

Review Article
Volume-1 Issue-1, 2021
Lymphedema: Old and New Ideas Concerning Treatment
Received Date: November 28, 2021
Accepted Date: December 28, 2021
Published Date: December 30, 2021
Journal Information
Abstract
Lymphedema is a progressive disease and also a major contributor to disability and social isolation. Major causes include cancer therapy (surgical removal of lymph nodes and/or irradiation), as well as parasitic disease fillariasis, damage of the skin caused by exposure to irritant soils known as podoconiosis and repeated episodes of lymphangitis. Excess protein-rich fluid accumulation occurs in the affected limb (pitting edema), which is considered as free, if it can be reversed by prolonged elevation. Otherwise, free edema is gradually replaced by fibrotic induration and fat deposits, leading to chronic inflammation and a positive Stemmer’s sign. Manual lymphatic drainage is a first step treatment. Special elastic and non-stretched bandages are applied on the lymphedematous area, including toes and fingers, to prevent expansion of fluid. Sequential compression on the upper or lower affected limb, can also be applied, at a more advanced stage. Lympho-venous bypass and vascularized lymphatic vessels or lymph nodes transplantation, are surgical techniques in use, that can improve considerably the condition at the end stages of the disease. Finally, it has been recently demonstrated, that ketoprofen can improve significantly skin damage in patients with lymphedema, by blocking the inflammatory molecule leukotriene B4 (LTB4).
Key words
Lymphedema; Ketoprofen
 |
 |
 |
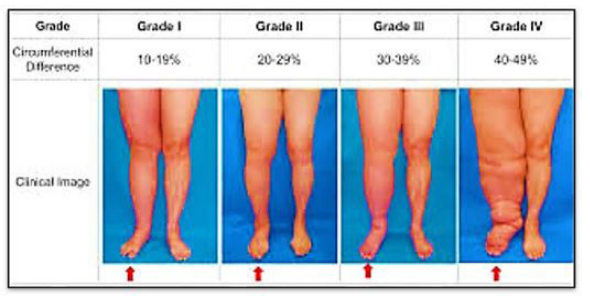
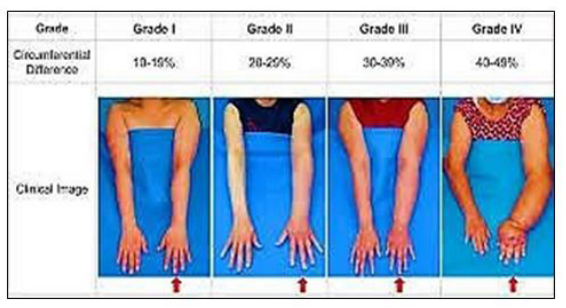
| Figure 1: Lymphedema of the upper or lower extremities |
 |
