

Research Article
Volume-2 Issue-1, 2025
Prevalence and Determinants of Overweight; Obesity; and Weight Gain among Young Women in Costa Rica
Received Date: November 18, 2025
Accepted Date: December 05, 2025
Published Date: December 20, 2025
Journal Information
Abstract
Background: Obesity is a critical public health issue worldwide, with Latin America among the most affected regions. Early adulthood is a key period to prevent excess weight gain, particularly in women.
Methods: We analyzed data from 7,465 women aged 18–25 in the Costa Rica HPV Vaccine Trial. Body Mass Index (BMI) classified overweight (25–29.9) and obesity (≥30). Prevalence was assessed among the same women at baseline (2004/2005) and follow-up (2010/2011). Logistic regression identified determinants of overweight/obesity and ≥20% weight gain.
Results: Prevalence of overweight/obesity increased from 35% to 56% over five years. In adjusted models, older age, lower education, early menarche (≤10years), irregular periods, pregnancies, injectable contraceptive use and smoking increased risk, while being single was protective. Coastal regions had higher prevalence than mountainous areas. Weight gain was associated with early menarche, new pregnancies, oral contraceptive use and marriage, whereas pregnancies before enrollment lowered risk.
Conclusions: Rapid increases in overweight/obesity among young women underscore the influence of social and reproductive factors. Interventions addressing educational and geographic differences are needed. Further studies on diet and physical activity will strengthen prevention and guide public health policy.
Keywords: Epidemiology, Observational Study, Sociodemographic Factors, Reproductive Health, Body Mass Index, Inequities.
Key words
| Characteristics | 2004-2005 Ages 18-25 (N=7465) | 2010-2011 Ages 22-32 (N=5176) | ||
| n | % | n | % | |
| Age | ||||
| 18-19 | 2437 | 32.6 | ||
| 20-21 | 1852 | 24.8 | ||
| 22-23 | 1663 | 22.3 | 1188 | 23.0 |
| 24-25 | 1513 | 20.3 | 1371 | 26.5 |
| 26-27 | 1191 | 23.0 | ||
| 28-29 | 1122 | 21.7 | ||
| 30-32 | 304 | 5.9 | ||
| Marital status | ||||
| Married/Cohabiting | 3076 | 41.2 | 3167 | 61.5 |
| Single/Divorced/Separated/Widowed | 4381 | 58.8 | 1987 | 38.5 |
| No information | 8 | 22 | ||
| Education Level | ||||
| Primary | 2096 | 28.2 | 1521 | 29.5 |
| Lower Secondary | 1697 | 22.8 | 1179 | 22.9 |
| Upper Secondary | 2246 | 30.2 | 1543 | 29.9 |
| University | 1396 | 18.8 | 910 | 17.7 |
| No information | 30 | 23 | ||
| Prevalence overweight/obesity by cantons | ||||
| Low | 573 | 7.7 | 415 | 8.0 |
| Middle | 2461 | 33 | 1696 | 32.8 |
| High | 4431 | 59.4 | 3065 | 59.2 |
| Smoking History | ||||
| Non-Smoker | 6440 | 86.4 | 4168 | 80.9 |
| Ever Smoked | 427 | 5.7 | 655 | 12.7 |
| Currently Smokes | 590 | 7.9 | 331 | 6.4 |
| No information | 8 | 22 | ||
| Menarche | ||||
| ≥14years | 1472 | 19.8 | 1012 | 19.6 |
| 13 years | 1812 | 24.3 | 1239 | 23.9 |
| 12 years | 2315 | 31.1 | 1604 | 31 |
| 11 years | 1293 | 17.4 | 906 | 17.5 |
| ≤ 10 years | 560 | 7.5 | 405 | 7.8 |
| No information | 13 | 10 | ||
| Menstrual Cycle Regularity | ||||
| Regular | 4853 | 65.2 | 3803 | 75.7 |
| Irregular | 2588 | 34.8 | 1218 | 24.3 |
| No information | 24 | 155 | ||
| Number of Pregnancies (Live Births) | ||||
| Nulliparous | 3907 | 52.3 | 1478 | 28.6 |
| 1 | 2192 | 29.4 | 1654 | 32.0 |
| 2 | 952 | 12.8 | 1274 | 24.6 |
| ≥3 | 414 | 5.5 | 770 | 14.9 |
| History of Abortions | ||||
| None | 6933 | 92.9 | 4540 | 87.7 |
| ≥1 | 527 | 7.1 | 636 | 12.3 |
| No information | 5 | 0 | ||
| Use of Oral Contraceptives | ||||
| Never used | 2942 | 39.5 | 927 | 18.2 |
| Used in the pass | 1374 | 18.5 | 2189 | 43.0 |
| Currently using | 3125 | 42 | 1980 | 38.9 |
| No information | 24 | 80 | ||
| Use of Injectable Contraceptives | ||||
| Never used | 5069 | 68.6 | 2426 | 47.7 |
| Used in the past | 1876 | 25.4 | 2044 | 40.2 |
| Currently using | 447 | 6 | 619 | 12.2 |
| No information | 73 | 87 | ||
| BMI Category | 2004-2005 (n = 7,465) | % | 2010-2011 (n=5,176) | % | Cumulative Incidence over Follow-up % | Estimated Annual Incidence % |
| Underweight | 556 | 7.5 | 160 | 3.1 | - | - |
| Normal Weight | 4306 | 57.7 | 2120 | 41.0 | - | - |
| Overweight | 1658 | 22.1 | 1585 | 30.6 | - | - |
| Obesity I | 603 | 8.1 | 785 | 15.2 | - | - |
