

Review Article
Volume-1 Issue-1, 2021
Hypertension, Inadequate Sleep, and Smoking are Commonly Associated with being Overweight and Obese among University Students in India
Received Date: September 12, 2021
Accepted Date: October 12, 2021
Published Date: October 14, 2021
Journal Information
Abstract
Background: Obesity is one of the major global health issues causing significant economic burden in both developed and developing countries. The prevalence of obesity is often associated with lifestyle and family history of obesity or related co-morbidities.
Methods: The study involving 786 volunteers between July 2015 and June 2016 was conducted at the Vellore Institute of Technology, Vellore, India based on a survey questionnaire along with anthropometric measurements, such as height, weight, waist and hip circumference and blood pressure.
Results: Our findings revealed the prevalence of general obesity based on body mass index with 16.2% of the study population categorized as overweight and 29.9% as obese. However, abdominal obesity based on waist circumference and waist-to-hip ratio turned out to be 26.5% and 24.8%, respectively. Hypertension (p < 0.001), high fat/sugar diet in females (p = 0.035), inadequate sleep (p < 0.001), and smoking (p = 0.001) were all observed more frequently among obese individuals who also had a family history of obesity-related medical condition(s) when compared to normal individuals.
Conclusion: Increase in the prevalence of both general and abdominal obesity was influenced by poor food choices, lifestyle changes, and inadequate sleep which pose a serious risk for the development of cardiovascular disorders among young adults in India.
Key words
Obesity; Hypertension; Smoking
S. No. |
State of Origin |
Number of Participants (%) |
1. |
Tamil Nadu |
298 (37.91) |
2. |
West Bengal |
74 (9.41) |
3. |
Maharashtra |
50 (6.36) |
4. |
Kerala |
49 (6.23) |
5. |
Uttar Pradesh |
43 (5.47) |
6. |
Karnataka |
36 (4.58) |
7. |
Andhra Pradesh |
32 (4.07) |
8. |
New Delhi |
30 (3.82) |
9. |
Odisha |
15 (1.91) |
10. |
Madhya Pradesh |
13 (1.65) |
11. |
Bihar |
12 (1.53) |
12. |
Haryana |
11 (1.40) |
13. |
Assam |
10 (1.27) |
14. |
Telangana |
10 (1.27) |
15. |
Gujarat |
8 (1.02) |
16. |
Jharkhand |
7 (0.89) |
17. |
Rajasthan |
7 (0.89) |
18. |
Chhattisgarh |
5 (0.64) |
19. |
**Others |
76 (9.67) |
** Puducherry, Punjab, Uttarakhand, Himachal Pradesh, Tripura, Andaman and Nicobar Islands, Arunachal Pradesh, Meghalaya and undisclosed states
|
Underweight (N = 94) |
Normal (N = 330) |
Overweight (N = 235) |
Obese (N = 127) |
||||
|
Male |
Female |
Male |
Female |
Male |
Female |
Male |
Female |
Age |
19.82 (1.7) |
19.82 (1.94) |
20.16 (2.02) |
20.1 (1.88) |
21.04 (2.65) |
20.41 (1.9) |
21.91 (3.72) |
20.5 (1.89) |
Body weight |
51.7 (5.25) |
44 (7.09) |
61.9 (5.56) |
52 (5.21) |
72.03 (6.06) |
61.61 (6.07) |
89.33 (15.32) |
76.02 (8.88) |
Height |
173 (6.81) |
158 (6.47) |
172 (6.4) |
158.3 (6.65) |
170.22 (6.20) |
158.2 (6.30) |
170.53 (10.79) |
157.84 (5.71) |
BMI |
17.27 (1.07) |
17.14 (0.87) |
20.8 (1.24) |
20.74 (1.21) |
24.83 (1.07) |
24.58 (1.18) |
30.98 (5.28) |
