption and also controls the parathyroid hormone secretion. Low vitamin D levels are common in IBS patients and are negatively correlated with symptom severity, similarly as in gastrointestinal diseases like IBD and colorectal cancer [6]. The immunomodulator, anti-inflammatory and antimicrobial properties of vitamin D are associated with its role in IBS [7]. Vitamin D has an important role in many factors associated with the onset and recurrence of IBS such as anxiety and depression, imbalance in intestinal permeability, inflammation and response to microorganisms in epithelial cells. Therefore, vitamin D supplementation may be effective in the control and remission of the disease [8].
SARS-CoV-2 infection has become a global health issue emerging from Wuhan, China in late December 2019, affecting morbidity, mortality, economic loses, and social issues indirectly as a result of social isolation [9]. In addition to people’s fear of infection, preventions, restrictions and prohibitions to control the disease globally caused stress in life. Since IBS is a stresssensitive disorder, symptoms of patients can be influenced by the pandemic situation [10]. Patients with gastrointestinal disorders have an increased risk of SARS-CoV-2 infection owing to existence of gut dysbiosis [11]. Vitamin D supplementation is suggested especially to people with high vitamin D deficiency risk during COVID-19 pandemic [12].
IBS Pathophysiology
IBS has a multifactorial, complex and unclear pathophysiology including changes in gut microbiome, genetic factors, immune response, physiologic stress, and psychosocial factors with some possible mechanisms [8,13].
Gut motility
Gut-brain axis dysregulation causes dysmotility throughout intestines. Motility response increases against stressors in IBS patients [14]. Increased gas retention in intestines and delayed transit of the gas from duodenum to rectum were reported in IBS patients [15].
Food Intolerance
Fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) triggers IBS symptoms. A metaanalysis demonstrated that a low FODMAP diet may improve IBS symptoms especially abdominal pain, bloating, and diarrhea [16].
Inflammation
IBS symptoms can be seen in patients with inflammatory diseases like celiac, inflammatory bowel disease or gastroenteritis. Although, there is an unclear pathophysiology of inflammation on IBS symptoms, there is an possible explanation that the inflammatory response alters intestinal permeability resulting in IBS symptoms [17].
Intestinal hypersensitivity
Intestinal hypersensitivity is a clinical marker of IBS which has an unclear reason. After an inflammation it can be seen with intestinal permeability [18]. Because of longer intestine emptying times; bowel distention and bloating are encountered as symptoms of intestinal permeability in IBS patients [15].
Post-infection
After an enteric infection, IBS symptoms are observed in 20% of patients. Prolonged fever, prolonged infection, anxiety, depression, and younger age are possible risk factors causing IBS symptoms [17].
Stress and depression
Stress, anxiety and depression are main psychological comorbities worsening IBS symptoms. Brain-gut axis dysfunction is a possible explanation of IBS pathophysiology. While central nervous system can change gut physiology, alterations in the gut can also effect psychology through interacting with brain [13].
Microbiome
IBS patients have altered microbiota and lower number and variety of bacterias in their gut [17]. Altered microbiota takes place IBS pathogenesis through increased permeability, changes in immune response, gut–brain axis and gut function [14].
Genetics
A wide range of genes and their interactions were explained as genetic impact of IBS. Some familial similarities related to having a monozygotic twin and mother with IBS were shown in several studies. Additionaly, many patients with IBS report that they have relatives experiencing IBS [13].
IBS Management
IBS management consists of individualized and multidisciplinary approach including pharmacological treatment, psychological therapy and dietary intervention. Antispasmodics, antidepressants, eluxadoline, lubiprostone, and linaclotide are suggested pharmacological therapies for IBS management. Low fermentable oligosaccharides, disaccharides, monosaccharides, polyols (FODMAP) diet, peppermint oil, probiotics, psyllium (not wheat bran), cognitive behavioral therapy and hypnotherapy are recommended as non- pharmacological treatment options [19]. Since it is a symptom-based syndrome, it is important to define gastrointestinal symptoms and the IBS subtype before selecting the treatment method [1]. Regular physical activity is recommended to IBS patients in order to get rapid bowel habits and improve the symptoms of illness. Some studies conducted with IBS patients support that exercise decreases colonic transit time and gastrointestinal symptoms [3]. Ninety percent of IBS patients associate their symptoms with their diet and make dietary restrictions [1]. Dietary interventions in IBS mainly consist of low FODMAP diet, gluten free diet. However, most of the dietary interventions have low level of recommendation and strength of evidence. Low FODMAP diet takes the largest part of literature in terms of dietary interventions. Besides, fiber consumption has a strong evidence, especially poorly fermentable and soluble fiber is recommended for IBS treatment [3].