| Obesity II | 228 | 3.1 | 327 | 6.3 | - | - |
| Obesity III | 114 | 1.5 | 199 | 3.8 | - | - |
| Obesity (all categories combined) | 945 | 12.7 | 1311 | 25.3 | 14.8 | 2.8 |
| Overweight/Obesity (all categories combined) | 2603 | 34.9 | 2896 | 56.0 | 33.1 | 7.0 |
| Characteristics | Overweight/Obesity (%) -2603 | Full Multivariate Model |
| Age | Trend p<0.01 | |
| 18-19 | 25.3 | 1 |
| 20-21 | 31.9 | 1.2 [1.1 - 1.4] |
| 22-23 | 38.8 | 1.4 [1.2 – 1.7] |
| 24-25 | 49.6 | 2.1 [1.8 – 2.5] |
| Marital Status | ||
| Married/Cohabiting | 45.7 | 1 |
| Single/Divorced/Widowed | 27.3 | 0.7 [0.6 - 0.8] |
| Education Level | Trend p<0.01 | |
| University | 25.9 | 1 |
| Upper Secondary | 27.6 | 1.1 [0.9 - 1.3] |
| Lower Secondary | 37.7 | 1.5 [1.2 - 1.8] |
| Primary | 46.3 | 1.8 [1.6 - 2.2] |
| Prevalence overweight/obesity by cantons | Trend p<0.01 | |
| Low | 23.7 | 1 |
| Middle | 32.7 | 1.4 [1.1 - 1.8] |
| High | 37.5 | 1.7 [1.4 – 2.1] |
| Smoking History | Trend p=0.04 | |
| Non-Smoker | 34.4 | 1 |
| Ever Smoked | 37.2 | 1.3 [1.0 - 1.6] |
| Currently Smokes | 38.3 | 1.3 [1.1 - 1.6] |
| Menarche | Trend p<0.01 | |
| ≥ 14 years | 25.0 | 1 |
| 13 years | 29.5 | 1.3 [1.1 - 1.6] |
| 12 years | 36.8 | 2.0 [1.7 – 2.3] |
| 11 years | 42.0 | 2.4 [2.1 – 2.9] |
| ≤ 10 years | 54.6 | 4.3 [3.4 – 5.3] |
| Menstrual Cycle Regularity | ||
| Regular | 34.6 | 1 |
| Irregular | 35.6 | 1.2 [1.1 - 1.4] |
| Number of Pregnancies (Live Births) | Trend p<0.01 | |
| Nulliparous | 25.5 | 1 |
| 1 | 40.2 | 1.2 [1.0 - 1.4] |
| 2 | 50.8 | 1.3 [1.1 - 1.6] |
| ≥3 | 58.5 | 1.4 [1.1 - 1.9] |
| History of Abortions | ||
| None | 33.8 | 1 |
| ≥1 | 48.4 | 1.1 [0.9 - 1.3] |
| Use of oral contraceptives | Trend p=0.81 | |
| Never used | 26.6 | 1 |
| Used in the past | 42.5 | 1.2 [1.0 - 1.4] |
| Currently using | 39.3 | 1.0 [0.9 - 1.2] |
| Use of injectable contraceptives | Trend p=0.38 | |
| Never used | 30.0 | 1 |
| Used in the past | 47.6 | 1.2 [1.1 - 1.4] |
| Currently using | 36.7 | 0.9 [0.7 - 1.1] |
| Characteristics | Δ≥20% (977) % | Full Multivariate Model |
| BMI EV | Trend p<0.01 | |
| Underweight | 25.1 | 1.3 [1.0 – 1.8] |
| Normal weight | 20.3 | 1 |
| Overweight | 18.3 | 0.9 [0.8 - 1.1] |
| Obesity | 10.6 | 0.5 [0.4 - 0.7] |
| Age at EV | Trend p=0.23 | |
| 18-19 | 22.1 | 1 |
| 20-21 | 20.2 | 1.0 [0.9 - 1.3] |
| 22-23 | 16.6 | 0.9 [0.7 - 1.1] |
| 24-25 | 15.0 | 0.9 [0.7 - 1.2] |
| Marital Status EV | ||
| Married/Cohabiting | 15.1 | 1 |
| Single/Divorced/Widowed | 21.8 | 1.0 [0.8 - 1.3] |
| Marital status at M48 | Trend p<0.01 | |
| Without changes in marital status | 15.7 | 1 |
| Separation between EV and M48 | 13.9 | 0.9 [0.6 - 1.2] |
| Married between EV and M48 | 29.2 | 1.8 [1.5 - 2.2] |
| Education Level EV | Trend p=0.24 | |
| University | 20.0 | 1 |
| Upper Secondary | 20.2 | 1.0 [0.8 - 1.3] |
| Lower Secondary | 18.8 | 1.1 [0.9 - 1.4] |
| Primary | 16.8 | 1.1 [0.8 - 1.4] |
| Prevalence overweight/obesity by cantons | Trend p=0.08 | |
| Low | 23.1 | 1 |
| Middle | 20.8 | 0.9 [0.7 - 1.2] |
| High | 17.3 | 0.8 [0.6 – 1.0] |
| Smoking History | Trend p=0.14 | |
| Non-Smoker | 18.3 | 1 |
| Ever Smoked | 22.6 | 1.2 [0.9 - 1.5] |
| Currently Smokes | 19.3 | 1.1 [0.8 - 1.5] |
| Menarche EV | Trend p<0.01 | |
| ≥ 14 years | 15.5 | 1 |
| 13 years | 17.8 | 1.3 [1.0 - 1.7] |
| 12 years | 20.4 | 1.6 [1.3 - 2.0] |
| 11 years | 20.9 | 1.7 [1.3 – 2.1] |
| ≤ 10 years | 20.7 | 1.9 [1.4 – 2.6] |
| Menstrual Cycle Regularity EV | ||
| Regular | 19.0 | 1 |
| Irregular | 18.7 | 1.2 [0.9 - 1.6] |
| Menstrual Cycle Regularity M48 | Trend p=0.56 | |
| Without changes in menstrual cycle | 18.5 | 1 |
| Regular at M48 | 21.5 | 0.8 [0.6 - 1.0] |
| Irregular at M48 | 19.2 | 1.2 [1.0 - 1.5] |
| Number of pregnancies EV | Trend p=0.10 | |
| Nulliparous | 21.9 | 1 |
| 1 | 16.7 | 0.6 [0.5 - 0.8] |
| ≥2 | 14.7 | 0.6 [0.4 - 0.8] |
| Number of pregnancies between EV and M48 | Trend p=0.02 | |
| Nulliparous | 17.7 | 1 |
| 1 | 20.2 | 1.3 [1.1 - 1.7] |
| ≥2 | 17.1 | 1.5 [1.1 – 2.1] |
| History of Abortions EV | ||
| None | 19.0 | 1 |
| ≥1 | 16.9 | 1.4 [0.9 – 2.3] |
| Abortions between EV and M48 | ||
| None | 19.1 | 1 |
| ≥1 | 17.5 | 0.7 [0.5 - 1.0] |
| Use of Oral contraceptives M48 | Trend p<0.01 | |
| Never used | 15.0 | 1 |
| Used in the past | 19.1 | 1.4 [1.1 - 1.7] |
