

Review Article
Volume-1 Issue-1, 2021
Assessing The Seroprevalence of Zikavirus Antibodies Among Pregnant Women in Selected Health Care Facilities in Lagos Southwestern Nigeria
Received Date: October 10, 2021
Accepted Date: November 10, 2021
Published Date: November 10, 2021
Journal Information
Abstract
Introduction: Zika virus is an Aedes mosquito or sexually transmitted pathogen resulting in an infection characterized by, fever, rash, conjunctivitis, headaches, muscle and joint pains, which typically start 3-6 days after infection. Currently, the majority of people diagnosed with Zika Virus however remain asymptomatic. Zika Virus infection in pregnant women results in severe birth defects including microcephaly. The prevalence of the infection among pregnant women in Nigeria is not known. Therefore, this study aimed to assess the prevalence of zika virus antibodies and risk factors implicated with infection among pregnant women accessing care at Obstetrics and Gynecology department of General Hospital, Lagos southwest Nigeria.
Methodology: A descriptive cross-sectional study was carried out among 442 consenting pregnant women consecutively enrolled (age ranged 18-48years (SD=- 6.1; Mean=30.9) attending Antenatal clinics at General Hospital Badagry from February 1st to March 28th 2018. Blood sample collected from each consenting participant was screened for Zika virus IgG and IgM using Audacia BioScience Zika virus rapid antigen test Kit. Information on Socio-demographic characteristic, reproductive profile and risk factors for contracting Zika Virus was obtained using questionnaires. Data were analyzed with SPSS Version 20.0 at p< 0.05 using a 95% confidence interval considered significant.
Results: This study found an overall rate of 1.6% for AntiZika virus among asymptomatic pregnant women in Lagos indicating both active and passive infections. Highest rate (2.04%) was found among age group 31-35years followed by 1.61% among age group 36-40years. Various risk factors identified included, relatively high Zika virus rates by Reported fever (OR=9.974; 95%CI=-2.29–34.08; p=0.0118), Anaemia (OR=14.34; 95%CI =3.32–50.14; p=0.0018), Skin rash (OR=9.024; 95%CI =-2.154–33.01; p=0.0079), Joint/Muscle pain (OR=5.406; 95%CI=1.31–19.96; p=0.0466), Conjunctivitis (OR=28.06; 95%CI =-5.046–77.52; p=0.0058) and Oedema (OR=4.971; 95%CI=1.216-18.86; p=0.429). None of the bio-demographic variables as risk factors evaluated significantly influenced Zika virus rate (p>0.05).
Conclusion: This study showed a relatively high rate of Zika virus among the participants and further revealed the possibilities of risk factors associated for the spread of the infection in the community. Conjunctivitis was found to be a major risk factor for zika virus among others. Therefore, compulsory diagnosis for Zika virus for all pregnant women during antenatal visit for early detection of the virus is advocated.
Key words
Zika Virus, Pregnant Women, Risk Factors, Congenital, Nigeria
Socio-demographic characteristics |
Frequency |
Percentage (%) frequency |
Age group (in years) |
|
|
≤25 |
78 |
17.6% |
26 – 30 |
137 |
31.0% |
31 – 35 |
147 |
33.3% |
36 – 40 |
62 |
14.03% |
≥41 |
18 |
4.07% |
Level of education |
|
|
None |
18 |
4.08% |
Primary |
26 |
5.88% |
Secondary |
212 |
47.96% |
Tertiary |
186 |
42.08% |
Reported Fever |
|
|
Yes, ≥38ºC at point of enrolment |
34 |
7.69% |
No |
408 |
92.31% |
Area of Residence |
|
|
Urban |
359 |
81.22% |
Rural |
83 |
18.78% |
Gravidity |
|
|
Primigravidae |
113 |
25.57% |
Secundigravidae |
156 |
35.29% |
Multigravidae |
173 |
39.14% |
Parity |
|
|
Primiparous |
206 |
46.61% |
Multiparous |
236 |
53.39% |
Gestational age |
|
|
1sttrimester (1-14weeks) |
142 |
32.13% |
2ndtrimester (15-27weeks) |
186 |
42.08% |
3rd trimester (≥28weeks) |
114 |
25.79% |
Birds around the environment |
|
|
Yes |
44 |
9.95% |
No |
398 |
90.05% |
Body/Skin rash |
|
|
Yes |
60 |
13.57% |
No |
382 |
86.43% |
Joint/Muscle pain |
|
|
Yes |
56 |
12.67% |
No |
386 |
87.33% |
Conjunctivitis |
8 |
1.81% |
Yes |
434 |
98.19% |
No |
|
|
Use of ITNs |
|
|
Yes |
265 |
59.95% |
No |
177 |
40.05% |
Use of mosquito repellants insecticide |
|
|
Yes |
258 |
58.37% |
No |
184 |
41.63% |
Edema of extremities |
|
|
Yes |
96 |
21.72% |
No |
346 |
78.28% |
Anaemia (Moderate/mild) |
|
|
Yes |
41 |
9.28% |
No |
