

Review Article
Volume-1 Issue-1, 2021
Molecular Insight into Key Targets and Inhibitors for Breast Cancer Treatment
Received Date: September 12, 2022
Accepted Date: October 12, 2022
Published Date: October 15, 2022
Journal Information
Abstract
Breast cancer accounts for the highest morbidity and mortality incidence among women globally. Despite advancements in technology, the mortality and mobility incidence of cancer patients have not yet declined. Several targets and inhibitors were discovered for the treatment of luminal, HER2 positive and triple-negative breast cancer. However, satisfactory treatment remains a challenge yet due to drug resistance and heterogeneity of these cancers. In this review, we describe the pathology, potential targets, and inhibitors developed to treat breast cancer. In addition, we briefly discuss the important scaffolds used in drug design for the development of inhibitors against potential targets of cancer. There is an evolving paradigm shift in oncology that focuses on molecularly targeted strategies for cancer treatment. For this, the current review highlights important drug targets to prevent cancer growth.
Abbreviations: DNA: deoxyribonucleic acid ; HER2: human epidermal growth factor receptor 2; MAPK: mitogen-activated protein kinase; PI3K: phosphatidylinositol 3-kinase; EGFR: epidermal growth factor receptor; TNBC: triple-negative breast cancer; IBC: inflammatory breast cancers; CSCs: cancer stem cells; HIF: Hypoxia-inducible factor; HR: hormone receptor; HR+: hormone receptor positive; HER2−: human epidermal growth factor receptor 2 negaitive; ER: estrogen receptor ; PR: progesterone receptor; ET: Endocrine therapy; TKI: tyrosine kinase inhibitor; ATP: adenosine triphosphate.