30.51 (3.28) |
WC (cm) |
69.8 (10.88) |
64.5 (8.76) |
76 (4.77) |
71.74 (9.56) |
84.12 (8.84) |
79.98 (15.31) |
99.65 (13.65) |
93.19 (13.71) |
HC (cm) |
79.67 (8.44) |
82.1 (6.99) |
84.6 (5.38) |
87.77 (9.72) |
90.23 (11.04) |
93.84 (12.26) |
103.54 (13.96) |
104.3 (9.99) |
W/H |
0.88 (0.06) |
0.81 (0.19) |
0.9 (0.05) |
0.82 (0.15) |
0.92 (0.10) |
0.86 (0.20) |
0.96 (0.05) |
0.9 (0.18) |
SBP |
116.9 (10.8) |
103 (10.29 |
119.6 (12.2) |
105 (10.71) |
124.5 (12.49) |
108.8 (12.16) |
128.33 (12.13) |
118.8 (11.76) |
DBP |
69.7 (8.4) |
67.13 (8.42) |
68.4 (7.44) |
66.8 (8.44) |
71.98 (8.87) |
71.53 (10.46) |
76.22 (10.27) |
76.54 (9.86) |
BMI: Body mass index; WC: Waist circumference; HC: Hip circumference; W/H: Waist-to-hip ratio; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure
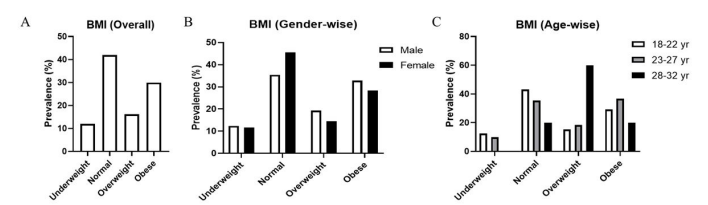 |
| Figure 1: Prevalence of underweight, normal, overweight, and obese individuals based on BMI (A) Overall prevalence between different categories (p = 0.033); (B) Prevalence among males and females (p = 0.041); (C) Prevalence within age groups, 18-22, 23-27, and 28-32 years (p = 0.006) |
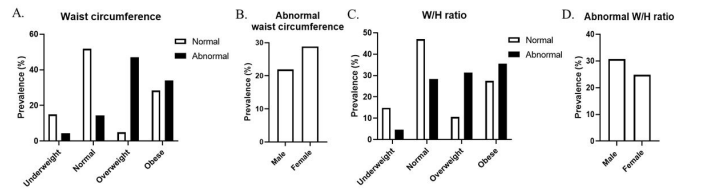 |
| Figure 2: Assessment of abdominal obesity based on WC and W/H ratios (A) Proportion of individuals with normal and abnormal WCs across different categories based on BMI (p < 0.001); (B) Proportion of males and females with abnormal WC; (C) Proportion of individuals with normal and abnormal W/H ratios across different categories based on BMI (p < 0.001); (D) Proportion of males and females with abnormal W/H ratios |
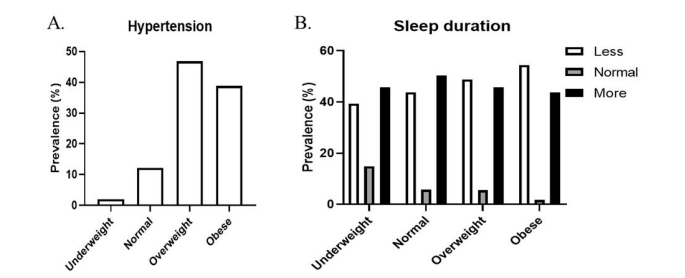 |
| Figure 3:Hypertension prevalence and sleep duration (A) Proportion of individuals with hypertension across different categories (p < 0.001); (B) Proportion of individuals based on their sleep duration across different categories (p < 0.001) |
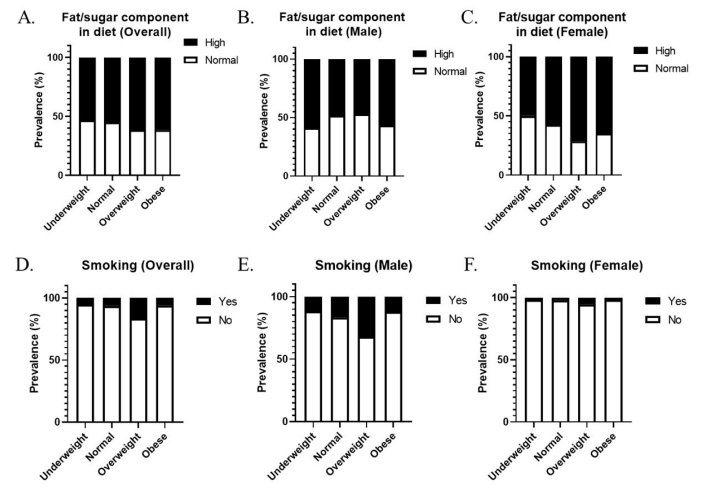 |
| Figure 4: High fat/sugar diet and smoking habit among different categories (A) Overall proportion of individuals consuming high fat/sugar diet across different categories (p = 0.246); (B and C) Proportion of males and females consuming high fat/sugar diet (p = 0.494 & p = 0.035, respectively); (D) Overall proportion of individuals based on their smoking habit (p = 0.001); (E and F) Proportion of males and females based on their smoking habit (p = 0.016 & p = 0.405, respectively). |
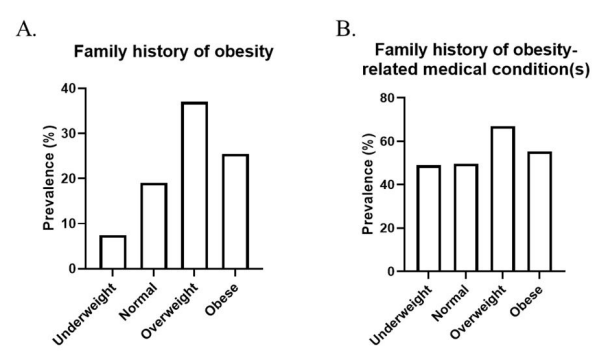 |
| Figure 5: Family history of obesity and obesity-related medical condition(s) (A) Proportion of individuals with a family history of obesity across different categories (p < 0.001); (B) Proportion of individuals with a family history of obesity-related medical condition(s) across different categories (p = 0.007) |
Introduction