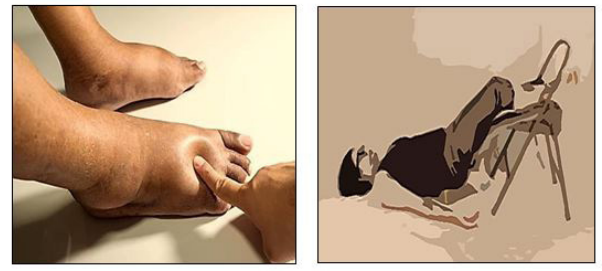
| Figure 2:Long standing deep venous insufficiency can lead to a lymphedema-like entity |
 |
| Figure 3:Assessment techniques for lymphedema |
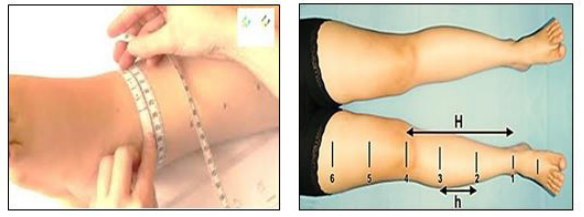 |
| Figure 4: Circumference measurements of the limbs using a tape |
 |
| Figure 5: Postivie Pitting edema (left) and negative stemmer's sign (right) |
 |
| Figure 6: Stemmer’s sign positive |
 |
| Figure 7: Manual lymphatic drainage is a first step treatment: This is a specialized form of very light massage that helps to move fluid from the end of the extremities toward the trunk of the body. Manual lymphatic drainage is different from standard massage and should be performed by a trained professiona |
 |
| Figure 8: Special elastic and non-stretched bandages are applied on the lymphedematous area including toes and fingers to prevent expansion of fluid. This action may be reinforced with the use of full length elastic stockings, applied above the bandages. |
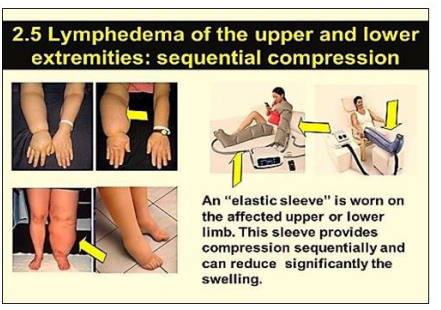 |
| Figure 9: Sequential Compression of the upper and lower lymphedematous limb |
 |
| Figure 10: The lymph-press device, has been used extensively at the old Nicosia General Hospital Vascular Laboratory, in treating lymphedema |
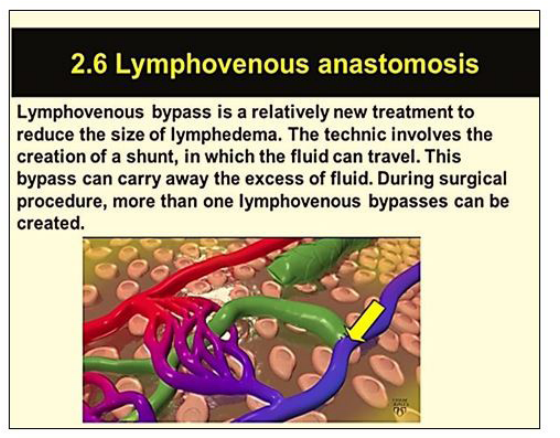 |
| Figure 11: Lymphovenous anastomosis (see the arrow) |
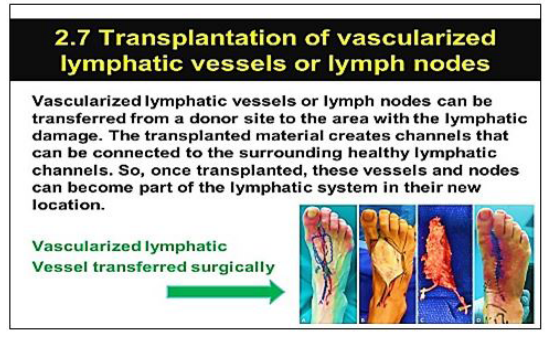 |
| Figure 12: Transplantation of lymphatic vessels and nodes in the lower extremity |
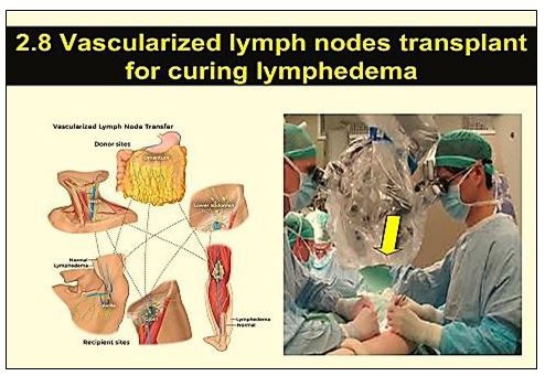 |
| Figure 13: Good results can be obtained anywhere in the body, using either vascularized lymph nodes or lymphatic vessels transplantation |
 |
| Figure 14: Ketoprofen. Could it be the answer for the treatment of lymphedema? |
What is lymphedema?