| Currently using | 20.5 | 1.6 [1.2 – 2.0] |
| Use of Injectable contraceptives M48 | Trend p=0.17 | |
| Never used | 18.4 | 1 |
| Used in the past | 18.3 | 1.0 [0.9 - 1.2] |
| Currently using | 22.6 | 1.2 [0.9 - 1.5] |
| BMI Category | 2004-2005 (n = 7,465) | % | 2004-2005 In those who did follow-up visit (n=5,176) | % | 2010-2011 (n=5,176) | % | 2010-2011 with imputation (%) | Cumulative Incidence over Follow-up % | Estimated Annual Incidence % |
| Underweight | 556 | 7.5 | 379 | 7.3 | 160 | 3.1 | 3.1 | - | - |
| Normal Weight | 4306 | 57.7 | 2902 | 56.1 | 2120 | 41 | 42.1 | - | - |
| Overweight | 1658 | 22.1 | 1181 | 22.8 | 1585 | 30.6 | 30.7 | - | - |
| Obesity I | 603 | 8.1 | 448 | 8.7 | 785 | 15.2 | 14.6 | - | - |
| Obesity II | 228 | 3.1 | 173 | 3.3 | 327 | 6.3 | 5.0 | - | - |
| Obesity III | 114 | 1.5 | 93 | 1.8 | 199 | 3.8 | 4.4 | - | - |
| Obesity (all categories combined) | 945 | 12.7 | 714 | 13.8 | 1311 | 25.3 | 24.1 | 14.8 | 2.8 |
| Overweight/Obesity (all categories combined) | 2603 | 34.9 | 1895 | 36.6 | 2896 | 56 | 54.7 | 33.1 | 7.0 |
| Weight Change Category | (N) | % | Cum (%) |
| Weight Loss | 826 | 15.96% | 15.96% |
| Weight Maintenance | 73 | 1.4% | 17.37% |
| Weight gain | 4277 | 82.63% | 100% |
| Total | 5176 | 100% |
| Characteristics | Obesity (%) (N=945) | Full Multivariate Model |
| Age | Trend p<0.01 | |
| 18-19 | 8.8 | 1 |
| 20-21 | 11.1 | 1.2 [1.0 - 1.5] |
| 22-23 | 14.7 | 1.5 [1.2 – 1.9] |
| 24-25 | 18.6 | 2.0 [1.6 – 2.5] |
| Marital Status | ||
| Married/Cohabiting | 17 | 1 |
| Single/Divorced/Widowed | 9.6 | 0.7 [0.6 - 0.9] |
| Education Level | Trend p<0.01 | |
| University | 8.2 | 1 |
| Upper Secondary | 9.6 | 1.2 [1.0 - 1.6] |
| Lower Secondary | 13.3 | 1.5 [1.2 – 2.0] |
| Primary | 18.4 | 2.1 [1.6 - 2.7] |
| Prevalence overweight/obesity by cantons | Trend p<0.01 | |
| Low | 7.5 | 1 |
| Middle | 11.4 | 1.5 [1.0 – 2.1] |
| High | 14 | 1.8 [1.3 – 2.5] |
| Smoking History | Trend p<0.01 | |
| Non-Smoker | 12.2 | 1 |
| Ever Smoked | 15.5 | 1.6 [1.2 – 2.1] |
| Currently Smokes | 16.1 | 1.6 [1.2 – 2.0] |
| Menarche | Trend p<0.01 | |
| ≥ 14 years | 7.3 | 1 |
| 13 years | 10.2 | 1.5 [1.2 – 2.0] |
| 12 years | 13 | 2.1 [1.6 – 2.6] |
| 11 years | 17.4 | 3.0 [2.3 – 3.8] |
| ≤ 10 years | 23 | 4.3 [3.2 – 5.7] |
| Menstrual Cycle Regularity | ||
| Regular | 11.8 | 1 |
| Irregular | 14.3 | 1.4 [1.2 - 1.7] |
| Number of Pregnancies (Live Births) | Trend p=0.92 | |
| Nulliparous | 9 | 1 |
| 1 | 14.7 | 1.1 [0.8 - 1.3] |
| 2 | 19 | 1.0 [0.8 - 1.4] |
| ≥3 | 22 | 1.0 [0.7 - 1.4] |
| History of Abortions | ||
| None | 12.3 | 1 |
| ≥1 | 17.5 | 1.0 [0.8 - 1.4] |
| Use of oral contraceptives | Trend p=0.72 | |
| Never used | 9.6 | 1 |
| Used in the past | 16.3 | 1.1 [0.9 - 1.4] |
| Currently using | 13.9 | 1.0 [0.8 - 1.2] |
| Use of injectable contraceptives | Trend p=0.48 | |
| Never used | 10.5 | 1 |
| Used in the past | 18.5 | 1.3 [1.1 - 1.6] |
| Currently using | 12.3 | 0.8 [0.6 - 1.1] |
| Characteristics | Overweight/Obesity (2896) % | Full Multivariate Model |
| Age | Trend p = 0.000 | |
| 22-23 | 45.8 | 1 |
| 24-25 | 52.6 | 1.3 [1.1 - 1.5] |
| 26-27 | 56.9 | 1.4 [1.2 - 1.7] |
| 28-29 | 65.7 | 2.0 [1.7 - 2.4] |
| 30-32 | 71.1 | 2.5 [1.8 - 3.3] |
| Marital status | ||
| Married/Cohabiting | 61.3 | 1 |
| Single/Divorced/Widowed | 47.6 | 0.8 [0.7 - 0.9] |
| Education Level | Trend p = 0.000 | |
| University | 46.4 | 0.6 [0.5 - 0.7] |
| Upper Secondary | 49.6 | 0.7 [0.6 - 0.8] |
| Lower Secondary | 59 | 0.9 [0.7 - 1.0] |
| Primary | 65.6 | 1 |
| Smoking History | ||
| Non- Smoker | 55.1 | 1 |
| Ever Smoked | 58.3 | 1.1 [0.9 - 1.3] |
| Currently Smokes | 62.8 | 1.4 [1.1 - 1.8] |
| Menarche | Trend p =0.000 | |
| ≥ 15 years | 45.5 | 0.3 [0.2 - 0.4] |
| 14 years | 43.9 | 0.3 [0.2 - 0.4] |
| 13 years | 51.3 | 0.4 [0.3 - 0.5] |
| 12 years | 57.3 | 0.5 [0.4 - 0.7] |
| 11 years | 66.1 | 0.8 [0.6 - 1.1] |
| ≤ 10 years | 71.4 | 1 |
| Menstrual Cycle Regularity | ||
| Regular | 53.9 | 1 |
| Irregular | 61.9 | 1.4 [1.2 - 1.6] |
| Number of Pregnancies | Trend p = 0.097 | |
| Nulliparous | 44 | 1 |
| 1 | 54.6 | 1.1 [0.9 - 1.3] |
| 2 | 62.4 | 1.2 [0.9 - 1.4] |
| ≥3 | 71 | 1.4 [1.0 - 1.8] |
| History of Abortions | Trend p=0.455 | |
| None | 55 | 1 |
| 1 | 62.3 | 0.9 [0.7 - 1.1] |
| ≥2 | 67.4 | 0.9 [0.6 - 1.5] |
| Use of oral contraceptives | Trend p=0.106 | |