Vitamin D Mechanism on IBS Pathophysiology
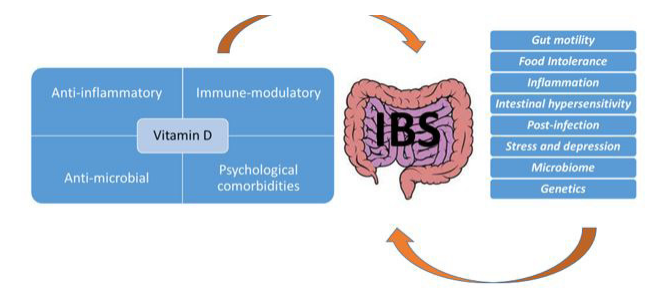
Although the exact pathophysiology of IBS has not been identified; changes in the gut microbiome, intestinal permeability, gut immune function, visceral sensation, brain–gut interactions, and psychosocial status are demonstrated as possible mechanisms [2]. Vitamin D has role in these mechanisms in terms of intestinal barrier function, immune response, T-cell regulation and central sensitivity [20] (Figure 1). Vitamin D synthesis begins with activation of 7-dehydrocholesterol in the skin. It is hydroxylated in the liver to produce 25-hydroxycholecalciferol and converted to 1,25 (OH)2D3 in the kidney to produce its active form. Vitamin D receptor intercedes biological activity of 1,25(OH)2D3. Vitamin D and vitamin D receptor regulates gut microbiome altering gut microbiome composition, regulating immune response, microbiota dysbiosis and gut tolerance [21].
Vitamin D and Microbiota
Vitamin D has a potential effect on microbiota. Its deficiency causes dysbiosis that induces inflammation. Vitamin D may alter gut microbiota through affecting intestinal immune cells. On the other hand, if vitamin D levels are low, specific bacterias compete with other microorganisms and lower the immune response [8]. In addition, alterations in vitamin D receptor gene affect human gut microbiome. Vitamin D and vitamin D receptor signaling is significant in intestinal barrier function, immunity and homeostasis [22].
Vitamin D and Immune response
Effect of vitamin D on immune system is demonstrated for Inflammatory Bowel Diseases (IBD). As immune system has also an important role in IBS pathophysiology, vitamin D may have similar effects on IBS [8]. Vitamin D receptors and enzymes regulate immune system through antigen-presenting-cells, T cells, B cells and monocytes [23].
Vitamin D and Psychological Comorbidities
According to American Association of Gastroenterology, depression and anxiety is prevalent (%60) in IBS patients and exacerbates gastrointestinal symptoms [24]. The relationship between vitamin D deficiency and depression has been investigated in many studies. Therefore; vitamin D supplementation can improve symptoms and quality of life by improving anxiety, stress and depression in IBS patients [25]. Dysregulated serotonin production and vitamin D insufficiency may have a role in IBS pathophysiology and pathogenesis.
Vitamin D modulates the expression of genetic biomarkers of IBS [26].
Vitamin D Status
Low level of sunlight exposure, diet with low vitamin D, dark skin color, aging and obesity take part as risk factors of vitamin D deficiency [27]. It is estimated that vitamin D deficiency is very common, occuring in 1 billion people worldwide [28]. Prevalence rates of 25(OH)D levels < 50nmol/L (or 20ng/ml) have been stated as 24% in US, 37% in Canada, and 40% in Europe. These levels have been estimated lower in children and elderly [29]. According to Endocrine Society, less than 20 ng/mL (50 nmol/L) of 25(OH)D level is defined as deficiency, levels between 20 to 29.9 ng/mL (52–72 nmol/L) is defined as insufficiency whereas levels higher than 30 ng/mL (75 nmol/L) is defined as sufficiency [30]. Moreover, Institute of Medicine (IOM) recommends 20 ng/ mL (50 nmol/L) of vitamin D for a healthy individual in order to maintain bone health [31]. Vitamin D intoxication occurs when the levels reach 150 ng/mL [28].
