

Review Article
Volume-1 Issue-1, 2021
Coracoid Fracture in Paediatric Patients Case Report and Revision of The Literature
Received Date: September 11, 2021
Accepted Date: October 11, 2021
Published Date: October 12, 2021
Journal Information
Abstract
The coracoid fracture in paediatric patients is extremely rare. It might be underlined only with specific radiographic projections. The clinic case set out in this article shows that the conservative treatment in paediatric patients, as reported in literature, is the choice’s treatment.
Key words
fracture, coracoid, paediatric patients.
 |
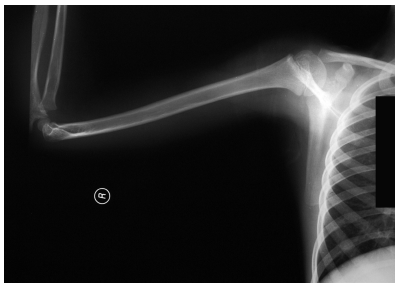
| Figure 1a: standard x-ray carried-out in the emergency room |
 |
| Figure 1b:standard x-ray carried-out in the emergency room |
 |
| Figure 2:specific projections of the left shoulder |
 |
| Figure 3a: good consolidation of the fracture and his realignment |
 |
| Figure 3b: good consolidation of the fracture and his realignment |
Introduction
The coracoid fracture is absolutely a rare event. Even more rare in paediatric patients [1]. The literature, in fact, reports few cases: most of them in adulthood [2], whereas are limited the reports below the 14 years of age [3].
Clinic case
Male, 7 years and 9 months old; fell from the dad’s motorbike hitting on the floor the right shoulder. Reached the emergency room immediately after the trauma. At the clinical examination presented swelling and deep pain at the pressure on the coracoid and all over the shoulder; the motility was good but it reawaken/stirred pain in particular in abduction. The standard x-ray carried-out in the emergency room suspecting a fracture of the clavicle or humerus (figureure 1 a-b) underlined a light discontinuity at the base of the right coracoid, centering of the humeral head and continuity of the acromio-clavicular joint. Are requested the specific and comparative projections of the left shoulder (figureure 2 a-b) that highlights the separation of the coracoid base with small compound fracture. Is decided for a conservative treatment by applying Desault bandage for 25 days. At the removal, the clinic examination shows light pain at the mobilization of the shoulder and at the pressure on the coracoid. The radiographic exam points out good consolidation of the fracture and his realignment (figureure 3 a-b). At the clinic follow-up after 20 days after the removal of the bandage, the patient does not complain any pain and presents a complete motility of the shoulder.
Discussion
The coracoid fracture is reported mainly in adulthood, rarely isolated [4-5], much more frequently associated to others injuries such as the dislocation of the acromio-clavicular joint in different scales [3, 6] dislocation6 or instability of the shoulder7, fracture of the clavicle or of the glenoid cavity [2], injury of the rotator-cuff6 or fracture of the acromion5.
Two classifications are proposed depending on the level of the fracture. Ogawa6 divides into two types related to the joint of the coraco-clavicular ligament: the type I behind them and the type II front of them. This subdivision it would be useful, according to the author, for the purpose of the treatment:
type II fractures, stables, would have more indication to the conservative treatment while the type I, more unstable, would have a surgical stabilization.
Saragaglia7 divides them into 3 types recognising to each of them a particular traumatic association: fracture of the coracoid base (associated to a dislocation of the acromio- cavicular joint), fracture of the horizontal part (associated to an instability of the shoulder) and fracture-avulsion of the coracoid apex (injuries apparently isolated).
It has a low visibility in standard x-rays [7], [1] and so it has to be researched with specific projections such as the “Stryker– notch view” [8].
Conclusion
The coracoid fracture is absolutely a rare event especially in paediatric patients. In these patients, conservative treatment must be taken in consideration particularly in isolated trauma.
References
- Rockwood CA, Wilkins KE, King RE (1991) Fractures in children. J.B.Lippincott Company, Philadelphia [892-3].
- Martin-Herrero T, Rodriguez-Merchan C, Munuera-Martinez L (1990) Fractures of the coracoid process: presentation of seven cases and review of the literature. J. Traum 30: 1597-9.
- Taga I, Yoneda M, Ono K (1986) Epiphiseal separation of the coracoid process associated with acromioclavicular sprain (A case report and review of the literature). Clin. Orthop. Relat. R 207: 138-41.
- Farfan Gil J, Haydar A (1991) Isolated Injury of the coracoid process: case report. J. Traum 31: 1696-7.
- Zilberman Z, Rejovitzky R (1981) Fracture of the coracoid process of the scapula. Injury 13: 203-6.
- Ogawa K, Yoshida A, Takahashi M, Ui M (1997) Fractures of the coracoid process. J. Bone Joint Surg B 17-9.
- Saragaglia D, Picard F, Gerard P, Tourne Y, Leroy JM (1994) Anterior shoulder instability associated with the fracture of the coracoid process. About three cases. Rev. Chir. Orthop 80: 651-5.
- Hall RH, Isaac F, Booth CR (1959) Dislocation of the shoulder with special reference to accompanying small fractures. J. Bone Joint Surg 41-A: 489-94.
Artcle Information
Review Article
Received Date: September 11, 2021
Accepted Date: October 11, 2021
Published Date: October 12, 2021
Journal of Pediatric Care and Neonatology
Volume 1 | Issue 1
Citation
Giorgio Marrè Brunenghi (2021) Coracoid Fracture in Paediatric Patients Case Report and Revision of The Literature. J Pediatr Care Neonatol 1: 1-6
Copyright
©2021 Giorgio Marrè Brunenghi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jpcn.2022.1.102