| Never used | 44.6 | 1 |
| Used in the past | 61.7 | 1.4 [1.2 - 1.7] |
| Currently using | 55.1 | 1.3 [1.1 - 1.6] |
| Use of injectables contraceptives | Trend p=0.903 | |
| Never used | 50.5 | 1 |
| Used in the past | 62.1 | 1.1 [1.0 - 1.3] |
| Currently using | 56.5 | 0.9 [0.7 - 1.1] |
| Characteristics | Gained 10K+ (1355) % | Full Multivariate Model | ||
| BMI EV | Trend p<0.01 | |||
| Underweight | 19.3 | 0.8 [0.6 - 1.0] | ||
| Normal weight | 23.7 | 1 | ||
| Overweight | 31.5 | 1.6 [1.3 - 1.8] | ||
| Obesity | 31 | 1.6 [1.3 - 1.9] | ||
| Age EV | Trend p=0.33 | |||
| 18-19 | 27.8 | 1 | ||
| 20-21 | 27.7 | 1.1 [0.9 - 1.3] | ||
| 22-23 | 24 | 0.9 [0.7 - 1.1] | ||
| 24-25 | 24.3 | 1.1 [0.8 - 1.2] | ||
| Marital Status EV | ||||
| Married/Cohabiting | 24.1 | 1 | ||
| Single/Divorced/Widowed | 27.8 | 0.9 [0.7 - 1.1] | ||
| Marital status at M48 | Trend p<0.01 | |||
| Without changes in marital status | 22.8 | 1 | ||
| Separation at M48 | 21.5 | 0.8 [0.6 - 1.1] | ||
| Married at M48 | 37.1 | 2.0 [1.7 - 2.4] | ||
| Education Level EV | Trend p=0.46 | |||
| University | 25.5 | 1 | ||
| Upper Secondary | 26.4 | 1.0 [0.8 - 1.2] | ||
| Lower Secondary | 26.9 | 1.1 [0.9 - 1.3] | ||
| Primary | 26 | 1.1 [0.8 - 1.3] | ||
| Prevalence of overweight/obesity by cantons | Trend p=0.083 | |||
| Low | 28.9 | 1 | ||
| Middle | 28.4 | 1.0 [0.8 - 1.3] | ||
| High | 24.6 | 0.8 [0.6 – 1.0] | ||
| Smoking History | Trend p=0.02 | |||
| Non-Smoker | 25.2 | 1 | ||
| Ever Smoked | 31.2 | 1.2 [1.0- 1.4] | ||
| Currently Smokes | 29.3 | 1.3 [1.0 - 1.6] | ||
| Menarche EV | Trend p<0.01 | |||
| ≥ 14 years | 21.7 | 1 | ||
| 13 years | 24.5 | 1.2 [1.0 - 1.5] | ||
| 12 years | 26.7 | 1.3 [1.1 – 1.6] | ||
| 11 years | 30 | 1.5 [1.2 – 1.9] | ||
| ≤ 10 years | 32.4 | 1.7 [1.3 – 2.2] | ||
| Menstrual Cycle Regularity EV Regular | 26.8 | 1 | ||
| Irregular | 25.1 | 1.1[0.9 - 1.4] | ||
| Menstrual Cycle Regularity M48 | Trend p=0.35 | |||
| Without changes in menstrual cycle | 26.3 | 1 | ||
| Regular at M48 | 23.5 | 0.8 [0.6 - 1.0] | ||
| Irregular at M48 | 30.4 | 1.2 [1.0 - 1.4] | ||
| Number of pregnancies EV | Trend p=0.08 | |||
| Nulliparous | 27.4 | 1 | ||
| 1 | 25.9 | 0.7 [0.6 - 0.9] | ||
| ≥2 | 23.5 | 0.6 [0.4 - 0.8] | ||
| Number of pregnancies between EV and M48 | Trend p=0.15 | |||
| Nulliparous | 22.3 | 1 | ||
| 1 | 29.1 | 1.4 [1.1 - 1.7] | ||
| ≥2 | 24.2 | 1.4 [1.1 - 1.9] | ||
| History of Abortions EV | ||||
| None | 26.1 | 1 | ||
| ≥1 | 27.3 | 1.3 [0.9 - 1.9] | ||
| Abortions between EV and M48 | ||||
| None | 26 | 1 | ||
| ≥1 | 27.4 | 0.9 [0.6 - 1.2] | ||
| Use of Oral contraceptives M48 | Trend p=0.007 | |||
| Never used | 20.8 | 1 | ||
| Used in the past | 27.4 | 1.2 [1.0 - 1.5] | ||
| Currently using | 27.5 | 1.3 [1.1 - 1.7] | ||
| Use of injetable contraceptives M48 | Trend p=0.36 | |||
| Never used | 24.3 | 1 | ||
| Used in the past | 27.1 | 1.1 [0.9 - 1.3] | ||
| Currently using | 29.9 | 1.2 [0.9 - 1.4] | ||
| Bolded Odds ratio indicates significant associations at 5% level. EV (enrollment visit), M48 (4-year visit) | ||||
| Full Multivariate model is adjusted for all variables listed in the table. | ||||
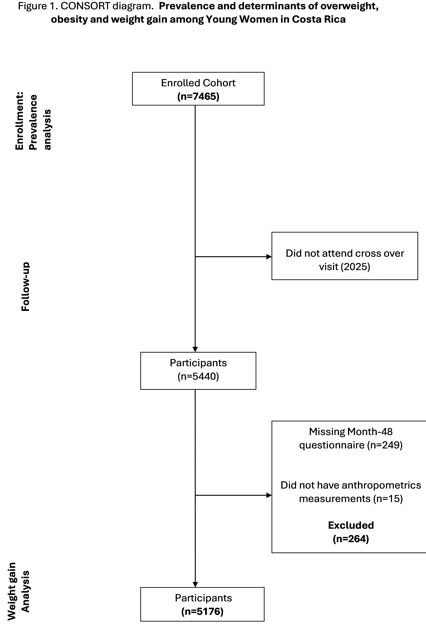 |
| Figure 1: Consort Diagram |
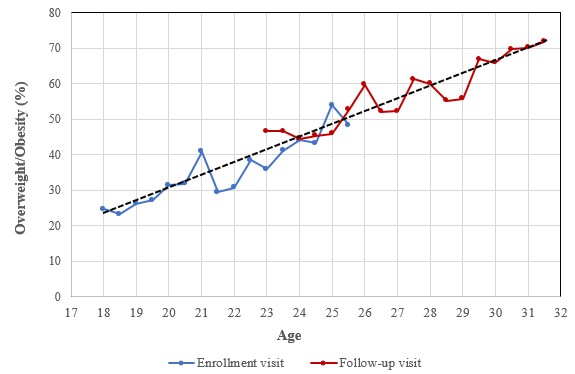 |
| Figure 2: Representation of the percentage of overweight/obesity in relation to age for both studies: |
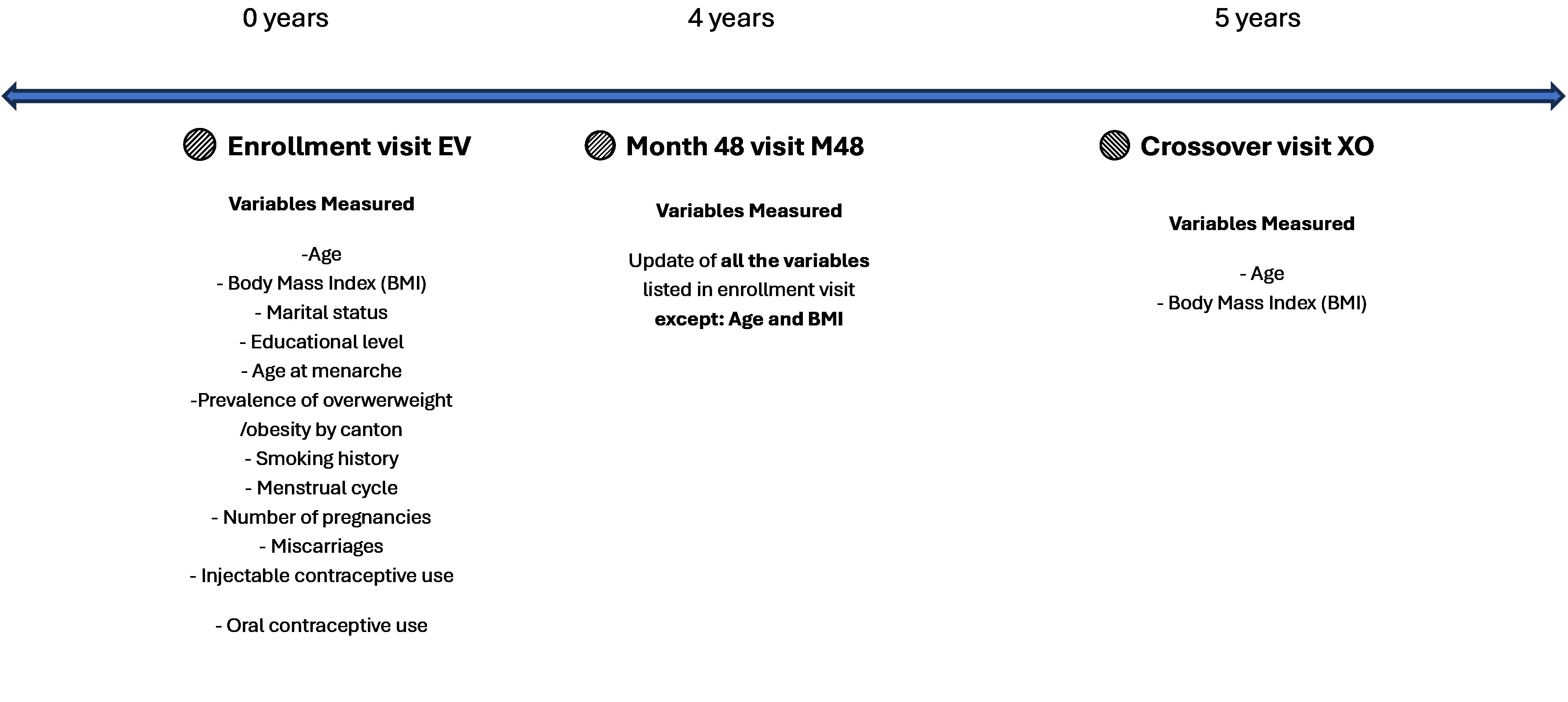 |
| Supplementary Figure 1: Timeline of Data Collection in the original study |
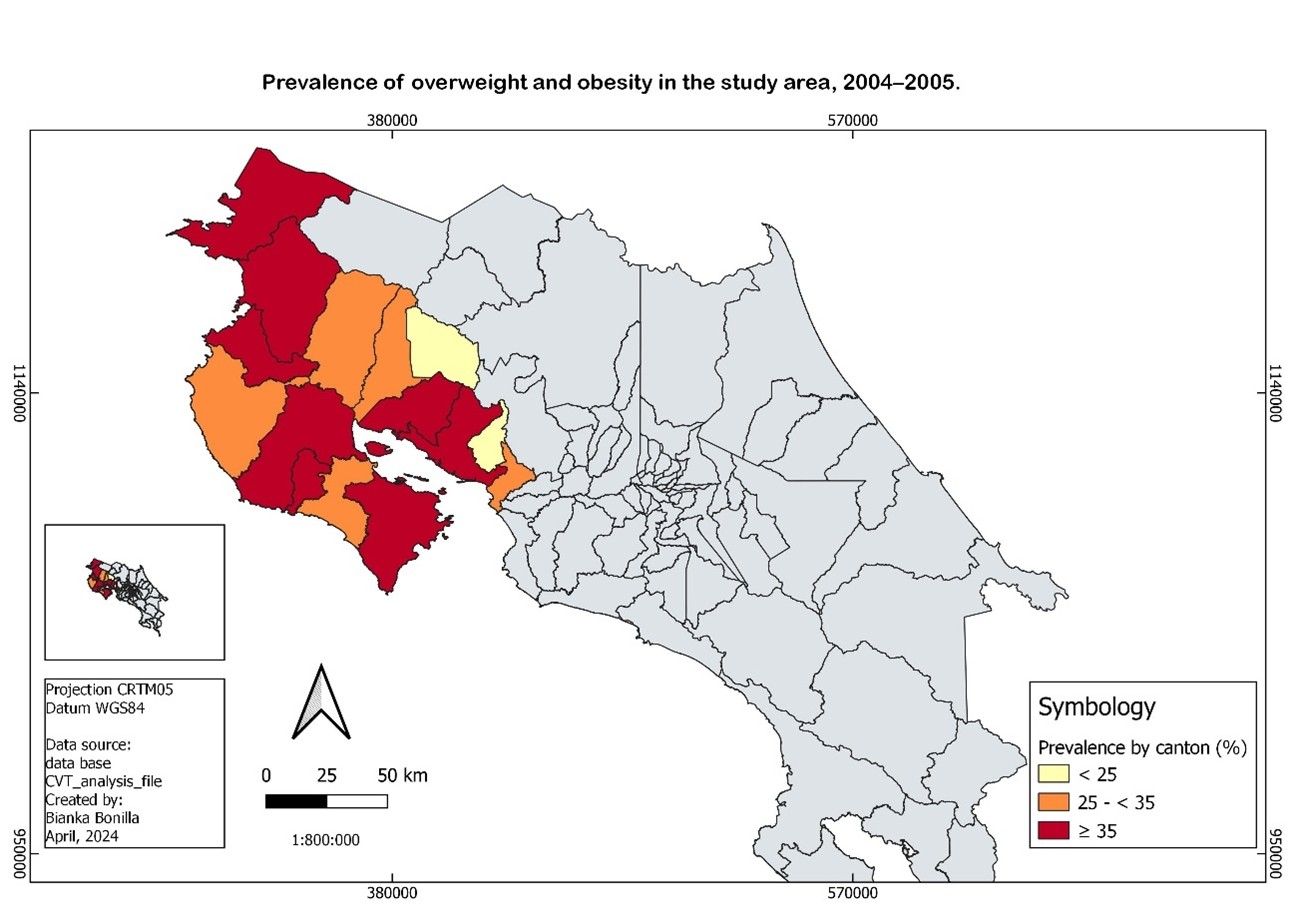 |
| Supplementary Figure 2: Prevalence of overweight/obesity at enrollment visit according to canton of residence |
Introduction
Obesity is a complex, global health crisis characterized by excessive body fat accumulation, that affects individuals with a BMI ≥30 and is associated with type 2 diabetes, heart disease, 13 types of cancer [1], anemia [2], aging [3], increased bone fragility [4], infections, and alterations of the immune system [5]. Furthermore, obesity can affect fertility and influence the quality of life, potentially hampering sleep and mobility [6]. Beyond its direct health implications, obesity is associated with a range of economic consequences, including increased healthcare expenditures and potential productivity losses [7, 8].