Vitamin D Deficiency in IBS
Vitamin D deficiency is defined as 25(OH)D level of less than 20 ng/ml [28]. Vitamin D status of IBS patients were investigated in several observational studies. Vitamin D deficiency was found significantly more common (82%) in patients with IBS compared to healthy individuals [32]. In a study, 1000 IBS patients were examined and serum 25(OH)D concentrations were lower than 30 nmol in 72% of women and 3% of men [6]. According to study conducted with 90 IBS patients and control group; 66.7 % of patients’ serum 25(OH)D levels were lower than 20 ng/ml. In addition to the high prevalence of vitamin D deficiency in IBS patients, vitamin D deficiency is associated with more severe clinical symptoms and lower quality of life. There is a significant association between vitamin D levels and quality of life [33]. In a retrospective study; vitamin D deficiency has been reported among more than 50% of pediatric IBS patients ages between 6-21 years. The study suggests that it is important to perform routine screening of vitamin D levels in these patients. This study also states that female gender and migraine are posssible factors associated with lower vitamin D levels [34]. In a cross-sectional study with 965 adolescent girls, IBS was found to be associated with reduced vitamin D levels. Patients with higher physical activity levels had higher vitamin D levels. Furthermore, being overweight and obese and lower AST and ALT concentrations were reversely related with vitamin D status [35].
Dietary sources, supplements and ultraviolet B exposure are known as main sources of vitamin D [28]. Natural sources of vitamin D are limited in foods that is why in some countries foods are fortified with vitamin D. It is found in foods in two forms: cholecalciferol (D3) from animal sources and ergocalciferol (D2) from plant sources. Fish, egg yolk and liver are good sources of vitamin D3, whereas some mushrooms are good sources of vitamin D2. Fortification can be made with D2 and D3 forms. Milk, breakfast cereals, margarine and fortified orange juice are some fortified foods in US [36].
There is no international recommendation for optimum vitamin D supplementation. The Endocrine Society recommends 10,000 IU as daily safe level, while the IOM and The European Food and Safety Authority recommend to stay below 4000 IU/ day (100µg) [29].
Vitamin D in Treatment of IBS
There are intervention studies investigating effects of vitamin D supplementation on IBS. In a 6-month study conducted with adolescents with IBS and vitamin D deficiency, vitamin D supplementation compared to the placebo group resulted in significant improvement in IBS symptoms and quality of life and it created a significant increase (2-fold) in serum vitamin D levels [7]. In a double-blind, randomized and placebocontrolled study; IBS patients were given 50,000 IU of vitamin D3 or a placebo. There was a significant improvement in IBS symptoms. Vitamin D supplements improve the quality of life (QoL) in IBS patients by improving anxiety and depression [37]. According to the factorial blinded study of effects of vitamin D and soy isoflavones on IBS treatment with women participants, co-administration of vitamin D and soy isoflavones significantly effected on total score of IBS. However, it did not improved symptom scores and quality of life. Vitamin D and soy isoflavones alone significantly improved symptom scores and quality of life [38]. Another study of vitamin D and soy isoflavones coadministration showed that vitamin D and soy isoflavones supplementation reduced plasma inflammatory markers and fecal protease activity which can be related to inflammation and intestinal permeability of IBS [39]. Jalili et al. also carried a double-blind, randomized and placebo-controlled study in order to indicate effect of vitamin D on women participants with IBS who do not get medicine for their symptoms and have similar diets. 6 weeks of vitamin D supplementation improved patients’ IBS symptoms and QoL [20]. A case study examined a woman with IBS who was diagnosed 20 years ago and high dose of vitamin D (50-75 μg per day) positively affected IBS symptoms, bowel functions, anxiety and depression. Also, social media accounts of IBS patients analysed in same paper and vitamin D supplementation improved symptoms in %70 of patients [40]. Another randomized clinical trial, conducted in patients with diarrhea-predominant IBS (IBS-D), analyzed the effects of vitamin D supplementation on pathogenesis. Participants were taken 50,000 IU/week of vitamin D3 or placebo. Vitamin D3 supplementation improved symptom severity, quality of life, depression and visceral sensitivity in IBS patients after 9 weeks of treatment. Serum serotonin concentrations and anxiety levels were not found significantly different [24]. Based on the knowledge of immune-modulatory and anti-inflammatory role of vitamin D, effect of vitamin D on inflammatory cytokines and biomarkers of oxidative stress were investigated in a trial. The double-blinded, placebo-controlled randomized study was conducted with 90 IBS patients for 6 months. Vitamin D supplementation showed a positive impact on some of these markers especially on IBS-D [41]. In a 12-week, randomized and double blinded study; it has been found that low vitamin D levels are associated with low quality of life in IBS [42]. The study indicates that vitamin D supplementation, compared to placebo and both vitamin D and probiotics, may have a positive effect on IBS patients with vitamin D deficiency through enhancing life quality of patients. Although this study of IBS did not find it effective, according to the results of a systematic review; cosupplementation of vitamin D and probiotics is effective in management of many chronic diseases [43].