401 |
90.72% |
Variables |
Number tested |
Number positive (%) |
Number negative (%) |
X2 |
p-value |
Age group (yrs) |
|
|
|
0.3132 |
0.9575 |
≤25 |
78 |
1 (1.28) |
77 (98.72) |
|
|
26 – 30 |
137 |
2 (1.46) |
135 (98.54) |
|
|
31 – 35 |
147 |
3 (2.04) |
144 (97.96) |
|
|
36 – 40 |
62 |
1 (1.61) |
61 (98.39) |
|
|
≥41 |
18 |
0 (0) |
18 (100) |
|
|
Level of education |
|
|
|
9.391 |
0.0245 |
None |
18 |
1 (5.56) |
17 (94.44) |
|
|
Primary |
26 |
2 (7.69) |
24 (92.31) |
|
|
Secondary |
212 |
3 (1.42) |
209 (98.58) |
|
|
Tertiary |
186 |
1 (0.54) |
185 (99.46) |
|
|
Area of Residence |
|
|
|
|
0.1261 |
Urban |
359 |
4 (1.11) |
355 (98.89) |
|
|
Rural |
83 |
3 (3.61) |
80 (96.39) |
|
|
Birds around the |
|
|
|
|
0.1474 |
Yes |
44 |
2 (4.55) |
42 (95.45) |
|
|
No |
398 |
5 (1.26) |
393 (98.74) |
|
|
Gravidity |
|
|
|
0.1413 |
0.9318 |
Primigravidae |
113 |
2 (1.77) |
111 (98.23) |
|
|
Secundigravidae |
156 |
2 (1.28) |
154 (98.72) |
|
|
Multigravidae |
173 |
3 (1.73) |
170 (98.27) |
|
|
Parity |
|
|
|
|
0.4570 |
Primiparous |
206 |
2 (0.97) |
204 (99.03) |
|
|
Multiparous |
236 |
5 (2.12) |
231 (97.88) |
|
|
Gestational age |
|
|
|
0.7765 |
0.6782 |
1st trimester (1-14weeks) |
142 |
2 (1.41) |
140 (98.59) |
|
|
2nd trimester (15-27weeks) |
186 |
4 (2.15) |
182 (97.85) |
|
|
3rd trimester (≥28weeks) |
114 |
1 (0.88) |
113 (99.12) |
|
|
Variables |
Number tested |
Number positive (%) |
Number negative (%) |
X2 |
p-value |
Reported Fever |
|
|
|
|
0.0118 |
Yes, ≥38ºC at point of |
34 |
3 (8.82) |
31 (91.18) |
|
|
No |
408 |
4 (0.98) |
404 (99.02) |
|
|
Anaemia |
|
|
|
|
0.0018 |
Yes |
41 |
4 (9.76%) |
37 (90.24%) |
|
|
No |
401 |
3 (0.75%) |
398 (99.25%) |
|
|
Body/Skin rash |
|
|
|
|
0.0079 |
Yes |
60 |
4 (6.67) |
56 (93.33) |
|
|
No |
382 |
3 (0.79) |
379 (99.21) |
|
|
Joint/Muscle pain |
|
|
|
|
0.0466 |
Yes |
56 |
3 (5.36) |
53 (94.64) |
|
|
No |
386 |
4 (1.04) |
382 (98.96) |
|
|
Conjunctivitis |
|
|
|
|
0.0058 |
Yes |
8 |
2 (25) |
6 (75) |
|
|
No |
434 |
5 (1.15) |
429 (98.85) |
|
|
Use of ITNs |
|
|
|
|
0.0182 |
Yes |
265 |
1 (0.38) |
264 (99.62) |
|
|
No |
177 |
6 (3.39) |
171 (96.61) |
|
|
Use of mosquito repellants/ insecticide sprays |
|
|
|
|
|
Yes |
258 |
2 (0.78) |
256 (99.22) |
|
0.1334 |
No |
184 |
5 (2.72) |
179 (97.28) |
|
|
Edema of extremities |
|
|
|
|
0.0429 |
Yes |
96 |
4 (4.17) |
92 (95.83) |
|
|
No |
346 |
3 (0.87) |
343 (99.13) |
|
|
Variables |
OR |
RR |
95% C.I |
p-value |
Reported Fever |
9.774 |
|
|
0.0118 |
Yes, ≥38ºC at point of enrolment |
|
9.0 |
2.29 - 34.08 |
|
No |
|
0.1111 |
0.02934 - 0.4367 |
|
Anaemia |
14.34 |
|
|
0.0018 |
Yes |
|
13.04 |
3.32 - 50.14 |
|
No |
|
0.07668 |
0.01994 - 0.3012 |
|
Yes |
|
0.1178 |
0.0303 - 0.4643 |
|
No |
|
|
|
|
Joint/Muscle pain |
5.406 |
|
|
0.0466 |
Yes |
|
5.17 |
1.31 - 19.96 |
|
No |
|
0.1934 |
0.05009 - 0.7635 |
|
Conjunctivitis |
28.6 |
|
|
|
Yes |
|
21.7 |
5.046 - 77.52 |
0.0058 |
No |
|
0.04608 |
0.0129 - 0.1982 |
|
Use of ITNs |
0.108 |
|
|
0.0182 |
Yes |
|
0.1113 |
0.01768 - 0.6966 |
|
No |
|
8.983 |
1.436 - 56.55 |
|
Edema of extremities |
4.971 |
|
|
0.0429 |
Yes |
|
4.806 |
1.216 - 18.86 |
|
No |
|
0.2081 |
0.05303 - 0.8221 |
|
 |
| Figure 1: (Top) A display of material used during surgical endoscopy: an endoscope with a high-definition Full HD camera, a flexible fiber optic cable with a cold light source, -(middle) Use of the endoscope during surgery. -(bottom) Viewing the video in real time on a screen in the operating theatre during surgical endoscopy. |
 |
| Figure 2:A world of fibers. Fibers are everywhere, in every nook and cranny and by their intersecting create microvolumes |
 |
| Figure 3:The vessels of the peritendinous sliding network display different non-linear progression during movement within a homogeneous substance |
 |
| Figure 4: The light emitted by the endoscope is reflected from the glistening facets of the microvolumes |
 |
| Figure 5: The combined action of these three distinct, yet closely related, types of fibrillar behaviour enables the fibrillar network to adapt to the constraint in three dimensions |
 |
| Figure 6: Arterioles, capillaries, venules and nerves all make use of the multimicrovacuolar system for support. This accounts for their seemingly random pattern of distribution |
 |
| Figure 7: Along the fibers, cells are found either in pairs, like ladybirds on a blade of grass, or in small groups |