The prevalence of overweight and obesity has reached epidemic proportions worldwide. Globally, in 2022, 43% of adults were classified as people with overweight, and approximately 16% as people with obesity [9]. In Latin America and the Caribbean, 63% of adults are people with overweight and 27% are people with obesity [10]. Costa Rica is not exempt from this trend: 63% of adult men and 65% of adult women aged 18 and older are classified as people with overweight [11]. Notably, obesity is more prevalent among Costa Rican women, affecting 34% compared to 25% of men [11]. According to statistics of the Costa Rican Social Security Fund (Caja Costarricense de Seguro Social, CCSS), the Greater Metropolitan Area around the capital exhibits the highest rates of overweight and obesity [12].
The early adult years (18-25) are considered a critical life stage for preventing and controlling weight gain [13]. During this period, individuals undergo significant physical, emotional, and social changes related to education, employment, and personal life, which can create challenges for maintaining a healthy weight [13]. Also, young adults often face a lack of time [14], motivation, and social support [15], which makes it difficult to maintain healthy behaviors. Academic and occupational changes bring challenges that can influence dietary behaviors and food choices. As a result, young adults often adopt less healthy eating patterns and daily activities to maintain a healthy weight [13].
During this critical period of life, women are more likely than men to drop out of sports [16] and interrupt athletic training [17]. Motherhood often reduces the time women dedicate to self-care, including physical activity [14, 18].
Previous research in Costa Rica has examined obesity in the general population [19, 20], but there is limited data on weight gain among young women.
To address this gap, we aimed to assess the prevalence and determinants of overweight and obesity, as well as to evaluate the determinants associated with weight gain in Costa Rican young women between two time points: 2004–2005 and 2010–2011.
Methods
Study Population and Data Collection
Data are from the “Phase III efficacy study of the Human Papillomavirus (HPV) 16/18 vaccine for the prevention of advanced cervical neoplasia associated with HPV 16 or HPV 18”, also known as the Costa Rica Vaccine Trial (CVT). It was a community-based, double-blind, controlled, randomized clinical trial conducted on healthy young adult women from the provinces of Guanacaste and Puntarenas in Costa Rica, recruited from June 2004 to December 2005.
Study methods have been reported [21, 22]. Briefly, CVT enrolled 7465 healthy women aged 18 to 25 years who resided in Guanacaste Province or selected areas of Puntarenas during 2004–2005. Women were included if they were born between July 1978 and November 1987, were able to speak and understand Spanish, appeared mentally competent, and were willing to use contraception. Women were excluded if they had a history of chronic diseases, cervical cancer, a history of hysterectomy, or prior HPV vaccination.
Prospective participants were identified through door-to-door survey. At enrollment participants were randomized to receive the HPV or control (Hepatitis-A) vaccine and were followed annually for 4 years, with high participation rates. At the completion of CVT in 2010, participants were individually unblinded and cross-over vaccination (XO visit) was offered. Participation in enrollment was 30.5% among invited women and 59.1% among eligible women. The study produced extensive information on vaccine efficacy and other aspects of HPV infection and associated conditions.
In addition, we compared selected demographic variables between study participants and women of the same age group and geographic area based on national census data. Compared with the census population, CVT participants had higher educational level, and a lower proportion were married, but the age distribution was very similar, with median ages of 21.0 years in the CVT cohort and 21.1 years in the census population [21].
At enrollment, a physician completed a medical history and physical exam that included measurement of weight and height.
At each visit, from enrollment (EV) through the 48-month follow-up visit (M48), a trained interviewer administered a risk factor interview. The questionnaire asked about years of education, marital status, income, household amenities, menstrual history, sexual, reproductive, and contraceptive history, and smoking status. Blood and cervical specimens were collected at each visit during CVT to evaluate the main objectives of the trial.
After the blinded phase of the study was completed, crossover vaccination was offered. At the first cross-over (XO) visit, the study doctor measured weight. No risk factor questionnaire was administered at the XO visit (Supplementary Figure 1). Therefore, the M48 data were used as the best available approximation of participants’ status at the time of XO. Indeed, the M48 questionnaire represents the closest available risk-factor assessment, with a mean interval of only 1.1 years between M48 and XO. Given this short gap and the relative stability of the risk-factor variables collected in our adult cohort, using M48 responses allows us to reasonably infer participants’ risk profiles at the time of XO.
Figure 1 presents the CONSORT diagram illustrating participant inclusion across the study. A total of 7,465 women were enrolled in the Costa Rica HPV Vaccine Trial (CVT) and included in the prevalence analysis at enrollment. At the cross-over visit, 2,025 participants did not attend. Among those who attended (n = 5,440), 264 were excluded due to missing Month-48 questionnaires (n = 249) or missing anthropometric measures (n = 15), yielding a final analytical sample of 5,176 women.
The prevalence of overweight/obesity was estimated at enrollment (2004–2005) among the 7,465 women and at follow-up (2010–2011) among the 5,176 women who completed the visit, who were also included in the weight gain analysis.
Outcomes
Weight and height were used to calculate body mass index (BMI) at enrollment (2004-2005). At cross over visit (2010–2011), weight was measured, but not height. Given the participant´s age at enrollment (over 18 years), no change in height was expected between enrollment and XO visit. BMI was used to classify participants as underweight (< 18.5), normal weight (18.5-24.9), overweight (25.0-29.9) or obesity (BMI ≥30).
Weight gain was defined by comparing weight at XO and at enrollment. For the analysis, we used a dichotomic indicator describing a relative weight increase >=20% from enrollment to the XO visit. A similar analysis was conducted using a dichotomic indicator describing an absolute weight gain >=10kg.
Independent Variables
For the prevalence analysis, we used sociodemographic, behavioral, hormonal, and reproductive covariates as independent variables strongly associated with BMI previous literature review. Regions were classified into three categories according to their prevalence of overweight/obesity: low (<25%), medium (25% to <35%), and high (≥35%).
For the weight gain analysis, we also added time-dependent covariates, including marital status (separation, marriage), menstrual cycle regularity, and reproductive behaviors (number of spontaneous abortions/pregnancies during follow-up, change in contraceptive use). The information from the interviews applied at enrollment and at the 48-month follow-up visit of CVT was used, since at the XO visit the risk factor questionnaire was not applied.
Statistical Analysis
Association between Age and Overweight/Obesity
The crude association between age and overweight/obesity prevalence was analyzed using both enrollment and cross-over visits. We tested non-linearity associations between age and overweight/obesity prevalence by testing the existence of significant joinpoints [23].
To avoid selection bias, we also impute BMI categories for the 2,289 participants who were not included in follow-up analysis, as a sensitivity analysis. Imputation was based on BMI at enrollment, age and socioeconomic characteristics (including educational level, marital status and age at menarche).
Incidence Rates
We calculated the follow-up incidence rates of overweight and obesity. We also estimated the annual incidence rates of overweight and obesity as the annual risk of developing these conditions, assuming a constant rate of change over the period. The rates were estimated by dividing the number of incident cases of overweight or obesity between enrollment and XO by the total number of person–years of follow-up among participants without overweight or obesity at enrollment.
Determinants of Overweight/Obesity
The analysis of the determinants of overweight/obesity at enrollment included 7,465 women who participated in the enrollment visit. We used a fully adjusted logistic regression model using all the independent variables measured at enrollment. We analyzed the determinants of obesity at enrollment; and the determinants of overweight/obesity at the follow-up visit as complementary analysis.
The analysis of the determinants of weight gain over five years included the 5,176 women who participated in the enrollment and the cross-over visits. We used a fully adjusted logistic regression model using all the independent variables measured at enrollment and at M48.
All statistical analyses were conducted using Stata software version 18.
Results
Table 1 shows the general characteristics of the study participants at both time points (2004–2005 and 2010–2011). Women were between 18 and 25 years old at enrollment and between 22 and 32 years at the follow-up visit (FW). 40% were married at enrollment and 60% at the follow-up visit. The fraction of nulliparous women decreased from 52% at recruitment to 29% at the follow-up visit. At enrollment, most women had used hormonal contraception and 7.9% were current smokers. At enrollment, 28.2% of women had completed primary education, compared with 29.5% at follow-up. Similarly, 59.4% of women resided in cantons with high prevalence of overweight and obesity at enrollment, and 59.2% did so at follow-up. Regarding early menarche, 7.5% reported having had their first menstrual period at age 10 years or younger at enrollment, compared with 7.8% at follow-up. These findings indicate that the distribution of education level, canton of residence, and age at menarche remained essentially unchanged throughout the study period, suggesting the absence of selection bias among the subset of the study population who participated in the follow-up visits included in this analysis.