Lymphedema is a progressive disease of the skin and of the subcutaneous tissues, that occurs when normal lymphatic clearance is disturbed. This disease, is a major contributor to disability and social isolation for the affected people. Anyone can develop this condition, either as a primary lymphedema, which usually is an autosomal dominantly inherited disease (Milroy’s disease), or a familial condition, that develops soon after puberty (Meige disease). Usually, it can be developed as a secondary lymphedema. Major causes for secondary lymphedema include cancer therapy, (surgical removal of lymph nodes and/or irradiation), as well as the parasitic disease fillariasis, damage of the skin caused by exposure to irritant soils (podoconiosis), and repeated episodes of lymphangitis (Figures 1).
Symptoms
A common symptom of fluid retention both in primary and secondary lymphedema, is swelling of the upper or lower extremities according to the etiology of lymphedema. It can be either mild or severe and may result from prolonged standing or sitting, but at the advanced stages, may be permanent and progressive, causing serious disability for the affected people.
In general, edema is defined as a palpable swelling caused by increased interstitial fluid volume. Apart from the primary or secondary lymphedema, common cause of leg edema in older adults is venous superficial or deep insufficiency. The most common cause in women -between menarche and menopause- is the idiopathic edema, formerly known as “cyclic” edema. Finally, a common but under-recognized cause of edema is pulmonary hypertension, which is often associated with sleep apnea [1,2].
Mechanism of lymphedema
When lymph flow is impeded for any reason, an accumulationof protein-rich fluid in the loose connective tissues occurs. This excess fluid is eventually replaced by fibrotic induration and fat deposition. Regardless of the cause, long-term reduction in lymphatic activity will always lead to chronic inflammation, skin pathologies, and an increased risk of bacterial and fungal infections.
In Europe, we see very rarely lymphedema due either to phyllariasis or podokoniosis. What is usually common, is the lymphedema after surgical removal of glands and the post irradiation lymphedema of the area that has developed cancer. Such lymphedema has a progressive character if remains untreated, and its management becomes increasingly difficult and intensive.
At this point, I would like to stress that a lymphedema-like entity common in Europe, results in patients with a long standing deep venous insufficiency, in the sense of incompetent superficial or deep venous valves, leading to accumulation of a concentrated interstitial fluid within the soft tissues of the affected extremities, which cannot be drained adequately into the existing high pressure venous environment (Figure 2). This situation can be considered as a free lymph flow disturbance [3-5].
Assessment techniques for lymphedema, when pitting edema is present
A simple way to characterize the lymphatic swelling as free, is the reversal of the swelling after prolonged limb elevation (Figure 3), because reabsorption of the interstitial fluid into the venous system may eventually occur, due to the existing pressure difference. On the contrary, the swelling that does not reverse by an overnight elevation, indicates that the accumulated fluid is not free any longer, as connective tissue overgrowth has already started as a result of inflammation (Figure 3).
Reversal on limb elevation
This may also occur, when high venous pressure exists, as in case of long standing superficial and/or deep venous incompetence. The high venous pressure, does not allow free lymphatic flow into the venous system. (Figure 3)
Comparison of circumference measurements of the lymphedematous limb to the normal, by using a tape
A tape is used to record circumference measures of both limbs at certain locations (Figure 4). Such circumference measurements are useful to determine the size of unilateral limb enlargement when there is an unaffected contralateral limb [6,7].
Pitting test
Pitting edema occurs when firm pressure is applied by a finger or thumb to the skin perpendicularly, holding it there until the underlying tissue deforms. Such a deep pit with a rounded base, can be formed easily when a protein-rich fluid is present but without significant fibrotic induration. (Figure 3 and 5). On the contrary, when a shallow pit is formed after prolonged pressure, indicates that the fluid load has been largely replaced by the growth of fibrotic tissue and by fatty deposits [8].
Stemmer’s sign (Figure 6) is frequently used for the differential diagnosis of an edema lymphatic in origin (positive Stemmer’s Sign-Figure 6), from an edema of venous origin (negative Stemmer’s Sign-Figure 6).