 |
| Figure 8: Sometimes we see groups of cells called clusters and they contain several million cells |
Introduction
Zika, a flavivirus from the family Flaviviridae [1], has a single stranded RNA [2]. This arthropod-borne virus (arbovirus) [3] is transmitted through the Aedes mosquito species, namely Ae. africanus, Ae. apicoargenteus, Ae. luteocephalus, Ae. aegypti, Ae. vitattus, and Ae. furcifer [4]. Besides vector transmission, the non-vector transmission occurs between the mother and fetus; during transplantation surgeries and hospital stay (nosocomial) [5], and from other substances of human origin (SoHO) [6]. At first the ZIKV infection did not get much consideration as the mild fever, arthralgia, and rash developed in 20% of the cases; while, 80% of the cases were asymptomatic [7]. The virus spreads mostly by the bite of an infected Aedes mosquito or by sexual transmission. In addition, Zika can be passed from a pregnant woman to her fetus, which can cause microcephaly and other severe brain defects [8].
Moreover, majority of people diagnosed with Zika Virus remain asymptomatic, while in symptomatic cases, symptoms (which include, fever, rash, conjunctivitis, headaches and muscle and joint pains), typically start 3-6 days after infection [9,10]. Prevention methodologies will therefore serve as a protective tool and barrier against the spread of the virus. One measure used to protect persons from Zika virus is enforcing proper vector control strategies like adopting use of appropriate nets and counseling in persons living in at risk locations [1,2]. According to estimation, ZIKV infected 3 - 4 million Americans in 2016 and 440000 – 1300000 Brazilians in 2015 [10]. About 2.17 billion people are residents of those areas that are favorable for its dispersal [11]. Since 2015, there has been a dramatic spread of ZIKV in 66 countries, whereas drastic outbreaks were also reported in 44 previously known ZIKV-negative countries [12].
The major threat of today’s world is that the fetus of symptomatic ZIKV infected pregnant female can become the victim of this perilous virus. Usually, the chances of microcephaly are only 7 per 10000 live births [13], however, ZIKV increases this estimation up to several folds. Currently, World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), European Centre for Disease Prevention and Control (ECDC), American Society of Reproductive Medicine (ASRM), and the International Planned Parenthood Federation (IPPF), etc., are the leading organizations that deals with the drastic effects of ZIKV on maternofetal health (1). The Nigerian Center of Disease Control (NCDC) has presented a review of current epidemiology for Zika virus and a risk assessment to the public. Interim recommendations for public health response to Zika virus in Nigeria are also being presented [3].
Nevertheless, in order to address this public health crisis, healthcare providers, pediatricians and community medicine workers are required to be well equipped with effective diagnostic tools and educational material to enhance the public dialogue on the transmission, and effective referral systems that will ensure proper monitoring of the virus [14]. Also, healthcare workers need to be at the forefront with necessary prevention resources in order to avoid the spread of this endemic in Nigerian communities [3]. Thus, it is desirable to include Zika virus diagnosis among other tests for antenatal pregnant attendees for early detection of the virus at point of care to safeguard the unborn child. Therefore, this study aimed to assess the prevalence of Zika virus antibodies and factors implicated with infection among pregnant women accessing care at Obstetrics and Gynecology department of General Hospital, Lagos southwest Nigeria
Methodology
This was a descriptive cross-sectional study involving 442 consecutives pregnant women attending Antenatal clinics at General Hospital Badagry from February 1st to March 28th 2018. Information on Socio-demographic characteristic, reproductive profile and risk factors for contacting Zika Virus will be obtained using questionnaires. About 4mls of blood samples was collected and screened for Zika virus IgG and IgM using Zika virus rapid antigen test Kit. The data was analyzed with SPSS, Version 20.0.