Key words
Luminal breast cancer; HER2 positive; triple negative; targets; inhibitors
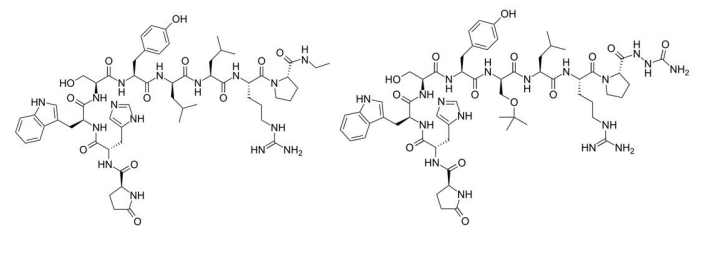  |
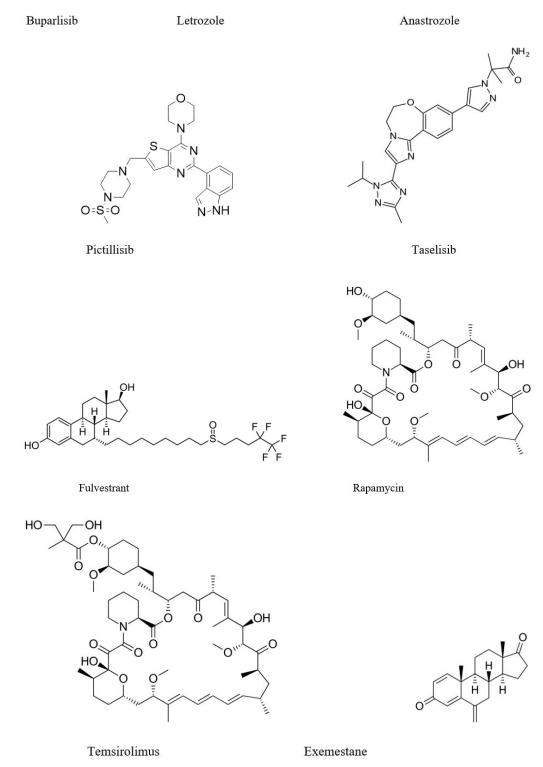
| Figure 1: Some potent drugs used in the treatment of luminal breast cancer |
 |
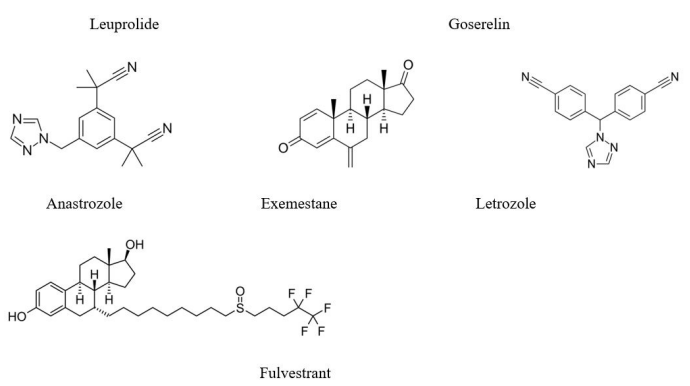
| Figure 2:Some potent and selective CDK4/6 inhibitors |
  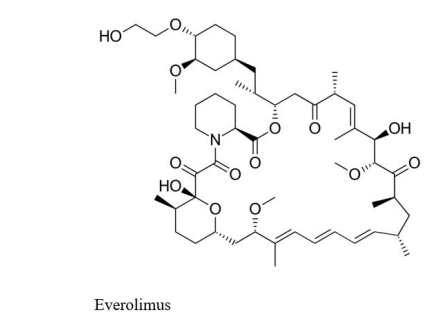 |
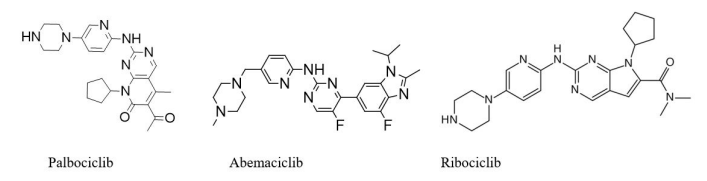
| Figure 3:Some potent PI3K–Akt–mTOR inhibitors |
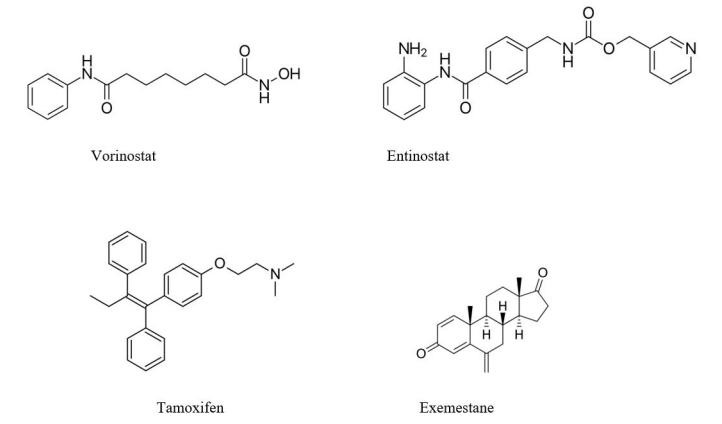 |
| Figure 4: Some potent histone deacetylase inhibitors used in combination therapy |
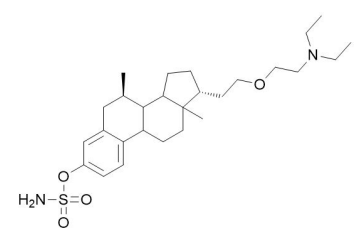 |
| Figure 5: SR16157 one of the potent steroid sulfatase inhibitor |
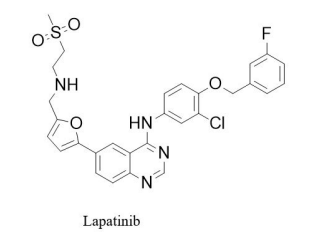 |
| Figure 6: Lapatinib one of the potent HER2 inhibitor |
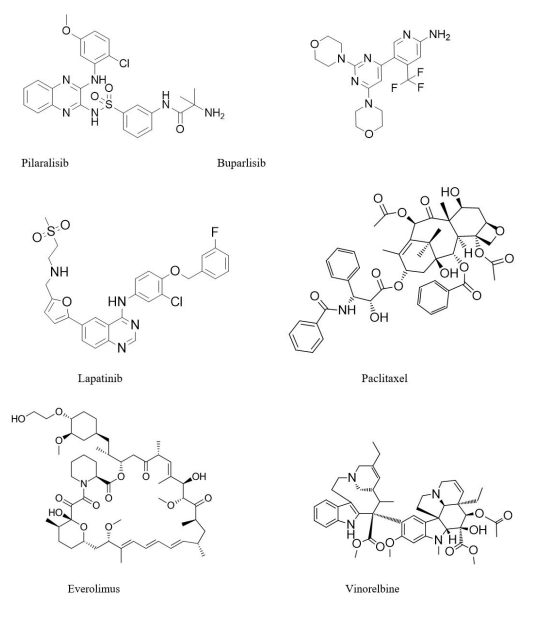 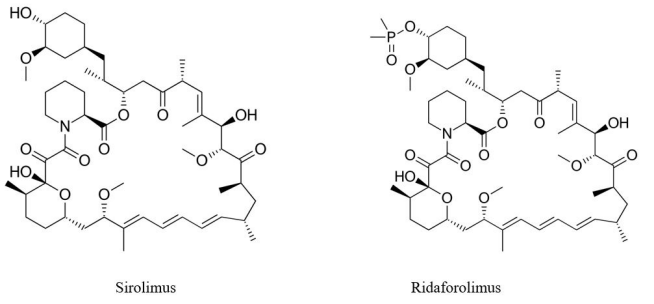 |
| Figure 7: Some potent and novel PI3K/Akt/mmTOR inhibitors used in combination therapy for HER2+ breast cancer |
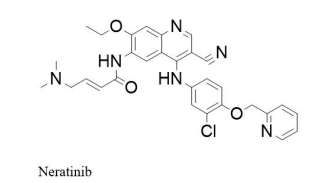 |
| Figure 8: Neratinib is one of the novel and potent HER2 inhibitor |
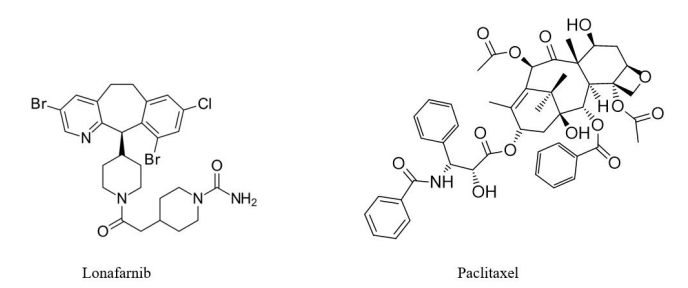 |
| Figure 9: Structure of farnesyl transferase inhibitor lonafarnib showed enhanced potency in combination with paclitaxel and trastuzumab during phase-I clinical trial |
 |