Impacts of SARS-CoV-2 Infection in IBS Patient
COVID-19 pandemic may affect gastrointestinal and psychological symptoms of IBS which is a gut-brain disorder responsive to stress [44]. Anxiety, stress and depression have become more prevalent worldwide since the beginning of COVID-19 pandemic. Spending longer time in quarantine was associated with increased psychological problems while family support was associated with decreased anxiety, stress and depression [45]. A study aiming to examine the effects of COVID-19 pandemic on IBS patients asserted that participants with IBS had worsened well-being and less adherence to social distancing compared to non-IBS participants. Most of the IBS patients reported that their symptoms have not changed during pandemic, about 27% of patients reported improved symptoms and about 12% of patients reported worsened symptoms. A higher proportion of the participants not experiencing symptom changes were disposed to maintain social distancing for an indefinite time period compared to those with worsened symptoms. Furthermore, participants with no symptom changes had better emotional well-being. Those participants had more fear of infection and applied better hygiene practices compared to participants with symptom deterioration [10]. COVID-19 pandemic may cause stress which exaggerates IBS symptoms in patients. An observational study analysed the impact of the COVID-19 related stress on patients with IBS in Saudi Arabia. The patients reported fear of self-infection or a family member infection and fear of death. Most of the stressed patients reported that they usually experience more severe symptoms. Some of them consulted a physician and used medication [46]. Another study examined the effect of COVID-19 caused stress on gastrointestinal symptoms of IBS, anxiety and depression. Most of the subjects reported increased stress, anxiety and depression in addition to increased gastrointestinal symptoms such as diarrhea, constipation and abdominal pain in about half of the subjects [47]. An online survey study conducted in Japan investigated SARS-CoV-2 infection on IBS and functional dyspepsia (FD) patients. The study demonstrated that COVID-19 pandemic caused negative impact on IBS/FD. Major percentage of subjects (85.3%) did not report changes in symptoms followed by worsened symptoms (11.9%) and improved symptoms (2.8%).
Subjects with both IBS and FD got the worst symptom scores [44]. Psychological disease comorbidity and occupational issues were suggested as factors worsening or improving IBS symptom severity. Youth, commuting public transportation before quarantine, working from home and flexible work or school hours were found as improving factors while occupational stress was an worsening factor [44].
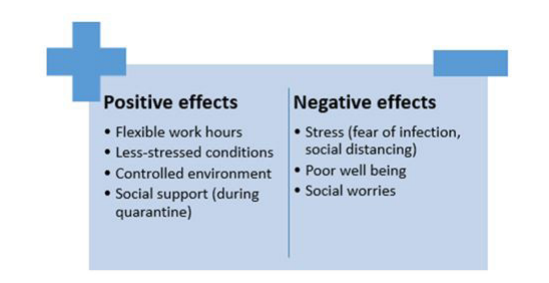
Although COVID-19 pandemic has some properties such as causing stress and poor well-being which may negatively effect IBS symptom severity, no change or improvement in symptoms were observed in a high percentage of patients. This condition was defined as COVID-19 IBS paradox by some researchers [10]. Low quality of life in IBS patients tends to higher risk of depression. Alterations in bowel habits, worries about body image, food choices and other social worries impair daily and social activities [48]. Flexible work hours, better social wellbeing due to social support of close ones, less stressed conditions related to work and a controlled environment preventing impairments in activities have been explained as possible causes of improvement in symptoms [10] (Figure 2).