The Audacia Bio Science Zika IgM and IgG rapid tests for specific Zika antibody in serum/plasma or whole blood were used for the in vitro diagnostic assay. This was an immune chromatographic assay for fast and easy detection of the Zika virus antibody and testing was carried out following the manufacturer’s instructions. Briefly the test cassettes were removed from the test card and laid flat on a clean surface. The frozen test samples were kept at room temperature for 20minutes to thaw and thereafter mixed well before running the test. Ten microliter of serum/plasma or whole blood was added to the opened test cassette using a pipette. Following the addition of the sample, three drops of assay buffer were added from the dropper bottle and the results were read within 15-30 minutes. The control line validated the result.
Study Design
This was a descriptive cross sectional study
Description of study area
A surveillance study was carried out among pregnant women visiting the ObGyn department at the General Hospital Badagry, Lagos State Nigeria to assess the burden of Zika virus perceived to be circulating silently in southwest Nigeria using the study area which has large population of pregnant women attending antenatal clinics. The study area is easily accessible in Lagos and presumed to pride relatively cheaper services for the mother to be but with little or no information being provided about the circulation of Zika virus in the study area among the visiting attendees. Badagry is an old ancient area in Lagos with easy accessibility for pregnant women, located at the Badgry local government area under the control of the State Ministry of Health.
Data Collection Tools & Techniques
A structured, semi-validated self-administered application was given to participant after an informed consent had been obtained to gather demographic information and other relevant information. Understanding of the prevalence of zikavirus disease was assessed based on responses to the diagnostic assay and clinical symptoms and patient presentation. There were indications as to which trimester of pregnancy for possible positive Zikavirus pregnant women. Future questions will inquire additional knowledge on how the infection in associated trimesters yielded poor foetal outcomes, whether or not transmission occurs in the absence of a vector, whether the response of the National Institutes of Health (NIH) is timely and sufficient, areas of important research to include impact of exposure to environmental factors and the need for further urgent research in Nigeria.
Ethical considerations
Ethical approval for the study was sought from the hospital Ethical Board Review Committee and respondents’ privacy was made possible by not collecting any data that can identify the participants. Informed consent from each participant was indicated by a check-box on the first page.
Statistical analysis
All statistical analyses were performed using SPSS windows version 20. Categorical variables were described using descriptive statistics (frequencies and percentages). Chi-square (x2) test and Fisher’s exact test (at 95% confidence intervals) were used to test for significant association between the prevalence of Zika virus antibodies and baseline characteristics/ health-related factors among the study subjects. Associations with independent variables of sex, profession, highest qualification obtained and years of practice were determined using chi-square and significance noted at p=0.05%. In cases of significant association, Binary logistics regression was used to test for the strength of association between variables and the strength of such association was expressed by the Odd ratio (OR) and/or Relative risk (RR). Statistical significance was set at P-value < 0.05
Results
Four hundred and seventy-five (475) pregnant women meeting the inclusion criteria were invited to participate in this study, and all of them consented. However, thirty-three [33] decided to discontinue their participation before collection of blood samples. The results presented was based on data from the four hundred and fourty two (442) women whose peripheral blood samples were collected and analysed for Zika virus antibodies. Of the 442 pregnant women examined, seven were positive for Zika virus antibodies with an overall seroprevalence of 1.6% for the study (Table 2).
Socio-demographic profile
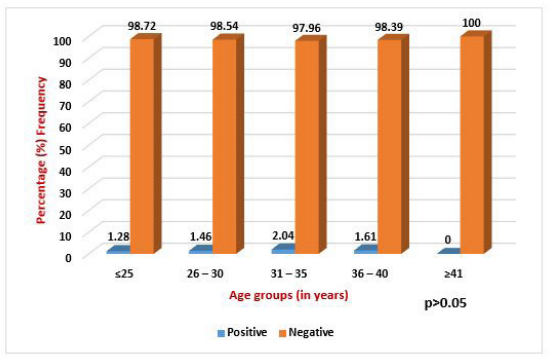
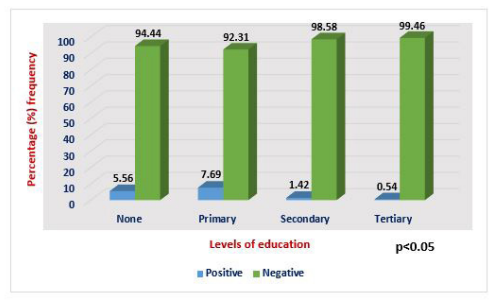
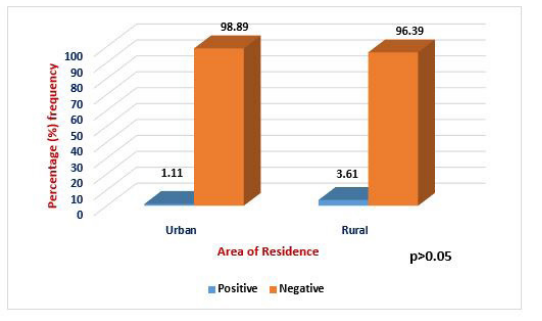
The mean age of the pregnant women was 30.9 years (standard deviation [SD]-6.1; range: 18-48 years) (Table 1). Majority of the participants totaling 212 (47.96%) had completed secondary education while 186 (42.08%) others had tertiary education. A major percentage of the subjects 359 (81.22%) resided in urban areas of Lagos state while only a few 83 (18.78%) resided in rural areas. At the point of enrolment, 34 (7.96%) of them had fever while 408 (92.31%) were without fever. Over a third (39.14%) of the pregnant women were multigravidae (n=173), 156 (35.29%) were secundigravidae while 113 (25.57%) were primigravidae. As for parity status, 236 (53.39%) of the pregnant women were multiparous while 206 (46.61%) were primiparous. A total of 142 (32.13%) were in first trimester, 186 (42.08%) were in second trimester while 114 (25.79%) were in third trimester. Age group 31-35 recorded highest prevalence (2.04%) of Zika virus antibodies while the lowest rate (1.28%) found among age group ≤25 years with no significance difference (P>0.05; X2 =0.3132) between Zika virus infection and age groups. Highest prevalence (7.69%) of zika virus antibodies was among pregnant women who had only primary education while those with secondary and tertiary education had the least prevalences of 1.42% and 0.54% respectively (Figures 1-3). There was a significance difference in the prevalence of zika virus antibodies in relation to level of education (P< 0.05; X2=9.391).