Obesity has emerged as one of the major global health problems affecting several millions today. Since 1975, the prevalence of obesity worldwide has almost tripled rising to pandemic proportions. According to a 2016 report by the World Health Organization (WHO), more than 1.9 billion adults, 18 years and older were overweight, of which about 650 million were obese [1]. The global prevalence of overweight and obesity has been projected to reach 2.16 billion and 1.12 billion respectively, by the end of that decade [2]. Apart from malnutrition and infectious diseases, obesity is the major cause for morbidity, mortality, and reduced quality of life throughout the world [3- 5]. In the year 2010, 3.4 million deaths occurred as a result of being either overweight or obese which had contributed to 3.8% of disability-adjusted life years globally [6,7]. Obesity has long been referred to as a medical condition until 2013 when several medical societies, including the American Medical Association and the American Heart Association, classified it as a disease [8]. Obesity is often associated with several other co-morbidities including diabetes, cardiovascular disorders, cancers, dyslipidaemia, reproductive disorders, and liver diseases [4,9,10]. The WHO considers obesity as the fifth major risk factor contributing to the global burden of chronic diseases. Recent studies have also revealed that 44% of diabetes, 23% of cardiovascular disorders, and 7-41% of certain types of cancer could be attributed to overweight and obesity [11].
India being home to a large population of diabetic individuals, both young and old, a sharp increase in the prevalence of obesity has become an alarming public health concern [12- 15]. According to a study conducted on the global burden of diseases in 2013, India has been ranked third for having the most number of obese individuals [16]. INDIAB (India Diabetes), a study conducted in three representative states and one union territory of India during 2008-10 (Phase I) by the Indian Council of Medical Research estimated that 7.33% of the population were overweight while the prevalence of general obesity, abdominal obesity, and combined obesity were 11.25%, 12.92%, and 8.92%, respectively [12]. The financial burden of obesity is huge at the individual, national, and international levels. In 2014, the world gross domestic product incurred an estimated loss of 2.8% due to the disease burden brought by obesity [17,18]. In 2005, India suffered a $9 billion loss in its national income due to the burden of heart diseases, stroke, and diabetes which is expected to increase multi-fold in the near future [19,20].
Obesity is characterized by an unusual body weight gain with serious implications on the normal health of individuals. It results from an abnormal or excessive accumulation of fat in the adipose tissues [21]. Several studies have shown that apart from genetics, epigenetic factors, such as diet, environmental toxins, physical activity, and lifestyle also contribute greatly to the development of obesity [22,23]. During the course of urbanization over the past few decades, wealthy populations have experienced an epidemiological transition towards obesity [24]. Urbanization and modern lifestyle have a very strong and harmful impact among school and university students gravely affecting their overall health. Indeed, urbanization has led to several deleterious changes in lifestyle, physical activity, and calorie intake of the millennials [25,26].