COVID-19 Risk and Impact of Vitamin D in IBS Patients
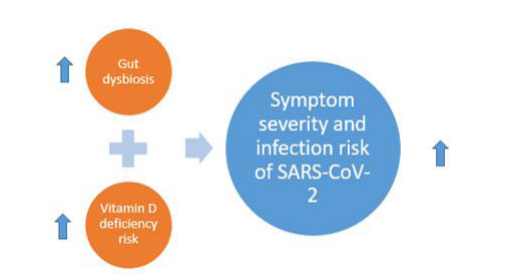
Studies show that vitamin D supplementation may protect against respiratory tract infections through its anti-inflammatory and immunomodulatory role and inhibition of viral replication (Ali, 2020). T regulatory lymphocytes provide a defence mechanism against inflammation and viral infection and vitamin D supplementation can increase its levels. Additionally, an increase in inflammatory cytokines associated with low levels of vitamin D causes an increased risk of viral respiratory tract infections [49]. Vitamin D supplementation is recommended to people who have more risk of vitamin D deficiency during COVID-19 pandemic. However, there is not enough evidence on its effect on COVID-19 severity and mortality [12]. Patients with gastrointestinal diseases like IBS and comorbidites like type 2 diabetes and obesity are prone to gut dysbiosis leading higher severity and infection risk of COVID-19 (Figure 3). Altered fecal microbiota was associated with SARS-CoV-2 infection and COVID-19 severity at fecal level. Therefore, therapeutic approaches to manage gut microbiota are necessary [11]. Since vitamin D deficiency is a common problem for people with IBS, it may be important to get sufficient vitamin D especially during pandemic.
Conclusion
IBS is a common gastrointestinal disease reducing quality of life and has important effects on societies. Symptom variability and multifactorial pathogenesis of IBS needs to follow a multidisciplinary approach in IBS treatment. Vitamin D is a crucial hormone for the organism and the factors related psychosocial comorbidities, immune response and gut microbiome are possible effects of Vitamin D on IBS. Vitamin D deficiency in IBS patients and its association with lower quality of life and severe symptoms were demonstrated in several studies. Furthermore, the intervention studies on vitamin D supplementation do not provide strong and generalizable evidence due to the differences in dose administered, duration of treatment and sample size. Therefore; further long-term studies with larger sample size are needed for the application of vitamin D in the treatment of IBS. SARS-CoV-2 infection could effect IBS symptoms negatively because of social isolation and stress of the pandemic. On the other hand, no change or improvement in symptoms were observed in a high percentage of patients. In addition, IBS patients are prone to infection and have a risk of more severe symptoms because of gut dysbiosis and a high risk of vitamin D deficiency. That is why, vitamin D supplementation may be more effective for IBS patients during COVID-19 pandemic. Also, health effects of pandemic on IBS patients should be investigated in future studies.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
No funding has been received.
Author Contributions
The contributions of the authors are as follow: S.E. Yilmaz, A. Gunes-Bayir, for searching published papers on the current theme; S.E. Yilmaz, A. Gunes-Bayir for designing this study; S.E. Yilmaz for writing this paper. All authors read and approved the manuscript.
References
- Chey WD, Kurlander J, Eswaran S (2015) Irritable Bowel Syndrome: A Clinical Review. JAMA 313 (9): 949–958. doi:10.1001/ jama.2015.0954
- Schoenfeld PS (2016) Advances in IBS 2016: A Review of Current and Emerging Data. Gastroenterol Hepatol (NY) 12 (8 Suppl 3): 1‐11.
- Ford AC, Moayyedi P, Chey WD, Harris LA, Lacy BE et al. (2018) ACG Task Force on Management of Irritable Bowel Syndrome. American College of Gastroenterology Monograph on Management of Irritable Bowel Syndrome. The American Journal of Gastroenterology 113(2): 1–18. doi: 10.1038/s41395-018- 0084-x
- Jerndal P, Ringström G, Agerforz P, Karpefors M, Akkermans LM et al. (2010) Gastrointestinal‐specific anxiety: an important factor for severity of GI symptoms and quality of life in IBS. Neurogastroenterology & Motility 22: 646-e179. doi: 10.1111/j.1365- 2982.2010.01493.x
- DeLuca, HF (2004) Overview of general physiologic features and functions of vitamin D. The American Journal of Clinical Nutrition 80(6): 1689-1696.