| Figure 10: Some potent PARP inhibitors |
 |
| Figure 11: Some potent anti-angiogenic agents used in combination therapy |
 |
| Figure 12: Some potent EGFR inhibitors that showed significant activity in combination with cetuximab |
 |
| Figure 13: Dasatinib is one of the potent SRC inhibitor |
Introduction
Cancer research has been the topic of concern discussion among scientists from several decades. It involves an array of dynamic changes in the genome that arise through mutations that transform normal tissues into malignant tumours [1]. Cancer is the second most death-causing disease among human beings affecting globally after cardiovascular diseases. Approximately 10 million deaths and 19.3 million new cases of cancer were reported in 2020 globally. Female breast cancer was reported as one of the most commonly diagnosed cancer and recording of 2.3 million new cases, followed by lung cancer. The overall global burden due to cancer is expected to be 28.4 million cases in 2040 [2]. Around 1,918,030 new cancer cases and 609,360 cancer deaths are expected to occur in United States in the year 2022. It is estimated that approximately 350 deaths could take place per day due to lung cancer in 2022 in United States alone [3]. Risk factors associated with the distribution of population growth, ageing, and socio-economic development reflects elevated cancer incidence and mortality rate globally among human beings. Environmental factors and lifestyle have adverse side-effects in the causation of cancer development and progression [45].