Clinical profiles
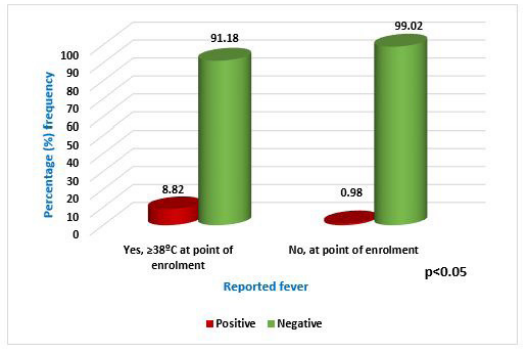
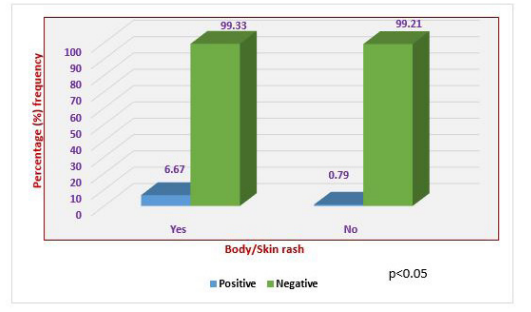
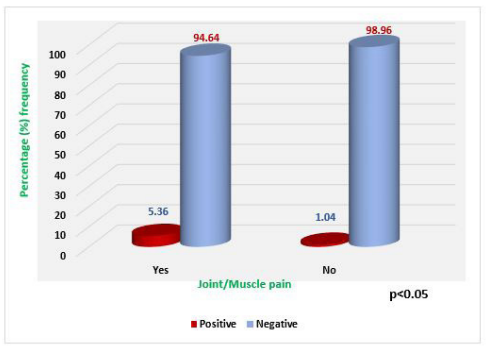
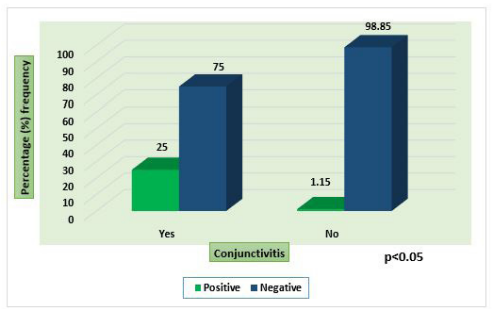
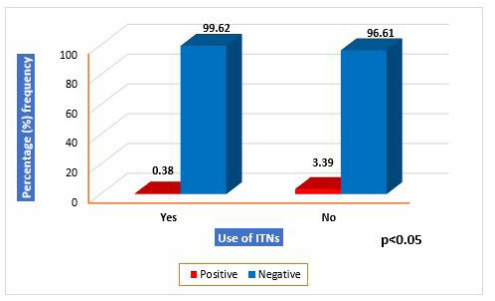
This indicate that 382 (86.43%) did not show any evidence of body rash, 386 (87.33%) subjects had joint/muscle pain while most of the subjects 434 (98.19%) had no conjunctivitis. Also, 346 (78.28%) them had edema of extremities, 41 (9.28%) had moderate and mild anaemia while 401 (90.72%) were not anaemic (Table 3). Prevalence of zika virus antibodies was significantly higher (8.82%) in pregnant women with reported fever at the point of enrolment when compared with women without fever (P< 0.05). Similarly, pregnant women with anaemia had significantly higher prevalence of zika virus antibodies (9.76%) when compared with women without anaemia (p< 0.05). In relation to body/skin rash, the prevalence of zika virus antibodies was significantly higher among pregnant women with reported cases of skin/body rash when compared with pregnant women without body rash (p< 0.05). Pregnant women with body/skin rash recorded a prevalence of 6.67% for zika virus antibodies while those without body rash recorded a prevalence of 0.79%. Prevalence of zika virus antibodies was significantly associated with conjunctivitis (p< 0.05). The prevalence of zika virus antibodies was significantly higher among pregnant with conjunctivitis when compared with those without conjunctivitis (p< 0.05). Pregnant women with joint/muscle pain recorded a prevalence of 5.36% for zika virus antibodies while those without joint/muscle had a prevalence of 1.04%. Pregnant women using ITNs had a reduced prevalence of 0.38% for zika virus antibodies while those who were not using ITNs had a higher prevalence rate of 3.39% for zika virus antibodies but no statistical association (p>0.05). Pregnant women with edema of lower extremities had significantly higher prevalence (4.17%) of zika virus antibodies when compared to women without edema of lower extremities (p< 0.05) (Table 3, Figures 4-8).