- Williams CE, Williams EA, Corfe BM (2018) Vitamin D status in irritable bowel syndrome and the impact of supplementation on symptoms: what do we know and what do we need to know?. European Journal of Clinical Nutrition 72(10): 1358–1363. doi: 10.1038/s41430-017-0064-z
- El Amrousy D, Hassan S, El Ashry H, Yousef M, Hodeib H (2018) Vitamin D supplementation in adolescents with irritable bowel syndrome: Is it useful? A randomized controlled trial. Saudi J Gastroenterol 24(2): 109‐114. doi:10.4103/sjg.SJG_438_17
- Barbalho SM, Goulart RA, Araújo AC, Guiguer EL, Bechara MD (2019) Irritable bowel syndrome: a review of the general aspects and the potential role of vitamin D. Expert Review of Gastroenterology & Hepatology 13(4): 345-359. doi: 10.1080/17474124.2019.1570137
- Romano CM, Chebabo A, Levi JE (2020) Past, present, and future of COVID-19: a review. Brazilian Journal of Medical and Biological Research 53(9): e10475. doi: 10.1590/1414- 431x202010475
- Quek S, Loo E, Demutska A., Chua CE, Kew GS et al. (2021) Impact of the coronavirus disease 2019 pandemic on irritable bowel syndrome. Journal of Gastroenterology and Hepatology. doi: 10.1111/jgh.15466
- Vodnar DC, Mitrea L, Teleky, BE, Szabo, K, Călinoiu, LF, Nemeş, SA, & Martău, GA (2020) Coronavirus Disease (COVID-19) Caused by (SARS-CoV-2) Infections: A Real Challenge for Human Gut Microbiota. Frontiers in Cellular and Infection Microbiology 10: 575559. doi: 10.3389/ fcimb.2020.575559
- Ali N (2020) Role of vitamin D in preventing of COVID-19 infection, progression and severity. Journal of Infection and Public Health 13(10): 1373–1380. doi: 10.1016/j.jiph.2020.06.021
- Black, CJ, Ford AC (2020) Global burden of irritable bowel syndrome: trends, predictions and risk factors. Nature Reviews. Gastroenterology & Hepatology 17(8): 473–486. doi: 10.1038/ s41575-020-0286-8
- Radovanovic-Dinic B, Tesic-Rajkovic S, Grgov S, Petrovic G, Zivkovic V (2018) Irritable bowel syndrome - from etiopathogenesis to therapy. Biomedical Papers of the Medical Faculty of the University Palacky, Olomouc, Czechoslovakia 162(1): 1–9. doi: 10.5507/bp.2017.057
- Defrees DN, Bailey J (2017) Irritable Bowel Syndrome: Epidemiology, Pathophysiology, Diagnosis, and Treatment. Primary Care 44(4): 655–671. doi: 10.1016/j.pop.2017.07.009
- Altobelli E, Del Negro V, Angeletti PM, Latella G (2017) LowFODMAP Diet Improves Irritable Bowel Syndrome Symptoms: A Meta-Analysis. Nutrients 9(9): 940. doi: 10.3390/nu9090940
- Hadjivasilis A, Tsioutis C, Michalinos A, Ntourakis D, Christodoulou DK et al. (2019) New insights into irritable bowel syndrome: from pathophysiology to treatment. Annals of Gastroenterology 32(6): 554–564. doi: 10.2524/aog.2019.0428
- Zhou Q, Verne GN (2011) New insights into visceral hypersensitivity--clinical implications in IBS. Nature reviews. Gastroenterology & Hepatology 8(6): 349–355. doi: 10.1038/ nrgastro.2011.83
- Moayyedi P, Andrews CN, MacQueen G, Korownyk C, Marsiglio M et al. (2019) Canadian Association of Gastroenterology Clinical Practice Guideline for the Management of Irritable Bowel Syndrome (IBS). Journal of the Canadian Association of Gastroenterology 2(1): 6–29. doi: 10.1093/jcag/gwy071
- Jalili M, Vahedi H, Poustchi H, Hekmatdoost A (2019) Effects of Vitamin D Supplementation in Patients with Irritable Bowel Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. International Journal of Preventive Medicine 10: 16. doi: 10.4103/ijpvm.IJPVM_512_17
- Shang M, Sun J (2017) Vitamin D/VDR, Probiotics, and Gastrointestinal Diseases. Current Medicinal Chemistry 24(9): 876–887. doi: 10.2174/0929867323666161202150008