Grading lymphedema
To grade lymphedema is not an easy task. That is because there are several staging systems and that is why a simple staging into mild, moderate and severe is still preferred. Cheng lymphedema grading system for moderate to severe cases, is presented in Table 1 and Table 2.
Pathophysiology and Management
Under normal conditions, lymph fluid is drained from the tissues by the lymphatic system, filtering the fluid through the lymph nodes. Lymphedema is caused by blockage or damage to the lymph system, and there are several steps that can be taken to manage the symptoms [8].
Manual lymphatic drainage (Figure 7)
Bandages and elastic stockings (Figure 8)
Sequential compression of the upper and lower extremities using special equipment (Figure 9)
Lymphovenous anastomosis (Figure 11)
Lymphatic transplantation (Figure 12)
Vascularized transplantation of lymph nodes and lymphatics anywhere in the body (Figure 13)
A new hope for the treatment of post-operative lymphedema immerged
So far, lymphedema has no cure. Current treatments proved to have palliative effect only. Recently, Dr Rockson of Stanford’s University have shown that ketoprofen can improve significantly skin damage in patients with post- mastectomy lymphedema.
Some years ago, Dr Rockson, Professor of cardiovascular medicine at Stanford's, began to suspect that inflammation was a significant cause of the disease. To test his theory, he created originally a mouse model for lymphedema and then, to test ketoprofen in humans, he conducted a pilot trial with normal volunteers and lymphedema patients, who knew they were getting the drug orally for four months. Skin biopsies were taken at the beginning and at the end of the trial, as a measurement of the severity of the disease. The positive findings of this trial were published in JCI Insight (2019) [9-12].
A 2nd research by Dr Rockson and associates found that ketoprofen worked by blocking the inflammatory molecule leukotriene B4 (LTB4). They also found that the buildup of lymph fluid is actually an inflammatory response within the skin and not a “plumbing” problem within the lymphatic system. They discovered that the naturally occurring inflammatory molecule LTB4 is elevated both in animal models and in humans with lymphedema and that elevated levels can cause tissue inflammation and impaired lymphatic function [13].
Ketoprofen (Fig 14) appears to effectively treat lymphedema and ease the burden of care. Ketoprofen is available in oral form, reaches its peak plasma level in 1/2 to 2 hours and its half-life is 2.4 hours; its analgesic duration is 4 to 6 hours. The recommended dosage is 300 mg/day. The extended-release capsules are usually taken daily for prolonged periods [14,15].
Factors linked with the risk of lymphedema
Factors that are linked with the risk for lymphedema included (a) age, (b) body mass index, (c) kind of infusion chemotherapy, (d) extent of lymph node removal, (e) location of the radiotherapy field, (f) amount of postoperative fluid collection, (g) extend of infection, and (h) extend of early edema (swelling). An initial estimation of the risk for lymphedema can be obtained prior to surgery, and the overall risk can be modified accordingly.
A variety of factors are associated with the occurrence of lymphedema after any cancer treatment
Other researches came to the conclusion that the incidence of lymphedema that results from a cancer treatment is associated (a) to the type of cancer and (b) to the type and extent of the treatment used. Also, (c) it is associated to the length of follow up and (d) to the methods that have been used in assessing the cancer [16-19].
Final thoughts
The aim of this presentation was to present what we have today available in the therapeutic armamentarium to deal with lymphedema. The use of ketoprofen recently as a mean of reduction of the extent and amount of lymphedema looks strange but is simple and effective to some extent. On the basis of my own observations, I have the feeling that the administration of this drug in the long run may be used only whenever there is evidence that new inflammatory reaction in the affected area is occurring and may create new complications.
References
- Smith JW, Conway H (1962) Selection of appropriate surgical procedures in lymphedema. Introduction of the hinged pedicle. Plast Reconstr Surg Transplant Bull 30: 10-31.
- Thompson N (1970) Buried dermal flap operation for chronic lymphedema of the extremities. Ten- year survey of results in 79 cases. Plast Reconstr Surg 45: 541-8.