Binary logistic regression analysis
This indicates that fever, anaemia, body/skin rash, joint/muscle pain, conjunctivitis, use of ITNs and edema of lower extremities were significantly associated with the prevalence of zika virus antibodies. Pregnant women with fever had increased odds of zika virus infection by 9.8 times than women without fever. Also, the odds of having Zika virus infection increased by 14.34 times higher among pregnant women with anaemia than in others with no anaemia. Pregnant women with body/ skin rash were associated with increased odds of having zika virus infection by 9.02 times than those without body rash. The odds of having zika virus infection increased 5.4 times among pregnant women who reported joint/muscle pain compared to women without joint/muscle pain. Pregnant women with conjunctivitis are more likely to have zika virus infection with an increased odd of almost 29 times more than pregnant women without conjuctivities. The use of insecticide treated nets (ITNs) was significantly associated with the prevalence of zika virus antibodies. Pregnant women who constantly slept under ITNs were 0.11 times less likely to have zika virus infection with a reduced odds of 0.108 compared to women who did not use ITNs. There was also a significant association between edema of lower extremities and zika virus infection. Pregnant women with edema of lower extremities are almost 5 times more probably going to have zika virus infection than those without edema of lower extremities (Table 4).
Discussion
The results from the study indicate exposure levels to Zika virus which suggest the possible circulation of the virus among febrile and asymptomatic patients accessing care at antenatal clinics in Lagos Nigeria with an overall sero-prevalence of 1.6%. The available information from the results generated in this study again indicates noticeable levels of susceptibility to Zika virus infections among the participants. This could mean many infected pregnant women are at risk of giving birth to babies with defects. Congenital Zika virus syndrome may include microcephaly, ventriculomegaly, intracranial calcifications, extra-axial fluid, decreased brain parenchymal volume, lissencephaly, cerebellar hypoplasia, delayed myelination and hypoplasia of the corpus callosum [15,16,17]. Furthermore, newborns of infected mothers can develop cardiac anomalies with septum defects [18,19], seizures due to the underlying brain malformations, neuromotor abnormalities such as spasticity and feeding difficulties [20,21], ocular abnormalities [22] and can be born small for the gestational age [23]. Hence the need to investigate the circulation of Zika virus in expectant mothers with ultimate goal to prevent birth defects will be interesting for further studies in Nigeria.
The overall sero-prevalence of Zika virus antibodies of 1.6% found in this study was consistent with study findings from other African countries which falls within the rates ranging from 0.1% in Gabon and Senegal and as high as 38% in Cameroon [24]. These differences could be due to inconsistency in the study participants’ inclusion criteria or diagnostic test used. Zika virus infection was estimated to affect females and males in a ratio of 2:1 which correlate well with several studies [14,25]. Considering the findings of Mattew et al. [25] with that obtained of this study, there may be gender-related differences in Zika virus infection incidence, which might be due to exposure differences [26]. Nevertheless, our study was only carried out among female participants without any comparison with their male counterparts. Activeness of females during the early hours of the day exposes greater proportion of females to Zika virus-carrying Aedes spp. of mosquitoes either at work or while travelling to and from work especially among pregnant women with higher risk of exposure [8]. This may also be attributed to possible differences in who sought medical care following symptomatic Zika virus infection.
Relatively high prevalence of IgM or IgG of 2.04% found in age group 31–35 compared to ≥41 years and above support data from earlier studies by Mattew et al. [25]. and Kumar et al. [27]. Possible explanation to this observation could be the activeness of age group 31–35 during the early hours of the day which exposes them to the bites of Zika virus-carrying Aedes spp. of mosquitoes more frequently than age group ≥41 years and above with no reported infection rate. This could also suggest female adults manifest with disease less, as they become immune to Zika virus. The proportions of the IgG antibody titers recorded in age group 35–40 and ≥41 years may suggest that, Zika virus infection is not endemic in Lagos Nigeria, rather the virus had been introduced to a non-exposed population as endemicity is attained when the adult infection decreases and only the new entrants into the population are more affected [8,27].
One of the target populations for the public health strategies are pregnant women because of the associated complications that Zika virus infection could have on them and their newborns [28]. Our findings show a prevalence of 1.6% (n = 432) of Zika virus infection among the asymptomatic pregnant women population of Badagry in Lagos, southwest Nigeria which is higher than the 0.1% confirmed cases of Zika virus in asymptomatic women found in Gabon and Senegal but much lower than 20.6% in Ghana while a higher rate of 38% was reported in Cameroon, a neighboring country to Nigeria [14,29]. This supports the evidence of global occurrence of Zika viral infection which suggests that in Africa the circulation of the virus which causes asymptomatic infection in 80% of cases, could be undetected and/or overlooked [24]. The mentioned findings may indicate that there is an underestimation of Zika virus infection that could be explained by the lack of sensitive and specific molecular diagnostic methods in isolated localities. Furthermore, the prevalence in this study highlights the importance of epidemiological surveillance of Zika virus infection in pregnant women that live in newly Zika virus endemic regions such as Lagos. These findings cannot be extrapolated to the Zika virus infection rates among pregnant women in other endemic regions of the world because of the lack of similar molecular diagnostic studies in other sub-Saharan localities [14].