- Sun J (2018) Dietary vitamin D, vitamin D receptor, and microbiome. Current Opinion in Clinical Nutrition and Metabolic Care 21(6), 471–474. doi: 10.1097/MCO.0000000000000516
- Prietl B, Treiber G, Pieber TR, Amrein K (2013) Vitamin D and immune function. Nutrients 5(7), 2502–2521. https://doi. org/10.3390/nu5072502
- Khalighi SM, Mokhtare M, Shidfar F, Janani L, Faghihi KA (2020) Effects of vitamin D3 supplementation on clinical symptoms, quality of life, serum serotonin (5-hydroxytryptamine), 5-hydroxy-indole acetic acid, and ratio of 5-HIAA/5-HT in patients with diarrhea-predominant irritable bowel syndrome: A randomized clinical trial. EXCLI Journal 19, 652–667. doi: /10.17179/excli2020-2247
- Kerr DC, Zava DT, Piper WT, Saturn SR, Frei B (2015) Associations between vitamin D levels and depressive symptoms in healthy young adult women. Psychiatry Research 227(1): 46‐51. doi:10.1016/j.psychres.2015.02.016
- Dussik CM, Hockley M, Grozić A, Kaneko I, Zhang L et al. (2018) Gene Expression Profiling and Assessment of Vitamin D and Serotonin Pathway Variations in Patients With Irritable Bowel Syndrome. Journal of Neurogastroenterology and Motility 24(1), 96–106. doi: 10.5056/jnm17021
- Holick MF, Chen TC (2008) Vitamin D deficiency: a worldwide problem with health consequences. The American Journal of Clinical Nutrition 87(4): 1080S–6S. doi: 10.1093/ ajcn/87.4.1080S
- Holick MF (2007) Vitamin D deficiency. N Engl J Med 357: 266–81.
- Amrein K, Scherkl M, Hoffmann M, NeuwerschSommeregger S, Köstenberger M et al. (2020) Vitamin D deficiency 2.0: an update on the current status worldwide. European Journal of Clinical Nutrition 74(11), 1498–1513. doi: 10.1038/s41430-020-0558-y
- Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA et al. (2011) Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. The Journal of clinical endocrinology and metabolism 96(7): 1911–1930. doi: 10.1210/jc.2011-0385
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium, Ross AC, Taylor CL, Yaktine AL, Del Valle HB (eds) (2011) Dietary Reference Intakes for Calcium and Vitamin D. National Academies Press (US).
- Khayyat Y, Attar, S (2015) Vitamin D Deficiency in Patients with Irritable Bowel Syndrome: Does it Exist?. Oman Medical Journal 30(2): 115–118.
- Abbasnezhad A, Amani R, Hasanvand A, Yousefi RE, Alipour M (2019) Association of Serum Vitamin D Concentration With Clinical Symptoms and Quality of Life in Patients With Irritable Bowel Syndrome. Journal of the American College of Nutrition 38(4), 327–333. doi: 10.1080/07315724.2018.1510349
- Nwosu BU, Maranda L, Candela, N (2017) Vitamin D status in pediatric irritable bowel syndrome. PloS One 12(2): e0172183. https://doi.org/10.1371/journal.pone.0172183
- Khayyatzadeh SS, Vatanparast H, Avan A, Bagherniya M, Bahrami, A et al. (2017) Serum Transaminase Concentrations and the Presence of Irritable Bowel Syndrome Are Associated with Serum 25-Hydroxy Vitamin D Concentrations in Adolescent Girls Who Are Overweight and Obese. Annals of Nutrition & Metabolism 71(3-4): 234–241. doi: 10.1159/000484634
- Lamberg-Allardt C (2006) Vitamin D in foods and as supplements. Progress in Biophysics and Molecular Biology 92(1): 33–38. doi: 10.1016/j.pbiomolbio.2006.02.017
- Abbasnezhad A, Amani R, Hajiani E, Alavinejad P, Cheraghian B et al. (2016) Effect of vitamin D on gastrointestinal symptoms and health-related quality of life in irritable bowel syndrome patients: a randomized double-blind clinical trial. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society 28(10): 1533–1544. doi: 10.1111/nmo.12851