As the breast cancer accounts for the highest morbidity and mortality incidence among women globally [6], there are numerous associated risk factors which increase the probability of breast cancer, such as ageing, estrogen, family history, alcohol, sex, obesity, hormone replacement therapy during menopause, higher levels of estrogens, early age at first menstruation, and old age gene mutations, ionizing radiation, unhealthy lifestyle, endocrine factors, early age at first menstruation, old age and prolonged tobacco smoking [7]. Apart from these risk factors, many genetic factors are liable for causing breast cancer. Mutations and abnormal amplification in oncogenes and antioncogenes play vital roles in tumor initiation and progression [8]. BRCA1 and BRCA2 are anti-oncogenes located on chromosome 17q21 and 13q12, respectively [9]. They are responsible for 5-10% breast cancers among 20-25% of hereditary breast cancers [10]. Both these genes participate in DNA repair and transcriptional regulation during DNA damage. Therefore, deficiencies of BRCA1 or BRCA2 functions ultimately result in increased genetic alterations and the development of cancer [11].
In addition, Human epidermal growth factor receptor 2 (HER2) oncogenes located on chromosome 17q12 plays a significant role in cell proliferation and division that is observed in breast cells12. HER2 is mediated by crucial signalling pathways such as the mitogen-activated protein kinase (MAPK) pathway and phosphatidylinositol 3-kinase (PI3K) pathway. HER2 gene amplification and protein overexpression ultimately lead to malignant transformation by PTEN/Akt/mTORC1 signalling [13,14]. Further, epidermal growth factor receptor (EGFR) is also located on chromosome 7p12 and stimulates cell proliferation, invasion, angiogenesis and protects against apoptosis by crucial signalling pathways, which include Ras-Raf-MAPK, PI3K, and JNK [15,16]. Overexpression of EGFR leads to approximately half cases of inflammatory breast cancers (IBC) and triplenegative breast cancers (TNBC) [17].
c-Myc is located on chromosome 8q24 and plays a crucial role in tumor initiation and progression. c-Myc over-expression is generally seen in the high-grade, invasive breast cancer stage [18]. Over-expression of H-ras gene is identified in primary and advanced breast cancer and signifies poor prognosis [19]. Modifications or mutations in the gene p53, a tumor suppressor gene localized on chromosome 17p13.1, eventually initiate deleterious effects in many cell based events such as cell-cycle arrest, DNA damage repair, and chromatin re-modeling, and apoptosis [20].
Pathogenesis
Breast cancer is usually adenocarcinoma that develops from hyper-proliferation in the cell lining of milk duct, which then proliferates into benign or metastatic tumors after repetitive stimulation by numerous carcinogenic factors. Tumor microenvironments that include macrophages and stromal influences have a crucial role in aiding breast cancer initiation and progression. Animal model studies have showed that repetitive exposure of carcinogens to stroma results in metastatic growth of mammary glands in mice [21]. Infiltration of macrophages creates a mutagenic inflammatory microenvironment and stimulates angiogenesis. Macrophages also suppress the immunity and play significant role in the promotion of cell migration and invasion [22]. Different DNA methylation patterns have been observed between the normal and tumor-associated microenvironments, suggesting that the tumor microenvironment produced through epigenetic modifications can aid in promoting carcinogenesis [23]. It has been observed variation patterns in DNA methylation at CpG sites in specific and invasive cancers, indicating epigenetic changes ultimately lead to carcinogenesis [24].
Recently, cancer stem cells (CSCs) were discovered that arise from stem cells or progenitor cells in normal or healthy tissues and are associated with tumor initiation, progression, escape, and recurrence. Moreover, they can undergo self-renewal, show pluripotency, and resistance to conventional modes of treatments such as chemo- and radiotherapy [25,26]. Breast cancer stem cells (bCSCs) are currently treated as one of the significant targets in breast cancer treatment. Many development pathways such as Wnt/β-catenin Notch, Shh (sonic hedgehog), BMP/TGF-β (bone morphogenetic proteins/transforming growth factor β), PI3K, p53, and HIF (Hypoxia-inducible factor) are involved in selfrenewal, proliferation differentiation, and invasion processes of bCSCs [27].