The aim of this study was to assess the prevalence of overweight and obesity and identify possible risk factors among university students in India. It was also conducted to bring awareness about the potential healthcare implications of poor food choices and lifestyle changes in a growing population of young adults in the country.
Participants, Materials, and Methods
Ethical approval
This study was conducted with the approval of the Institutional Ethical Committee for Studies on Human Subjects (Ref.No.VIT/ IECH/02/May23,2014) at the Vellore Institute of Technology (VIT), Vellore, India. It was based on a survey questionnaire along with anthropometric measurements which was carried out after obtaining written informed consent from all the participants as per the guidelines of the Declaration of Helsinki [27].
Study design and human subjects
The study was conducted on university students in VIT Vellore who hailed from different parts of the country (Table 1). While individuals of both genders between the ages of 18 and 32 years were included, pregnant and lactating females as well as foreign nationals were excluded from this study. Participants were divided into three age groups, namely 18-22, 23-27, and 28-32 years comprising of students in bachelor’s, master’s, and doctoral programmes. Between July 2015 and June 2016, a total of 786 volunteers participated in the study which consisted of a survey questionnaire covering different sections related to food habits, awareness about obesity and its risk factors, physical activity, medical history of the individual and their family members, drinking and smoking habits, and socio-economic status. Anthropometric measurements, such as height, weight, waist circumference, hip circumference, and blood pressure were taken using standard procedures (Table 2).
Measurement of body mass index
Height and body weight measurements were done to calculate the body mass index (BMI). A BMI (kg/m2) of < 18.5 is considered as underweight, 18.5-22.9 as normal, 23-26.9 as overweight and > 27 as obese according to the BMI Guidelines for Asians and Asian Americans [28].
Measurement of waist circumference and waist-to-hip ratio
Waist circumference (WC) and hip circumference measurements were done using a non-stretchable measuring tape. The normal cut-off values for WC (cm) and waist-to- hip ratio (W/H) are 90 and 80, and 0.9 and 0.8 for males and females, respectively [29,30].
Measurement of blood pressure
Blood pressure (BP) was recorded using an electronic blood pressure monitor. Individuals with a systolic BP ≥ 140 and/or a diastolic BP ≥ 90 mm Hg were considered as hypertensive [31].
Sleep duration
Based on sleep duration, individuals were categorised into those getting less sleep (< 7 h), normal sleep (7-9 h), and more sleep (> 9 h) based on the recommendations of the National Sleep Foundation [32].
Socioeconomic status
Socioeconomic status was determined based on the annual family income of the participants. It was classified into low (< ₹60,000), lower-middle (₹60,000-₹1,80,000), middle (₹1,80,000-₹6,00,000), upper-middle (₹6,00,000-₹12,00,000) and high-income (> ₹12,00,000) groups.
Statistical analysis
All statistical analysis was performed using SPSS 16.0 software (IBM, Chicago, USA). Descriptive statistics such as percentages for categorical variables and mean ± SD for continuous variables were calculated. Pearson’s chi-squared test was used to find association among variables. Student’s t-test for difference in means was also used. For all the tests, a two-sided p-value of 0.05 or less was considered statistically significant.
Results
Anthropometric analysis
A cross-sectional study on the prevalence of overweight and obesity and associated risk factors was conducted among 786 student volunteers in VIT Vellore. The study consisted of participants in the age group of 18-32 years, except pregnant and lactating females. The study population consisted of 274 males (34.86%) and 512 females (65.14%).
Prevalence of overweight and obesity
General obesity based on BMI revealed 11.96% to be underweight (12.4% male and 11.7% female), 41.98% normal (35.4% male and 45.5% female), 16.2% overweight (19.3% male and 14.5% female), and 29.9% obese (33.8% male and 28.3% female), p = 0.033 and p = 0.041, respectively (Figures 1A and B). A significant difference in the age-wise distribution of individuals across the various BMI categories was observed. While a larger proportion of individuals in the 28-32 and 23-27 age groups were overweight and obese, respectively, majority of the 18-22 age group were normal, p = 0.006 (Figure 1C).