The prevalence of overweight/obesity at enrollment (2004–2005) was 35% and increased at follow-up (2010–2011) to 56% (Table 2). Among the participants who attended follow-up visit, the prevalence of overweight/obesity at enrolment was similar (37%) (Supplementary Table 1). In addition, the analysis including imputation of missing BMIs produced very similar results (54.7% of overweight/obesity at the follow-up visit), confirming the absence of selection bias (Supplementary Table 1).
The cumulative incidence of overweight/obesity during follow-up was 33.1%, and the cumulative incidence of obesity during follow-up was 14.8%. The annualized incidence of overweight/obesity was 7.0%, and the annualized incidence of obesity was 2.8% (Supplementary Table 1). Participants were classified into three weight change categories during follow-up: weight loss (16.0%), weight maintenance (1.4%), and any weight gain (82.6%) (Supplementary Table 2). 19% experienced a ≥20% BMI increase and 26% had an absolute weight gain of at least 10 kg. These patterns indicate a general shift toward higher BMI categories over the study period.
Figure 2 shows the percentage of overweight/obesity by age. It illustrates the significant increase in overweight/obesity rates with age. The percentage of overweight/obesity is below 25% at 18 years old and above 70% at 31 years old. Percentages of overweight/obesity are similar in the EV and follow-up visits among the overlapping age groups (23-25.5 years old) (p=0.52), suggesting the absence of a secular trend during the study period. In absence of significant joinpoint, the association between age and the prevalence of overweight/obesity can be described as linear.
Supplementary Figure 2 shows the prevalence of overweight and obesity at enrollment by region/canton of residence, revealing significant geographic differences (p<0.01). Prevalence ranged from approximately 23% in the lowest-prevalence areas (Montes de Oro and Tilarán) to around 40% in the highest-prevalence areas (Puntarenas, La Cruz, Hojancha and Liberia).
Table 3 presents the multivariate model of determinants of overweight and obesity at enrollment (2004-2005). It confirms that overweight and obesity significantly increase with age (p-trend<0.01). Single/divorced/widowed women had a lower risk of having overweight/obesity, compared to married women or those in cohabitation (OR = 0.7 [0.6-0.8]). Women with primary level education had a higher risk of having overweight/obesity (OR = 1.8 [1.6-2.2]) compared to those with university level education. The differences across regions still appeared in the fully adjusted model and are therefore not explained by the model's variables. In our population of young adult women, smoking, whether current or past, increased the risk of being overweight and obesity compared to those who had never smoked (OR = 1.3 [1.1-1.6]).
Having an early menarche (≤ 10 years) increases the risk of overweight/obesity compared to those who had late menarche (≥ 14 years) (OR = 4.3 [3.4-5.3], p-trend <0.01). Women who had irregular menstrual periods had a higher risk of having overweight/obesity, compared to women who had regular menstrual cycles (OR = 1.2 [1.1-1.4]). The risk of having overweight/obesity also increased with the number of pregnancies (p-trend<0.01). Women who had ever used injectable contraceptives in the past had a higher risk of having overweight/obesity compared to women who had never used injectable contraceptives (OR = 1.2 [1.1-1.4]), but women who were currently using oral contraceptives did not show higher risk of having overweight/obesity (OR = 0.9 [0.7-1.1]).
The determinants of obesity alone were very similar to the determinants of overweight/obesity (Supplementary Table 3), except that the number of pregnancies was not a significant determinant of obesity. The analysis of determinants of overweight/obesity based on the follow-up visit confirmed the association between overweight/obesity and age, marital status, education level, age at menarche, and regularity of menstrual cycles. At the follow-up visit, overweight/obesity was associated with oral contraceptive, but not with injectable contraception, in opposition to EV visit results (Supplementary Table 4).
Table 4 presents the determinants of weight gain between 2004–2005 and 2010–2011, defined as a ≥ 20% increase in BMI. A total of 977 participants (19%) experienced a ≥ 20% increase in BMI. Women who reported having married between EV and M48 (OR = 1.8 [1.5-2.2]), who had early menarche (OR = 1.9 [1.4-2.6]), who were pregnant during the period (OR = 1.5 [1.1-2.1]) and who use oral contraceptives (OR = 1.6 [1.2-2.0]) had a higher probability of ≥20%-weight gain in the multivariate model. Also, in the fully adjusted model, having been pregnant before the period studied was associated with a lower likelihood of ≥20%-weight gain (OR = 0.6 [0.4-0.8]).
The results from both the relative weight gain model (≥20%) and the absolute weight gain model ≥10kg) were very similar, suggesting consistent associations across both approaches (Supplementary Table 5).
Discussion
In this cohort of 18-25 years old women from Costa Rica, we observed a significant increase in the prevalence of overweight and obesity over five years of follow-up, from 35% at enrollment to 56%. The annual incidence rates were 7.0% for overweight and 2.8% for obesity. Overweight/obesity was associated with older age, lower educational level, early menarche, irregular menstrual periods, pregnancies, past use of injectable contraceptives and smoking history. Being single was associated with a lower risk of overweight and obesity.
Although comparable national data are not available for Costa Rica, international evidence suggests that obesity has increased with earlier onset and greater severity, raising concerns about long-term health consequences beginning in childhood [24, 25].
Older age was also associated with higher prevalence of overweight and obesity in our cohort. Previous research has shown that women between the ages of 18 and 35 experience the most rapid weight gain, with a progressive increase in BMI up to age 35 [26]. This period typically involves hormonal stabilization following adolescence and the onset of important lifestyle changes such as entering the workforce, forming relationships, and reduced engagement in physical activity [16, 26].
Lower educational attainment was another significant predictor of overweight and obesity. Our findings align with prior studies in Costa Rica and other settings, where women with only primary education were more likely to have obesity [27–29]. Education is often correlated with higher socioeconomic status, greater health literacy, and better access to health-promoting resources [16]. However, some studies conducted in Costa Rica have reported no significant differences in anthropometric indicators by education level among adult women [19]. Interestingly, Costa Rican data also show that in childhood, overweight and obesity are more prevalent among those from higher socioeconomic backgrounds, suggesting a possible reversal of the social gradient during the transition to adulthood [30]. An interesting finding of this study is that early menarche (≤10 years) was significantly associated with overweight and obesity. This result is consistent with several previous studies showing that early pubertal timing is linked to greater adiposity, higher BMI, and increased waist circumference throughout adulthood [31–34]. The association may be partly explained by early activation of estrogen and gonadotropin-releasing hormone secretion, which can be triggered by elevated BMI in childhood [35]. However, even after adjusting for childhood BMI, early menarche has been associated with higher adult BMI, suggesting an independent contribution to weight outcomes [36].
Other factors associated with overweight, and obesity included irregular menstrual cycles, recent pregnancies, past use of injectable contraceptives and smoking history. Also, being single was associated with lower likelihood of having overweight or obesity. These associations are consistent with findings from other populations. Menstrual irregularity has been linked to anovulation and excess weight [37]. Pregnancies during follow-up were linked to weight gain, while pregnancies prior to enrollment were not, suggesting that recent pregnancies contributed more strongly to incident overweight and obesity, in line with literature on postpartum weight retention [38, 39]. Past use of injectable contraceptives was also associated with overweight and obesity at enrollment, consistent with studies reporting weight gain linked to hormonal contraceptive use [40-42]. Smoking has been associated with altered eating behavior and weight regulation [43]. Single women were associated with a lower risk of overweight and obesity compared to married women. Women may maintain less healthy eating patterns after entering marriage or cohabitation, regardless of whether they have children [29]. Marriage during follow-up was associated with greater weight gain compared to single women, as previously reported in longitudinal studies that observed increased BMI after entering marriage or cohabitation [26, 44, 45].
We also observed geographic differences in overweight and obesity, with higher prevalence in coastal regions (e.g., Puntarenas, La Cruz) and lower prevalence in mountainous regions (e.g., Montes de Oro, Tilarán). These differences were not explained by the variables included in our models and may relate to population composition or regional environmental factors, as previously described in Costa Rican studies [46–49].
This study, based on a large, population-based trial of young Costa Rican women followed over five years, provides strong evidence of rising overweight and obesity during young adulthood. Its strengths include the large sample size, long follow-up, and consideration of sociodemographic, behavioral, hormonal, and reproductive factors. These findings highlight education, regional disparities, and early-life determinants as critical targets for prevention.