Classification and treatment regimens
Breast cancer can be broadly classified into four significant subtypes, which include luminal A, luminal B, HER2 positive, and triple-negative. Luminal breast cancer is primarily positive for hormone receptor (HR), which can be either estrogen receptor (ER) or progesterone receptor (PR). Luminal subgroup A (HR+/ HER2−) is comparatively slow-growing and less aggressive than luminal subgroup B (HR+/HER2+) with low prognosis rate and marked by high expression of Ki67 (a proliferation marker) or HER2 [28]. Luminal A is the most common type of breast cancer that can be ER+ and/or PR+/HER2 in nature.
Luminal B accounts for approximately 10% of all breast cancers and is characterized by ER+ and/or PR+/HER2+ status. Breast cancer subtype having negative ER, PR, and HER2 status are termed as “triple negative” breast cancers that is prevalent in pre-menopausal, younger and overweight female population. The HER2 positive breast cancer characterized with HER2+/ ER−/PR− status is less common but having treated as highgrade tumor with poor clinical outcomes [29]. Heterogeneity of breast cancer is the most challenging aspect for determining the therapeutics options [30]. Targeted therapies or molecular targeted therapy is a type of cancer treatment that interferes with specific targeted molecules involved in cancer cell growth and survival [31]. Many promising anticancer drug targets have been reviewed, including kinases, monoclonal antibodies, cancer stem cells, vascular targeting agents, and tubulin. Treatment options which are currently employed for different subtypes of breast cancers are described in this review.
Luminal breast cancer (HR+)
Luminal breast cancer comprises 60% of the total breast cancer incidences in the developed countries and the population rate appears to be increasing in premenopausal women [32]. Endocrine therapy (ET) acts as the mainstay for treating HR+ breast cancer patients in adjuvant and metastatic circumstances. Currently, several drugs are available in the market that are based on blocking the estrogen uptake like tamoxifen, or depleting estrogen level via oophorectomy, luteinizing hormone-releasing hormone analogs such as leuprolide and goserelin or aromatase inhibitors like anastrozole, exemestane and letrozole. [33] Other options include targeting the estrogen receptor by making use of selective estrogen receptor down-regulators like fulvestrant or through selective estrogen receptor modulators (Figure 1). Sequential administration of endocrine treatment is preferentially recommended until there is a necessity for rapid response or evidence of clinical resistance, while chemotherapy will be indicated [34]. Metastatic luminal breast cancer may sometimes develop resistance to these hormonal therapies, facilitated by either genomic modifications in the estrogen receptor or by upregulation of other signaling pathways. Thus, several strategies are used to develop novel agents aimed at reversing resistance to standard hormonal therapies [33].
CDK4/6 inhibitors
Cyclin-dependent kinases 4 and 6 (CDK4/6) are serine/threonine kinases consisting of a 300-aminoacid catalytic domain, which are usually inactive [35]. During S phase of DNA synthesis of cell progression, all the cells need cyclin subunit to activate the catalytic domain of CDKs. The D-type cyclin (cyclin D1, cyclin D2, and cyclin D3) work in association with CDK4/6, which mediates cells to progress through the G1 phase of the cell cycle. Activation of several upstream mitogenic pathways including PI3K-AKTmTOR, estradiol, and RAS-RAF-MEK-ERK enhances the cyclin D-dependent CDK4/6 activity [36]. CDK4/6 inhibitors work by blocking the downstream phosphorylation of retinoblastoma (Rb) by binding to the ATP–binding pocket of protein kinase. Thus, resulting in down-regulation of E2F-response genes which mediate G1-S arrest [37]. Moreover, these inhibitors are responsible for dephosphorylating the transcription factor FOXM1 (Forkhead box protein M1), thus inhibiting cell proliferation [37]. Palbociclib, abemaciclib, and ribociclib are orally bioavailable and highly selective inhibitors of CDK4/6 [38] (Figure 2).