Measurement of WC among participants indicated that 26.5% of the study population had WC values higher than the normal cut-off. The percentage of population with abnormal WC values was significantly higher among the overweight and obese (47.1% and 34.1%, respectively) when compared to the underweight and normal categories (4.3% and 14.4%, respectively), p < 0.001 (Figure 2A). Abnormal WC values were higher among females (28.9%) when compared to males (21.9%) (Figure 2B). On the other hand, 211 participants (24.8%) had W/H ratios higher than the normal cut-off. The percentage of population with abnormal W/H ratios was also significantly higher among the overweight and obese (31.3% and 35.5%, respectively) when compared to the underweight and normal categories (4.7% and 28.4%, respectively), p < 0.001 (Figure 2C). Abnormal W/H ratios were higher among males (30.7%) when compared to females (24.8%) (Figure 2D).
Blood pressure
In the study, 6.23% of the population had hypertension which was more common in the overweight and obese categories, i.e., out of 49 participants with hypertension, 23 were overweight and 19 were obese (46.9% and 38.8%), whereas it was 1 and 6 in underweight and normal categories, respectively (2% and 12.2%), p < 0.001 (Figure 3A).
Sleep duration
It was observed that individuals with higher BMI did not get adequate sleep when compared to others. For instance, the obese category had the lowest number of individuals (1.7%) who slept for the recommended duration (7-9 h), and highest numbers who slept less (< 7 h, 54.5%) when compared to the underweight and normal categories (39.4% and 43.8%). However, the number of individuals who slept for longer duration (> 7 h) did not differ much between the categories, p < 0.001 (Figure 3B).
Food choices
Food preferences, such as vegetarian, non-vegetarian, and fast foods, as well as frequency of fast foods consumed by them were not significantly different across the BMI categories (data not shown). However among females, overweight and obese individuals seemed to prefer a significantly higher proportion of fat/sugar in their diet compared to other foods (71.6% and 64.8%, respectively), p = 0.035 (Figures 4A,B and C).
Alcohol consumption and smoking
While alcohol consumption did not differ significantly between the categories, smoking habit was higher in the overweight category (16.54%) compared to others (5.32%, 6.36%, and 5.96% of underweight, normal, and obese categories, respectively), p = 0.001. Similarly, the proportion of males who smoked was more in the overweight category (32.08%) compared to others (11.76%, 16.49%, and 12.22% of underweight, normal, and obese categories, respectively), p = 0.016. However, this trend was not observed among females, p = 0.405 (Figures 4D,E and F).
Medical history
In the study population, 13.2% had a family history of obesity which was higher among the overweight and obese (37% and 25.53%, respectively) when compared to the underweight and normal categories (7.44% and 19.09%, respectively), p < 0.001 (Figure 5A). On the other hand, 34.7% had a family history of obesity-related medical condition(s) which was also higher among the overweight and obese (66.93% and 55.32%, respectively) when compared to the underweight and normal categories (48.94% and 49.7%, respectively), p = 0.007 (Figure 5B).
Socioeconomic status
Prevalence of obesity among individuals belonging to the high- income group was higher when compared to that of other income categories, although statistically insignificant (p = 0.212).
Discussion
Increasing prevalence of obesity in different parts of the world has made it a major cause of morbidity and mortality, irrespective of age and gender. An alarming rise in its prevalence has also been observed in India over the past couple of decades [12,14,26]. The period when students enter universities is very crucial since reduced parental control gives them enough freedom to explore different kinds of lifestyles that include consuming unhealthy foods thereby posing them at higher risk towards excessive weight gain [33]. Many studies aimed at the prevalence of overweight and obesity among university students have reported that a significant proportion of the population were overweight [34-36]. Overweight or obesity at a young age imposes a serious health threat as it could prolong disability-adjusted life years leading to both reduced quality of life as well as life expectancy [37]. The present study was conducted to assess the prevalence of overweight and obesity and identify possible risk factors among university students in India.
In our study population, we observed the prevalence of both general as well as abdominal obesity based on BMI, WC, and W/H ratio which was found to be higher compared to a previous study [12]. Students when they move from schools to universities far away from their homes often get attracted by the smell and sight of high-calorie, unhealthy, and unhygienic foods that are commonly available in street stalls or nearby restaurants [33]. A large number of students are forced to move out of their hometowns for one reason or another in pursuit of higher education [38]. Individuals staying in hostels are the most affected as they do not have access to home- made healthy foods, unlike junk foods that are easily available [39]. Many of the participants in our study indicated poor food choices and overeating as major causes for their weight gain.