However, limitations include reliance on BMI (which cannot distinguish fat from lean mass), lack of data on diet and physical activity, and restricted generalizability due to study population characteristics and inclusion/exclusion criteria. Given that the CVT sample had a higher level of education than the national census population and considering that the data were collected nearly two decades ago, the reported prevalence of overweight and obesity is likely underestimated and may not fully reflect current population prevalence. Nevertheless, these limitations do not affect the analysis of determinants or the study of weight gain.
Overall, the study demonstrates a significant increase in weight during young adulthood, driven by a complex interplay of sociodemographic, reproductive, behavioral, and regional factors. These patterns highlight the need for more geographically tailored interventions and suggest that hormonal and reproductive determinants merit further investigation. Broader analyses of obesity incidence in women and in the general Costa Rican population would also help contextualize these findings and guide future prevention strategies.
Importantly, these results carry substantial implications for public health policy. Women in this age range are at high risk for developing obesity and related complications, often even before clinical manifestations become evident. This makes early adulthood a critical window for prevention. Our findings underscore the need for targeted interventions such as age-specific obesity screening and postpartum programs to help mitigate long-term weight gain among young women.
Acknowledgements
We are grateful to all the young women of Costa Rica who participated in the CVT study, who gave of themselves in participating in this effort. In Costa Rica, we acknowledge the tremendous effort and dedication of the staff involved in this project; we would like to specifically acknowledge the meaningful contributions by Carlos Avila, Loretto Carvajal, Rebeca Ocampo, Cristian Montero, Diego Guillen and Mario Alfaro. In the United States, we extend our appreciation to the team from Information Management Services (IMS) responsible for the development and maintenance of the data system used in the trial and who serve as the data management center for this effort, especially Jean Cyr, Julie Buckland, John Schussler, and Brian Befano. We thank Dr. Diane Solomon (CVT: medical monitor & QC pathologist) for her invaluable contributions in the design and conduct of the trial and Nora Macklin (CVT) and Kate Torres (LFU) for the expertise in coordinating the study. We thank the members of the Data and Safety Monitoring Board charged with protecting the safety and interest of participants during the randomized, blinded phase of our study (Steve Self, Chair, Adriana Benavides, Ruth Karron, Ritu Nayar, and Nancy Roach) and members of the external Scientific HPV Working Group who have contributed to the success of our efforts over the years (Gypsyamber D’Souza, Chair, Ruanne Barnabas, Karla Chavez, Diane Davey, Michelle Khan, Silvia Lara, Henriette Raventós, Wasima Rida, Richard Roden, Maria del Rocío Sáenz Madrigal, and Margaret Stanley). We thank all the people who worked with a lot of energy and enthusiasm on the original project. ACIB-FUNIN dedicates this study to the memory of our beloved colleague and friend Dr. Paula González Maya, a distinguished researcher in the field of cervical cancer prevention. Dr. González Maya also recognized the importance of addressing emerging public health challenges in cancer prevention and control, including her early suggestion to study the growing epidemic of obesity. Her advice and support are gratefully acknowledged. She passed away on March 26, 2020.
Conflict of Interest Statement
The Costa Rica HPV Vaccine Trial is a long-standing collaboration between investigators in Costa Rica and the NCI. The trial is sponsored and funded by the NCI (contract N01-CP-11005), with funding support from the National Institutes of Health Office of Research on Women's Health. GlaxoSmithKline Biologicals (GSK) provided vaccine and support for aspects of the trial associated with regulatory submission needs of the company under a Clinical Trials Agreement (FDA BB-IND 7920) during the four-year, randomized blinded phase of our study. The NCI and Costa Rica investigators are responsible for the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation of the manuscript. Registered with Clinicaltrials.gov NCT00128661. The authors declare no conflict of interest.
Data Availability
Participant data can be shared with outside collaborators for research to understand more about the performance of the HPV vaccine, immune response to the vaccine, and broader study factors associated with the natural history of HPV infection and risk factors for infection and disease. Outside collaborators can apply to access our protocols and data from the blinded phase of the Costa Rica Vaccine Trial (NCT00128661). For the trial summary, current publications, and contact information for data access see: https://dceg.cancer.gov/research/who-we-study/cohorts/costa-rica-vaccine-trial.
The Costa Rica HPV Vaccine Trial Group:
Bernal Cortés1; Paula González1,10; Rolando Herrero1; Carolina Porras1; Allan Hildesheim2; Aimée R. Kreimer2, Douglas R. Lowy2; Mark Schiffman2, John T Schiller2, Sholom Wacholder2,10, Ligia A Pinto3; Troy J Kemp3; Mary K. Sidawy4; Wim Quint5,10; Leen-Jan van Doorn5; Linda Struijk5; Joel M Palefsky6, Teresa M Darragh6; Mark H Stoler7; Ana Cecilia Rodríguez8; Silvia E Jiménez8; Mark Sherman9
1. Agencia Costarricense de Investigaciones Biomédicas (ACIB), formerly Proyecto Epidemiológico Guanacaste, PEG, Fundación INCIENSA, San José, Costa Rica
2. United States National Cancer Institute, Bethesda, MD, USA
3. Leidos Biomedical Research, Inc., Frederick National Laboratory for Cancer Research, Frederick, MD, USA
4. Medstar Georgetown University Hospital, Washington, DC, USA
5. DDL Diagnostic Laboratory, Netherlands
6. University of California, San Francisco, CA, USA
7. Emeritus, University of Virginia, Charlottesville, VA, USA
8. Independent Consultant, San José, Costa Rica
9. Mayo Clinic, Jacksonville, FL, USA
10. Deceased
Supplementary Information
References
- A Obesity and Cancer | CDC [Internet]. 2021 [cited 2022 Feb 8]. Available from: https://www.cdc.gov/cancer/obesit y/index.htm
- Saad RA, and Qutob HM (2022) The relationship between anemia and obesity. Expert Review of Hematology. 15: 911–26.
- Zannolli R, Mohn A, Buoni S, Pietrobelli A, Messina M, Chiarelli F, et al. (2008) Telomere length and obesity. Acta Paediatrica. 97: 952–4.
- Rinonapoli G, Pace V, Ruggiero C, Ceccarini P, Bisaccia M, Meccariello L, et al. (2021) Obesity and Bone: A Complex Relationship. International Journal of Molecular Sciences. 22: 13662.
- Fariñas Guerrero F, López Gigosos RM (2021) Obesidad, inmunidad y vacunación. Vacunas. 22: 180–8.
- Obesity and overweight [Internet]. [cited 2025 Mar 28]. Available from: https://www.who.int/n ews-room-fa-ct-sheets-detail-obesity-and-overweight
- Dee A, Kearns K, O’Neill C, Sharp L, Staines A, et al. (2014) The direct and indirect costs of both overweight and obesity: a systematic review. BMC Research Notes. 7: 242.
- Burkhauser RV, Cawley J. Beyond BMI (2008) The value of more accurate measures of fatness and obesity in social science research. Journal of Health Economics. 27: 519–29.
- World Health Organization. Obesity and overweight [Internet]. 2024 [cited 2025 Jan 31]. Available from: https://www.who.intnews-roomfact-sheets-detail-obesity-a nd-overweight
- FAO. Panorama regional de la seguridad alimentaria y nutricional - América Latina y el Caribe 2022 [Internet]. FAO; IFAD; PAHO; WFP; UNICEF; 2023 [cited 2024 Apr 22]. Available from: http://www.fao.org/documents/card/es/c/cc3859e s
- Global Nutrition Report | Country Nutrition Profiles - Global Nutrition Report [Internet]. 2022 [cited 2025 Jan 31]. Available from: https://globalnutritionreport.org/resource s/nutrition-profiles/
- Evans-Meza DR, Bonilla-Carrión R, Salvatierra-Durán DR, González-Picado L. SALUD EN PERSPECTIVA N 12 UNIVERSIDAD HISPANOAMERICANA UNIDAD DE INVESTIGACIÓN. ESCUELA DE MEDICINA. 2023;
- Lanoye A, Brown KL, LaRose JG (2017) The Transition into Young Adulthood: A Critical Period for Weight Control. Curr Diab Rep. 17: 114.
- Evenson KR, Aytur SA, Borodulin K (2009) Physical activity beliefs, barriers, and enablers among postpartum women. J Womens Health (Larchmt). 18: 1925–34.
- Nelson MC, Kocos R, Lytle LA, Perry CL (2009) Understanding the Perceived Determinants of Weight-related Behaviors in Late Adolescence: A Qualitative Analysis among College Youth. Journal of Nutrition Education and Behavior. 41: 287–92.
- Lunn PD (2010) The sports and exercise life-course: A survival analysis of recall data from Ireland. Social Science & Medicine. 70: 711–9.