- Jalili M, Hekmatdoost A, Vahedi H, Poustchi H, Khademi B et al. (2016) Co-Administration of Soy Isoflavones and Vitamin D in Management of Irritable Bowel Disease. PloS One. 11(8): e0158545. doi:10.1371/journal.pone.0158545
- Jalili M, Vahedi H, Poustchi H, & Hekmatdoost, A (2019) Soy isoflavones and cholecalciferol reduce inflammation, and gut permeability, without any effect on antioxidant capacity in irritable bowel syndrome: A randomized clinical trial. Clinical Nutrition ESPEN 34: 50–54. doi: 10.1016/j.clnesp.2019.09.003
- Sprake EF, Grant VA, Corfe BM (2012) Vitamin D3 as a novel treatment for irritable bowel syndrome: single case leads to critical analysis of patient-centred data. BMJ Case Reports. doi: 10.1136/bcr-2012-007223
- Amani R, Abbasnezhad A, Hajiani E, Cheraghian B, Abdoli Z et al. (2018) Vitamin D3 Induced Decrease in IL-17 and Malondialdehyde, and Increase in IL-10 and Total Antioxidant Capacity Levels in Patients with Irritable Bowel Syndrome. Iranian Journal of Immunology: IJI 15(3): 186–196. doi: 10.22034/IJI.2018.39388
- Tazzyman S, Richards N, Trueman AR, Evans AL, Grant VA et al. (2015) Vitamin D associates with improved quality of life in participants with irritable bowel syndrome: outcomes from a pilot trial. BMJ Open Gastroenterology 2: e000052.
- Abboud M, Rizk R, Al Anouti F, Papandreou D, Haidar S et al. (2020) The Health Effects of Vitamin D and Probiotic Co-Supplementation: A Systematic Review of Randomized Controlled Trials. Nutrients 13(1): 111. https://doi.org/10.3390/ nu13010111
- Oshima T, Siah K, Yoshimoto T, Miura K, Tomita T et al. (2020) Impacts of the COVID2019 pandemic on functional dyspepsia and irritable bowel syndrome: A population-based survey. Journal of Gastroenterology and Hepatology Advance online publication. doi: 10.1111/jgh.15346
- Shah S, Mohammad D, Qureshi M, Abbas MZ, Aleem S (2021) Prevalence, Psychological Responses and Associated Correlates of Depression, Anxiety and Stress in a Global Population, During the Coronavirus Disease (COVID-19) Pandemic. Community Mental Health Journal 57(1): 101–110. doi: 10.1007/s10597-020-00728-y
- Alzahrani MA, Alshamrani AS, Ahmasani IM, Alahmari FS, Asiri AH (2020) Coronavirus disease 2019 pandemic stress and its effects on irritable bowel syndrome patients in Saudi Arabia. Medicine 99(51): e23711. doi: 10.1097/MD.0000000000023711
- Kamp KJ, Levy RL, Munson, SA, Heitkemper, MM (2021) Impact of COVID-19 on Individuals With Irritable Bowel Syndrome and Comorbid Anxiety and/or Depression. Journal of Clinical Gastroenterology Advance online publication. doi: 10.1097/MCG.0000000000001515
- Kopczyńska M, Mokros Ł, Pietras T, Małecka-Panas E (2018) Quality of life and depression in patients with irritable bowel syndrome. Przeglad Gastroenterologiczny 13(2): 102–108. doi: 10.5114/pg.2018.75819
- Weir EK, Thenappan T, Bhargava M, Chen Y (2020) Does vitamin D deficiency increase the severity of COVID-19?. Clinical Medicine (London, England) 20(4): e107–e108. doi: 10.7861/clinmed.2020-0301
Artcle Information
Review Article
Received Date: January 26, 2022
Accepted Date: February 26, 2022
Published Date: February 28, 2022
Journal of Immunology and Respiratory Medici
Volume 1 | Issue 1
Citation
ISolmaz Ece Yilmaz (2022) Vitamin D and SARS-CoV-2 Infection in IBS Patients The Role of Vitamin D and the Impact of SARS-CoV-2 Infection in Irritable Bowel Syndrome Patients. World J Immunol and Resp Med 1(1):103
Copyright
©2022 Solmaz Ece Yılmaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jirm.2022.1.101