Suggest clinical features of zika virus infection ranged from joint/muscle pain seen in 5.36% (95%CI=1.31–19.96; p=0.0466) in Lagos ante-natal clinic from Joint/Muscle pain presentation (Ambry et al., 2017) of cases to conjunctivitis (25%) OR=28.06; 95%CI =5.046–77.52; p=0.0058) among those with conjunctivitis and this could be due to several reasons. A major possibility is that differences in definitions of symptoms and criteria for Zika virus infection (including the diagnostic test used) could have led to differences in prevalence estimates when compared with Zika endemic regions of the world in which the participants presented with clearly defined symptoms corresponding to higher rates of infection [8,30,31]. This possibility is supported by the lower prevalence of asymptomatic Zika virus infection in pregnant women with confirmed recent infection than in those with possible recent infection of 42% against 63% in a previous study in the United States [32]. Furthermore, in this study, commonly reported symptoms of Zika virus infection documented were fever, muscle pain, joint pain and conjunctivitis. This suggests symptomatic infection among the pregnant women thus confirming the possibility of presumptive diagnosis. In a previous study in the US, prevalence rates of Zika virus infection using presumptive diagnosis was 63% compared with a prevalence of 42% using molecular diagnosis. Patients presenting with clinical features of joint/muscle pain and conjunctivitis could therefore be further evaluated for Zika virus infection using laboratory diagnostic measures. Consequently, conjunctivitis appears statistically significant to be the commonest feature of Zika virus infection with 25% of pregnant women presenting with the symptoms.
Conclusion
The disease caused by Zika virus could be an emerging infection that remains a major public health issue in in Nigeria especially in Lagos due to their endemicity in isolated localities such as Badagry as revealed by the results of this study. This study reports the first confirmed outbreak in the region of Badagry in Lagos Nigeria among asymptomatic pregnant women and describes a low rate of Zika infection in comparison to other hot spot zones of the world such as Brazil and the US. The results obtained are also comparable with what have been reported in some African countries such as Senegal, Algeria and Gambia with low rates of Zika virus infection. The low rate of Zika infection among the asymptomatic pregnant women accessing care at the ante-natal clinics using rapid diagnostic kit could have been higher if more sophisticated diagnostic kits such as ELISA and molecular techniques were available. Therefore, it is advocated that molecular diagnosis of Zika virus infection be included in pregnancy screening programs. This may help to reduce the burden of fetal anomalies associated with the asymptomatic cases
Conflicts of Interest
All authors have declared no conflicts of interest of any kind.
Acknowledgements
We are grateful to the to all the participants, clinicians and paramedical staff of the Obstetrics and Gynecology Department of General Hospital, Lagos State Nigeria for their technical assistance, the administrative support from the head and staff of the Hospital and the State Hospital Management Board.
References
- World Health Organization declares end of Zika emergency. The Irish Times.Retrieved 2016-11-18.
- Rasmussen SA, Jamieson DJ, Honein MA, Petersen LR (2016) Zika Virus and Birth Defects--Reviewing the Evidence for Causality. N Engl J Med 374: 1981-7.
- N. C. F. D. C. (2016, October 1): Public Health Risk Assessment of Zika Virus in Nigeria and Interim Recommendations. Retrieved July 25, 2017, from http://www.ncdc.gov.ng/themes/common/ docs/protocols/12 1478775264.pdf
- Kanki, P (2017) Continued Transmission of Zika Virus in Humans in West Africa, 1992-2016. Journal of Infectious Disease 0000:1-5
- GC Michael, I Aliyu AO Asimi (2017) Knowledge of Zika virus disease among reproductive-age women attending a general outpatient clinic in Northern Nigeria. J South African Family Practice.
- Lucey DR, Gostin LO (2016) The Emerging Zika Pandemic Enhancing preparedness. JAMA 315: 865-6.
- Haddow AD, Schuh AJ, Yasuda CY et al. (2012) Genetic Characterization of Zika Virus Strains: Geographic Expansion of the Asian Lineage. PLoS Neglected Tropical Diseases 6: e1477
- Schwartz KL, Chan T, Rai N, et al. (2018) Zika virus infection in a pregnant Canadian traveler with congenital fetal malformations noted by ultrasonography at 14-weeks’ gestation. Trop Dis Travel Med Vaccines 4: 2.
- Savage HM, Ezike VI, Nwankwo AC, Spiegel R, Miller BR (1992) First record of breeding populations of Aedes albopictus in continental Africa: implications for arboviral transmission. J Am Mosq Control Assoc 8: 101-3. Epub 1992/03/01.
- Wikan N, Smith DR (2016) Zika virus: history of a newly emerging arbovirus. The Lancet Infectious Diseases. 16: e119– 26.
- Dick GW (1952) Zika virus. II. Pathogenicity and physical properties. Transactions of the Royal Society of Tropical Medicine and Hygiene 46: 521-34.