- Mazerolle SM, Eason CM, Pitney WA, Mueller MN (2015) Sex and Employment-Setting Differences in Work-Family Conflict in Athletic Training. J Athl Train. 50: 958–63.
- Bellew - Women and Girls in Sport, Active Recreation & Phys.pdf [Internet]. [cited 2025 Mar 31]. Available from: https://www.sport.nsw.gov.au/sites/default/files/2021-04/sprinter- omen_and_girls_participation_review_final.pdf
- Gómez Salas G, Quesada Quesada D, Monge Rojas R, Gómez Salas G, Quesada Quesada D,et. al (2020) Perfil antropométrico y prevalencia de sobrepeso y obesidad en la población urbana de Costa Rica entre los 20 y 65 años agrupados por sexo: resultados del Estudio Latino Americano de Nutrición y Salud. Nutrición Hospitalaria. 37: 534–42.
- Pabón CA, Hubley E, Spurrell G, Smoczyk M. OBESIDAD: Análisis de la prevalencia de obesidad y sobrepeso en una población de adultos con bajos ingresos en Costa Rica. CS [Internet]. 2021 Apr 16 [cited 2025 Mar 14]; 5(2). Available from: http://revista cien ciaysa lud.ac.cr/ojs/inde x.php/cien ciay sal ud/article/view/244
- Herrero R, Hildesheim A, Rodríguez AC, Wacholder S, Bratti C, Solomon D, et al. (2008) Rationale and design of a community-based double-blind randomized clinical trial of an HPV 16 and 18 vaccine in Guanacaste, Costa Rica. Vaccine. 26: 4795–808.
- Gonzalez P, Hildesheim A, Herrero R, Katki H, Wacholder S, Porras C, et al. (2015) Rationale and design of a Long Term Follow-up study of women who did and did not receive HPV 16/18 vaccination in Guanacaste, Costa Rica. Vaccine. 33: 2141–51.
- Joinpoint Regression Program [Internet]. [cited 2025 Sept 5]. Available from: https://sur veil lance.ca ncer.gov/jo in po int/
- Ng M, Dai X, Cogen RM, Abdelmasseh M, Abdollahi A, Abdullahi A, et al. ( 2024) National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990–2021, and forecasts up to 2050. The Lancet. 404: 2278–98.
- Cunningham SA, Hardy ST, Jones R, Ng C, Kramer MR, Narayan KMV (2022) Changes in the Incidence of Childhood Obesity. Pediatrics. 150: e2021053708.
- Pegington M, French DP, Harvie MN (2020) Why young women gain weight: A narrative review of influencing factors and possible solutions. Obesity Reviews. 21: e13002.
- 2023 - Panorama regional de la seguridad alimentaria y nu.pdf [Internet]. [cited 2024 Apr 22]. Available from: https://www.fao.org/3/cc3859es/cc3859es.pdf
- HLPE_2017_Nutrition-and-food-systems [Internet]. [cited 2024 Apr 22]. Available from: https://www.fao.org/filead min/user_upload/hlpe/hlpe_documents/HLPE_S_and_R/HL PE _2017_Nutrition-and-food-systems_S_R-ES.pdf
- Montero-López M, Santamaría-Ulloa C, Bekelman T, Arias-Quesada J, et al. (2021) Determinantes sociales de la salud y prevalencia de sobrepeso-obesidad en mujeres urbanas, según nivel socioeconómico. Hacia la Promoción de la Salud. 26(2):192–207.
- Gamboa-Gamboa T, Fantin R, Cordoba J, Caravaca I, Gómez-Duarte I (2021) Relationship between childhood obesity and socio-economic status among primary school children in Costa Rica. Public Health Nutr. 24: 3825–33.
- Dreyfus J, Jacobs DR, Mueller N, Schreiner PJ, Moran A, Carnethon MR, et al. (2015) Age at menarche and cardiometabolic risk in adulthood: the Coronary Artery Risk Development in Young Adults Study. 167: 344-52.
- Żurawiecka M, Wronka I (2020) Association between age at menarche and body mass index, waist circumference, waist to hip ratio, and waist to height ratio in adult women. Am J Hum Biol. 21: e23523.
- Gemelli IFB, Farias E dos S, Souza OF (2016) Age at Menarche and Its Association with Excess Weight and Body Fat Percentage in Girls in the Southwestern Region of the Brazilian Amazon. Journal of Pediatric and Adolescent Gynecology. 29: 482–8.
- Rosenberg L, Palmer JR, Wise LA, Horton NJ, Kumanyika SK, Adams-Campbell LL (2003) A Prospective Study of the Effect of Childbearing on Weight Gain in African-American Women. Obesity Research. 11: 1526–35.
- Cho H, Han JW (2023) Obesity-Related Factors in Adult Women with Early Menarche. Healthcare. 11: 557.
- Gaml-Sørensen A, Brix N, Ernst A, Lunddorf LLH, Arah OA, Strandberg-Larsen K, et al. (2025) Pubertal timing and tempo and body mass index trajectories: investigating the confounding role of childhood body mass index. American Journal of Epidemiology. kwaf063.
- Brewer CJ, Balen AH (2010) The adverse effects of obesity on conception and implantation. Reproduction. 140: 347–64.
- Hollis JL, Crozier SR, Inskip HM, Cooper C, Godfrey KM, Harvey NC, et al. (2017) Modifiable risk factors of maternal postpartum weight retention: an analysis of their combined impact and potential opportunities for prevention. Int J Obes. 41: 1091–8.
- Endres Lk, Straub H, Mckinney C, Plunkett B, Minkovitz Cs, Schetter Cd, et al. (2015) Postpartum Weight Retention Risk Factors and Relationship to Obesity at One Year. Obstet Gynecol. 125: 144–52.
- Simmons KB, Edelman AB (2016) Hormonal contraception and obesity. Fertility and Sterility. 106: 1282–8.
- Endalifer ML, Diress Alen G, Addisu A, Linger B (2020) The association between combined oral contraceptive use and overweight/obesity: a secondary data analysis of the 2016 Ethiopia Demographic and Health Survey. BMJ Open. 10: e039229.
- Metz L, Isacco L, Redman LM (2022) Effect of oral contraceptives on energy balance in women: A review of current knowledge and potential cellular mechanisms. Metabolism. 126: 154919.
- Ely AV, Wetherill RR (2023) Reward and inhibition in obesity and cigarette smoking: Neurobiological overlaps and clinical implications. Physiol Behav. 260: 114049.
- Liu J, Garstka MA, Chai Z, Chen Y, Lipkova V, Cooper ME, et al. (2021) Marriage contributes to higher obesity risk in China: findings from the China Health and Nutrition Survey. Annals of Translational Medicine. 9: 564–64.
- Jeffery RW, Rick AM (2002) Cross-Sectional and Longitudinal Associations between Body Mass Index and Marriage-Related Factors. Obesity Research. 10: 809–15.
- Wang Z, Hildesheim A, Wang SS, Herrero R, Gonzalez P, Burdette L, et al. (2010) Genetic Admixture and Population Substructure in Guanacaste Costa Rica. PLOS ONE. 5: e13336.
- Guevara-Villalobos D, Céspedes-Vindas C, Flores-Soto N, Úbeda-Carrasquilla L, et al. (2019) Hábitos alimentarios de la población urbana costarricense. Acta Médica Costarricense. 61: 152–9.
- Gómez Salas G, Quesada D, Chinnock A (2020) Consumo de frutas y vegetales en la población urbana costarricense: Resultados del Estudio Latino Americano de Nutrición y Salud (ELANS)-Costa Rica. Población y Salud en Mesoamérica. 18: 450–70.
- Indice-de-Desarrollo-Humano-Cantonal-y-su-Ajustes-por-el-PIB-Ajuste-datos-al-2023.pdf [Internet]. [cited 2025 Mar 12]. Available from: https://ci odd.ucr.ac.cr/wp-con tent/uplo ads/2023/09/Indi ce-de-Desarrollo-Hum ano-Can tonal-y-su-Ajus tes-por-el-PIB-Ajuste-datos-al-2023.pdf
Article Information
Research Article
Received Date: November 18, 2025
Accepted Date: December 05, 2025
Published Date: December 20, 2025
Prevalence and Determinants of Overweight; Obesity; and Weight Gain among Young Women in Costa Rica
Volume 2 | Issue 1
Citation
Bianka Bonilla, Romain Fantin, Carolina Porras, Juan Carlos Vanegas, Juan José Romero-Zúñiga (2025) Prevalence and not Prevalence and Determinants of Overweight; Obesity; and Weight Gain among Young Women in Costa Rica.J Obes Comp 1: 1-24
Copyright
©2025 Bianka Bonilla. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: joc.2025.2.101