PI3K–Akt–mTOR pathway inhibitors
PI3K–Akt–mTOR (PAM) is a significant signalling pathway involved in cell proliferation, metabolism, survival, and motility [39]. Abnormal activation in the signalling pathway results in hormonal resistance [40]. This pathway has been observed to be activated in approximately 70% breast cancer, having PIK3CA and PTEN3 most frequently mutated or amplified oncogenes and tumor suppressor genes respectively [41, 42]. Combination therapies have been introduced to target both HR and PI3K/Akt/ mTOR pathways for effectively reversing hormonal resistance43. Different strategies used earlier for targeting the PAM signalling pathway revolve around the inhibition of upstream targets, including PI3K and Akt. Although dual inhibitors were developed for inhibiting both mTOR and PI3K, but these showed increased toxicity [43]. Buparlisib (a pan-class I PI3K inhibitor) has shown a significant effect in progression-free survival (PFS), especially in those that involve PIK3CA mutation [44].
The PI3K pathway involves a series of a complex system of interactions with various parallel cascades. Therefore, hindrance in its path indirectly leads to negative feedback whose consequence may result in the activation of additional compensatory signalling pathways including PTEN loss [45,46]. Since breast cancers have heterogeneous genomic architecture [47], they have multiple drivers in different pathways for causing the disease, such as, in some cells, PI3K-AKT has been observed for not being a dominant regulator of Mtor [48]. To overcome this problem, combinational therapies are being used both in the pre-clinical and clinical trials [49]. For example, for HR+/ HER2− early breast cancer patients, neoadjuvant treatment is used in combination with letrozole or anastrozole [50]. However administration of both pictilisib and taselisib were found to improve antitumor effects regardless of PIK3CA status [51]. Among several modifications with potential clinical significance, PIK3CA inhibitors used in combination with fulvestrant showed promising results at the expense of increased toxicity [51]. Recently, with the help of preclinical data it was found that PI3K inhibition may act synergistically with CDK 4/6 inhibition to overcome intrinsic and adaptive resistance mechanisms and reduce cell viability [52].
Rapamycin (sirolimus) exists as the first mTOR inhibitor and was employed as an immunosuppressant in transplant recipients [53]. Temsirolimus was subsequently developed and is approved for the treatment of renal cell carcinoma49. Everolimus is an oral mTOR inhibitor approved for HR-positive breast cancer in combination with exemestane after treatment failure with letrozole or anastrozole [54]. These agents are considered as “rapalogues” and work as allosteric inhibitors of mTORC1 [49] (Figure 3).
HDAC inhibitors
In ER+ patients, histone deacetylation-mediated loss of ER expression results in hormonal resistance, which may be reversed by histone deacetylase (HDAC) inhibitors. These inhibitors upregulated the expression of ERα and aromatase and inhibit growth factor signalling pathways [55]. Both vorinostat and entinostat are used as second-line treatment for HR-positive breast cancer, and these show significant anticancer activity in combination with tamoxifen and exemestane respectively as compared to tamoxifen/exemestane monotherapy56 (Figure 4).
Steroid sulfatase inhibitors
Steroid sulfatase is a key enzyme responsible for converting the inactive sulfate-conjugated steroids forms to the most active and estrogenic non-conjugated formats [57]. The expression level and the enzyme activity of steroid sulfatase were upregulated abnormally in ERα+ breast cancer [58]. Thus, the rationale for inhibiting steroid sulfate is essential for reducing estrogenic steroids that help in stimulating breast cancer growth and progression56. A novel steroid sulfatase inhibitor SR16157 has been evaluated for hormone-dependent breast cancer to inhibit steroid sulfatase and release specific ERα modulators59 (Figure 5).
HER2 positive breast cancer
The insight study of tumor biology and HER2 signalling has led to the innovation of novel HER2-molecular targeted agents that along with anti-HER2 therapy beyond progression, leads to unpreceded survival outcomes in advanced HER2 positive breast cancer patients [60]. The agents used for HER2 positive breast cancer are administered alone or in combination with standard chemotherapy. Trastuzumab is a humanized monoclonal antibody whose mechanism of action against the HER2 receptor has become a landmark for treating HER2 positive breast cancer patients61. Pertuzumab is a humanized monoclonal antibody binds to the extracellular domain II receptor, contradicting the trastuzumab binding site. It targets and blocks heterodimers HER2 and HER3 stimulating various intracellular signalling pathways responsible for cell proliferation and survival. The combination of pertuzumab with taxane and trastuzumab works more effectively than taxane and trastuzumab monotherapy with significant clinical benefits as first-line treatment in HER2 positive breast cancer [61, 62].