- Simpson DI (1964) ZIKA VIRUS INFECTION IN MAN. Transactions of the Royal Society of Tropical Medicine and Hygiene 58: 335-8.
- Ramzy Austin. Experts Study Zika's Path from First Outbreak in Pacific. The New York Times.Hong Kong. 2016. Retrieved 12 February 2016.
- Ankrah GA, Bonney JHK, Agbosu Pratt D and Adiku KT (2019) Serological evidence of Zika virus infection in febrile patients at Greater Accra Regional Hospital, Accra Ghana. BMC Res Notes 12: 326.
- Soares de Oliveira-Szejnfeld P, Levine D, Melo AS, et al. (2016) Congenital brain abnormalities and Zika virus: what the radiologist can expect to see prenatally and postnatally. Radiology 281: 203.
- Hazin AN, Poretti A, Cavalcanti Souza Cruz D Di, et al. (2016) Computed tomographic findings in microcephaly associated with Zika virus. N Engl J Med 374: 2193.
- Besnard M, Eyrolle-Guignot D, Guillemette-Artur P, et al. (2016) Congenital cerebral malformations and dysfunction in fetuses and newborns following the 2013 to 2014 Zika virus epidemic in French Polynesia. Euro Surveill.
- Cavalcanti DD, Alves LV, Furtado GJ, et al. Echocardiographic findings in infants with presumed congenital Zika syndrome: retrospective case series study. PLoS ONE. 2017;12: e0175065
- Leal MC, Muniz LF, Ferreira TS, et al. (2016) Hearing loss in infants with microcephaly and evidence of congenital Zika Virus infection—Brazil, November 2015–May 2016. MMWR Morb Mortal Wkly Rep 65: 917.
- Miranda-FilhoDde B, Martelli CM, Ximenes RA, et al. (2016) Initial description of the presumed congenital Zika syndrome. Am J Public Health 106: 598.
- França GV, Schuler-Faccini L, Oliveira WK, et al. (2016) Congenital Zika virus syndrome in Brazil: a case series of the first 1501 live births with complete investigation. Lancet 388: 891.
- de Paula Freitas B, de Oliveira Dias JR, Prazeres J, et al. (2016) Ocular findings in infants with microcephaly associated with presumed Zika virus congenital infection in Salvador, Brazil. JAMA Ophthalmol 134: 529-35.
- Meneses JDA, Ishigami AC, de Mello LM, et al. (2017) Lessons learned at the epicenter of Brazil’s Congenital Zika epidemic: evidence from 87 confirmed cases. Clin Infect Dis 64: 1302.
- Saiz JC, Vázquez-Calvo Á, Blázquez AB, Merino-Ramos T, Escribano-Romero E, et al. (2016) Zika virus: the latest newcomer. Front Microbiol 7:496.
- Matthew JL, Rachal MB, Lopez J, Acevedo V, Amador M, et al. (2016) Prevalence of symptomatic Zika virus infection by age and sex—Puerto Rico. J Infect Dis. jix630.
- Kaplan JE, et al. (1983) Epidemiologic investigations of dengue infection in Mexico. Am J Epidemiol. 117: 335-43.
- Kumar M, Sharma R, Parihar G, Sharma M (2015) Seroprevalence of dengue in central Rajasthan: a study at a tertiary care hospital. Int J Curr Microbiol Appl Sci 4: 933-40
- Gupta E, Dar L, Kapoor G, Broor S (2006) The changing epidemiology of dengue in Delhi, India.Virol J 3: 92
- Brasil P, Calvet GA, Siqueira AM, Wakimoto M, de Sequeira PC, et al. (2016) Zika virus outbreak in Rio de Janeiro, Brazil: clinical characterization, epidemiological and virological aspects. PLoSNegl Trop Dis
- Aubry M, Teissier A, Huart M, Merceron S, Vanhomwegen J, et al. (2017) Zika virus seroprevalence, French Polynesia, 2014– 2015. Emerg Infect Dis 23: 669-72.
- Godson Aryee Ankrah, Joseph Humphrey Kofi Bonney, EsinamEudosiaAgbosu, Deborah Pratt & TheophilusKorkuAdiku Serological evidence of Zika virus infection in febrile patients at Greater Accra Regional Hospital, Accra Ghana. BMC Research Notes 12: 326
- Reynolds MR, Jones AM, Petersen EE, Lee EH, Rice ME, et al. (2017) U.S. Zika Pregnancy Registry Collaboration. Vital signs: update on Zika virus-associated birth defects and evaluation of all U.S. infants with congenital Zika virus exposure – U.S. Zika pregnancy registry, 2016. MMWR Morb Mortal Wkly Rep 66: 366-73.
Artcle Information
Review Article
Received Date: October 10, 2021
Accepted Date: November 10, 2021
Published Date: November 10, 2021
Journal of Immunology and Respiratory Medicine
Volume 1 | Issue 1
Citation
Ifeorah IM, Eya JN, Bakarey AS, Ifeorah IK and Onyemelukwe FN (2021) Assessing The Seroprevalence of Zikavirus Antibodies Among Pregnant Women in Selected Health Care Facilities in Lagos Southwestern Nigeria. World J Immunol and Resp Med 1(1):103
Copyright
©2022 Dr. AS Bakarey. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jirm.2022.1.103