Lack of awareness about obesity and its associated risk factors among our participants could be another reason for the increased prevalence of overweight or obesity reported here. We also found that 13.2% of the study population had a family history of obesity which was more pronounced in the above normal BMI categories. Co-morbidities like type 2 diabetes and heart disease were also found to be more prevalent in the families of individuals with above normal BMI. Alcohol consumption and smoking are risk factors commonly associated with several diseases. While we could not find any significant association between alcohol consumption and obesity, we observed smoking to be significantly associated, especially among males. This is not surprising since the disease risk associated with both of these factors is expected to only increase with age. Although few research studies have reported contradicting associations between alcohol consumption and obesity, it has been recently shown that obesity is associated only with high alcohol consumption [40]. The association with smoking is quite complex as light smokers were less likely to gain weight compared to heavy and non-smokers, whereas ex- smokers showed much more weight gain than all the above mentioned groups [41].
Sleep duration is another factor that has an impact on body weight gain. Many studies have reported a positive correlation between reduced amount of sleep and the prevalence of overweight and obesity [42]. In contrary, longer sleep duration was also found to be associated with obesity [43]. Our study also found that obese individuals slept for less duration compared to the normal ones. Lack of sleep induces appetite and food intake due to alterations in the levels of leptin and ghrelin which regulate energy homeostasis by suppressing or inducing appetite, respectively [44,45]. Shorter sleep duration is also associated with chronic emotional stress, fatigue, and reduced physical activity [46,47].
inducing appetite, respectively [44,45]. Shorter sleep duration is also associated with chronic emotional stress, fatigue, and reduced physical activity [46,47].
Our physical state of being overweight or obese potentially exposes us to a variety of lifestyle-associated illnesses. India being a developing nation harbouring a large population of diabetic individuals and an increasing incidence of cardiovascular disorders, rise in the prevalence of overweight and obesity among young adults is bound to make a serious impact on the healthcare system and government policy. Hence, a periodic assessment of the prevalence and constant public awareness would be necessary for the well-being of society. Our study is an attempt in this direction which clearly indicates a rise in the prevalence of overweight and obesity among young adults compared to some of the studies conducted in the past [12,50-55]. We have also identified poor lifestyle as being the major cause for overweight and obesity which includes poor food choices, inadequate sleep, and smoking that were also reported in other studies. This lifestyle is becoming more and more common among young adults across the world. We also found a significant association between hypertension and obesity which could be of serious concern since it may predispose individuals to cardiovascular disorders in the future. Although our study was limited to a small number of participants belonging to a single academic institute, representation from the various states points to a nationwide trend in overweight and obesity prevalence in the country. However, similar such studies on larger populations could shed more light on the health status and thereby further increase the awareness in the society.
Acknowledgement
The authors would like to acknowledge all the student volunteers and study participants for their contributions to the study and the management of VIT Vellore for their generous sanction of Seed Fund to E.J.R.N.
Conflict of Interest
The authors declare that they have no conflict of interest to disclose with respect to the research study and the data that is published here.
Transparency Declaration
The corresponding author affirms that this manuscript is an honest, accurate, and transparent account of the study being reported. The reporting of this work is compliant with STROBE2 guidelines.
References
- World Health Organization (2013) Obesity and overweight Fact sheet N 311, WHO Media Centre Geneva, Switzerland.
- Kelly T, Yang W, Chen C-S, Reynolds K, He J (2008) Global burden of obesity in 2005 and projections to 2030. International journal of obesity 32: 1431-7
- Alley DE, Chang VW (2007) The changing relationship of obesity and disability, 1988-2004. Jama. 298: 2020-7.
- Flegal KM, Graubard BI, Williamson DF, Gail MH (2007) Cause-specific excess deaths associated with underweight, overweight, and obesity. Jama 298: 2028-37.
- Abdelaal M, le Roux CW, Docherty NG (2017) Morbidity and mortality associated with obesity. Annals of translational medicine 5.
- Lim S, Vos T, Flaxman A (2010) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2224-60.