Further, ado-trastuzumab emtansine is an antibody-drug conjugate with HER2 targeted anti-tumour properties and here the trastuzumab is incorporated with a maytansine derivate (DM1), which is a potent anti-mitotic agent and binds to microtubules for action [63]. Such type of agents allow the specific drug delivery movement intra-cellularly, targeting HER2-overexpressed cells, thus improving the therapeutic index efficiently and reducing normal tissue exposure [64]. Lapatinib, an oral tyrosine kinase inhibitor (TKI) that reversibly inhibits both HER2 and epidermal growth factor receptor (EGFR) is one of the recently developed molecules for breast cancer [56] (Figure 6). Currently, neoadjuvant treatment with a combination of anti-HER2 targeted therapy and chemotherapy is employed as a standard regimen for treating early-stage HER2 positive breast cancer. In continuation of this, specific therapies are proceeded, such as surgery, radiotherapy, and additional HER2-targeted treatment65.
Although significant progress in the treatment of HER positive breast cancer resulted in an increased survival rate of patients, fewer patients are at substantial risk of reoccurrence of the disease. In concern of this, novel agents are being developed and evaluated rapidly [66].
PI3K/Akt/m TOR inhibitors
To overcome the problem of trastuzumab resistance, which occurs due to abnormal activation of the pathway, a combination therapy of trastuzumab with PI3K/Akt/mTOR inhibitors is being reviewed [56]. For instance, combination of Pan-class I PI3K inhibitors pilaralisib and buparlisib, with trastuzumab [67] and the combination of lapatinib, or paclitaxel with trastuzumab antibody showed promising efficacy and safety in pretreated HER2 positive advanced breast cancer patients [68]. Akt inhibitors such as MK-2206 exhibit significant antitumor activities when employed in combination with trastuzumab or paclitaxel and trastuzumab in pretreated HER2 positive advanced breast cancer patients [69, 70]. Combining mTOR inhibitor everolimus with vinorelbine and trastuzumab did not significantly improve clinical outcomes in pretreated HER2 positive advanced breast cancer patients. Yet, these combinations revealed better anticancer activity than using trastuzumab alone in HER positive patients who are HR negative as well [71]. Contrary to this, the combination of two novel mTOR inhibitors sirolimus and ridaforolimus with trastuzumab have shown promising anti-cancerous activity in refractory HER2 positive breast cancer [72,73] (Figure 7).
Multi-Targeting tyrosine kinase inhibitors (TKIs)
Neratinib (HKI-272) is one of the novel irreversible TKI of HER1/ HER2/HER4, which binds to intracellular kinase domain and forms a covalent complex. Moreover, treatment with neratinib after trastuzumab-based adjuvant therapy had shown significant efficacy in HER2 positive breast cancer [74] (Figure 8).
Monoclonal Antibodies
Patritumab is an anti-HER3 monoclonal antibody, and preclinical data have shown promising antitumor activity by hindering the production of HER2/HER3 heterodimers. Moreover, it exhibited auspicious efficiency and satisfactory tolerability in HER2 positive advanced breast cancer patients [75].
Antibody-Drug Conjugate (ADC)
Trastuzumab emtansine (T-DM1) is an ADC that integrates the HER2 targeting the antitumor activity of trastuzumab with the cytotoxicity of a microtubule-inhibitory candidate, emtansine. It is approved for being the second-line treatment avenues in trastuzumab/ lapatinib-relapsed/refractory HER2 positive breast cancer patient [76, 77].