- Degni M (1974) New technique of lymphatic-venous anastomosis (buried type) for the treatment of lymphedema. VASA 3: 479-83.
- O’Brien BM, Sykes P, Threlfall GN (1977) Micro-lymphaticovenous anastomoses for obstructive lymphedema. Plast Reconstr Surg 60: 197-211.
- Degni M (1978) New technique of lymphatic-venous anastomosis for the treatment of lymphedema. J Cardiovasc Surg (Torino) 19: 577-80.
- Baumeister RG, Siuda S (1990) Treatment of lymphedemas by microsurgical lymphatic grafting: what is proved? Plast Reconstr Surg 85: 64-74.
- Lee M (2015) Mitsumori, Elizabeth S. McDonald, Gregory J. Wilson, et al. Lymphangiography: How I do it. Journal of Magnetic Resonance Imaging 42: 1465.
- Ran Ito, Jonathan Zelken, Chin-Yu Yang (2016) Proposed pathway and mechanism of vascularized lymph node flaps. Gynecologic Oncology 141: 182.
- Maria Antonietta Mazzei, Francesco Gentili, Francesco Giuseppe Mazzei (2017) High- resolution MR lymphangiography for planning lymphatic venous anastomosis treatment: a singlecentre experience. La radiologia medica 122: 918.
- Caroline A, Gjorup Helle W, Hendel Bo Zerahn (2017) Volume and Tissue Composition Changes Measured with DualEnergy X-Ray Absorptiometry in Melanoma-Related Limb Lymphedema. Lymphatic Research and Biol 15: 274.
- Pavel N (2018) Myshencev, Sergey E. Katorkin, Leonid A. Lichman. A case of successful surgical treatment of a patient with lymphedema of lower limbs. I P Pavlov Russian Medical Biological Herald 26: 288.
- Wang Jing, Mitsunaga Narushima (2018) Half-transection method combined with intravascular stent for supermicrosurgical lymphatico-venular anastomosis. J Plastic Reconstructive & Aesthetic Surgery 71: 1816.
- Daniel J Gould, Babak J Mehrara, Peter Neligan (2018) Lymph node transplantation for the treatment of lymphedema. J Surgical Oncol 118: 736.
- Hisako Hara, Makoto Mihara. Multi-area lymphatic venous anastomosis with multi- lymphosome injection in indocyanine green lymphography: A prospective study. Microsurgery 39: 167.
- Pavel N. Myshencev, Sergey E. Katorkin, Leonid A Lichman (2018) A case of successful surgical treatment of a patient with lymphedema of lower limbs. I P Pavlov Russian Medical Biological Herald 26: 288.
- Bonina F, Santagati NA, Puglia C (2003) Ketoprofen 1‐ alkylazacycloalkan‐2‐one esters as dermal prodrugs: in vivo and in vitro evaluations. Drug Dev Ind Pharm 29: 181-90.
- Pontiki E, Hadjipavlou‐Litina D (2005) Lipoxygenases superfamily (LOX): an interesting target for the development of inhibitors‐promising drugs against cell differentiation, inflammation and carcinogenesis. Curr Enz Inh 1: 309-28.
- G Pons, JA Clavero, X Alomar (2019) Preoperative planning of lymphatic venous anastomosis: The use of magnetic resonance lymphangiography as a complement to indocyanine green lymphography. Journal of Plastic Reconstructive & Aesthetic Surgery 72: 884.
- Zinka Rajic, Dimitra Litina, E Pontiki (2010) The Novel Ketoprofen Amides – Synthesis and Biological Evaluation as Antioxidants, Lipoxygenase Inhibitors and Cytostatic Agents. Chemical Biol and drug Design 75: 641-52.
Artcle Information
Review Article
Received Date: November 28, 2021
Accepted Date: December 28, 2021
Published Date: December 30, 2021
Journal of Pathology and Medicine
Volume 1 | Issue 1
Citation
N Angelides (2021) Lymphedema: Old and New Ideas Concerning Treatment. J Pathol Med 1(1):101
Copyright
©2021 N Angelides. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jpm.2022.1.101