- Tabarés Seisdedos R (2017) Health effects of overweight and obesity in 195 countries over 25 years. New England Journal of Medicine 377: 13-27.
- Patham B, Mukherjee D, T San Juan Z (2013) Contemporary review of drugs used to treat obesity. Cardiovascular & Hematological Agents in Medicinal Chemistry (Formerly Current Medicinal Chemistry-Cardiovascular & Hematological Agents). 11: 272-80.
- Pischon T, Boeing H, Hoffmann K (2008) General and abdominal adiposity and risk of death in Europe. New England Journal of Medicine 359: 2105-20.
- Kyrou I, Randeva HS, Tsigos C, Kaltsas G, Weickert MO (2018) Clinical problems caused by obesity. Endotext [Internet]. MDText com, Inc., USA.
- Pradeepa R, Anjana RM, Joshi SR (2015) Prevalence of generalized & abdominal obesity in urban & rural India-the ICMR-INDIAB Study (Phase-I)[ICMR-INDIAB-3]. The Indian journal of medical research 142: 139.
- Joshi SR, Parikh RM (2007) India; The Diabetes Capital of the World: Now heading Towards Hypertension. Journal- Association Of Physicians Of India 55: 323.
- Ahirwar R, Mondal PR (2019) Prevalence of obesity in India: A systematic review. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 13: 318-21.
- Young MF, Nguyen P, Tran LM, Avula R, Menon P (2020) A Double Edged Sword? Improvements in Economic Conditions over a Decade in India Led to Declines in Undernutrition as Well as Increases in Overweight among Adolescents and Women. The Journal of Nutrition 150: 364-72.
- Ng M, Fleming T, Robinson M (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 384: 766-81..
- Woetzel J, Dobbs R, Manyika J, Sawers C, Child P, et al. (2014) Overcoming Obesity: An Initial Economic Analysis.
- Tremmel M, Gerdtham U-G, Nilsson PM, Saha S (2017) Economic burden of obesity: a systematic literature review. International journal of environmental research and public health 14: 435.
- Ajay VS, Prabhakaran D (2010) Coronary heart disease in Indians: Implications of the INTERHEART study. The Indian journal of medical research 132: 561.
- Vita-Finzi L (2005) Preventing chronic diseases: a vital investment.
- Alemany M (2011) Utilization of dietary glucose in the metabolic syndrome. Nutr Metab (Lond) 8: 74.
- Herrera BM, Keildson S, Lindgren CM (2011) Genetics and epigenetics of obesity. Maturitas 69: 41-9.
- Imam MU, Ismail M (2017) The Impact of Traditional Food and Lifestyle Behavior on Epigenetic Burden of Chronic Disease. Global Challenges 1: 1700043.
- Guyenet SJ, Schwartz MW (2012) Regulation of food intake, energy balance, and body fat mass: implications for the pathogenesis and treatment of obesity. The Journal of Clinical Endocrinology & Metabolism 97: 745-55.
- Kumanyika S, Libman K, Garcia A (2013) Strategic action to combat the obesity epidemic. Report of the Obesity Working Group.
- Sashindran VK, Dudeja P (2020) Obesity in School Children in India. Public Health in Developing Countries-Challenges and Opportunities. IntechOpen 2020.
- Williams JR (2008) The Declaration of Helsinki and public health. Bulletin of the World Health Organization 86: 650-2.
- Joslin (2014) AADI BMI calculator.
- Committee S (2000) The Asia-Pacific perspective: Redefining obesity and its treatment. Melbourne: International Diabetes Institute, Australia.
- Gupta R, Rastogi P, Sarna M, Gupta V, Sharma S, et al. (2007) Bodymass index, waist-size, waist-hip ratio and cardiovascular risk factors in urban subjects. Japi 55: 621-7.
- Chobanian AV, Bakris GL, Black HR (2003) The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. Jama 289: 2560-71.
- Hirshkowitz M, Whiton K, Albert SM (2015) National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health 1: 233-43.
- de Vos P, Hanck C, Neisingh M, Prak D, Groen H, et al. (2015) Weight gain in freshman college students and perceived health. Preventive medicine reports 2: 229-34.
- Vella-Zarb RA, Elgar FJ (2009) The ‘freshman 5’: a meta- analysis of weight gain in the freshman year of college. Journal of American College Health 58: 161-6.
- Yakusheva O, Kapinos K, Weiss M (2011) Peer effects and the freshman 15: evidence from a natural experiment. Economics & Human Biology 9: 119-32.
- Smith-Jackson T, Reel JJ (2012) Freshmen women and the “Freshman 15”: perspectives on prevalence and causes of college weight gain. Journal of American College Health 60: 14- 20.
- Kitahara CM, Flint AJ, de Gonzalez AB (2014) Association between class III obesity (BMI of 40–59 kg/m 2) and mortality: a pooled analysis of 20 prospective studies. PLoS Med 11: e1001673.
- Chandrasekhar S, Sharma A (2014) Internal migration for education and employment among youth in India. Indira Gandhi Institute of Development Research, Mumbai, India.
- Deliens T, Clarys P, De Bourdeaudhuij I, Deforche B (2014) Determinants of eating behaviour in university students: a qualitative study using focus group discussions. BMC public health 14: 53.
- Traversy G, Chaput J-P (2015) Alcohol consumption and obesity: an update. Current obesity reports 4: 122-30.
- Chiolero A, Faeh D, Paccaud F, Cornuz J (2008) Consequences of smoking for body weight, body fat distribution, and insulin resistance. The American journal of clinical nutrition 87: 801-9.
- Wu Y, Zhai L, Zhang D (2014) Sleep duration and obesity among adults: a meta-analysis of prospective studies. Sleep medicine 15: 1456-62.
- Brady E, Bodicoat D, Hall A (2018) Sleep duration, obesity and insulin resistance in a multi-ethnic UK population at high risk of diabetes. Diabetes research and clinical practice 139: 195-202.
- Taheri S, Lin L, Austin D, Young T, Mignot E (2004) Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med 1: e62.
- Brondel L, Romer MA, Nougues PM, Touyarou P, Davenne D (2010) Acute partial sleep deprivation increases food intake in healthy men. The American journal of clinical nutrition 91: 1550-9.
- Vgontzas AN, Bixler EO (2008) Short sleep and obesity: are poor sleep, chronic stress, and unhealthy behaviors the link. Sleep 31: 1203.
- Patel SR, Malhotra A, White DP, Gottlieb DJ, Hu FB (2006) Association between reduced sleep and weight gain in women. American journal of epidemiology 164: 947-54.
- Lakka H-M, Laaksonen DE, Lakka TA (2002) The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. Jama 288: 2709-16.
- Kini S, Kamath VG, Kulkarni MM, Kamath A, Shivalli S (2016) Pre-hypertension among young adults (20–30 years) in coastal villages of Udupi District in Southern India: An alarming scenario. PloS one 11: e0154538.
- Luhar S, Timæus IM, Jones R (2020) Forecasting the prevalence of overweight and obesity in India to 2040. PloS one 15: e0229438.
- Sharma S, Raina SK, Bhardwaj AK, Chander V, Kumar D, et al. (2013) Utility of consensus statement in assessment of obesity: A study among undergraduate medical students from rural northwest India. Journal of family medicine and primary care 2: 274.
- Ismail B, Anil M (2014) Regression methods for analyzing the risk factors for a life style disease among the young population of India. Indian heart journal 66: 587-92.
- Mukhra R, Kaur T, Krishan K, Kanchan T (2018) Overweight and obesity: a major concern for health in India. La Clinica Terapeutica 169: e199-e201.
- Al Kibria GM, Swasey K, Hasan MZ, Sharmeen A, Day B (2019) Prevalence and factors associated with underweight, overweight and obesity among women of reproductive age in India. Global health research and policy 4: 1-12.
- Thomas E, Geethadevi M (2020) Prevalence and determinants of overweight and obesity among medical students. National Journal of Physiology, Pharmacy and Pharmacology 10: 42-8.
Artcle Information
Review Article
Received Date: September 12, 2021
Accepted Date: October 12, 2021
Published Date: October 14, 2021
Journal of Obesity and Complications
Volume 1 | Issue 1
Citation
Sahu GR, Lankapalli AR, Lakshmi KM, Jayakumar S, Rajkumari R, et al. (2021) Hypertension, Inadequate Sleep, and Smoking are Commonly Associated with being Overweight and Obese among University Students in India. J Obes Comp 1: 1-12
Copyright
©2021 Nelson EJR. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: joc.2022.1.12