Farnesyl Transferase Inhibitors (FTI)
Lonafarnib, as a specific FTI, inhibits Ras function by farnesylation. Although RAS mutations are not expected (< 2%) in BC, Ras protein and its downstream effectors are often activated due to overexpression of upstream signalling molecules (e.g., HER2) [78]. Recently, a phase I trial showed that addition of lonafarnib to trastuzumab and paclitaxel therapy exhibited superior antitumor activities in HER2 positive breast cancer [79] (Figure 9).
Triple negative breast cancer
Triple-negative breast cancer (TNBC), a subtype of breast cancer that is defined by the absence in the expression of estrogen and progesterone receptors (ER/PR) and HER2 receptors and accounts for about 10–15% of all diagnosed breast cancers [80]. It is well-characterized for having a unique molecular profile, biologically aggressive behavior, inferior prognosis, diverse metastasis patterns, association with BRCA1 mutation status, and deficient targeted therapies [81]. Deficiency in the expression of ER, PR, and HER2 in advanced TNBC excludes the use of targeted therapies. Thus adjuvant chemotherapy is the widely accepted systemic treatment option that commonly includes anthracyclines, taxanes, and platinum drugs with or without bevacizumab which is a recombinant humanized monoclonal antibody that works against vascular endothelial growth factor (VEGF) [82]. As compared to other breast cancer subtypes, TNBC has limited therapeutic options due to the absence of well-defined molecular targets. Therefore, there is an urgent requirement for identifying novel therapeutic targets and the development of preventive methods. Following are novel therapies that are being used for the treatment of TNBC.
PARP inhibitors
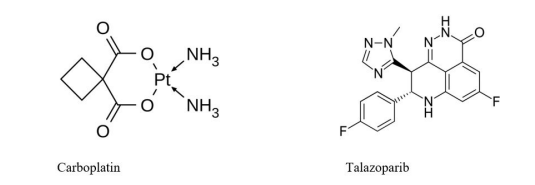
Poly (ADP-ribose) polymerases (PARPs) are the enzymes found to be involved in several aspects of cellular response to various forms of damage. The most abundant PARP-1 and PARP-2 play a central role in DNA damage repair, and treated as one of the important therapeutic targets for cancer treatment. It is presumed that inhibition of PARP activity sensitizes the cancerous cells to chemotherapy and radiation leading to effective outcome [83]. Development in understanding the TNBC heterogeneity is due to the disclosure of a subgroup of sporadic TNBC, which essentially shares the homologous repair deficiency characteristic with BRCA1/2-mutated breast cancer [84]. Therefore, combinational drug therapies are being proposed by integrating the DNAtargeting platinum drug carboplatin or PARP inhibitors to standard chemotherapy [85]. The PARP enzyme helps repair the DNA single-strand breaks while the BRCA1/BRCA2 genes, encoding tumor-suppressor proteins, are involved in the repair of DNA double-strand breaks via homologous recombination. Promising clinical activities have been seen by using PARP inhibitors in patients with germ line BRCA1/BRCA2 mutation (gBRCA+), probably by synthetic lethality that arise from unresolved DNA damage and also by replication arrest triggered by physical hindrance of DNA replication forks [86]. Talazoparib is currently under phase III trial (NCT01945775) and has shown utmost preclinical efficacy due to strong binding with DNA utilizing trapping PARP–DNA complexes [86]. It has proved to have promising antineoplastic activities in advanced gBRCA+ BC as a single agent [87] (Figure 10).
Anti-angiogenic agents
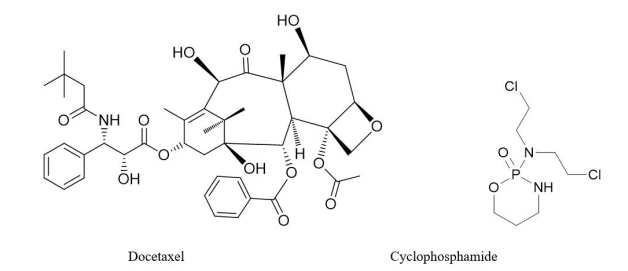
The intra-tumoral expression of angiogenic factors such as VEGF is well-known for being abnormally higher in TNBC in contrast to non-TNBC breast cancers [88]. Bevacizumab is an anti-VEGF monoclonal antibody that helps in suppressing the tumor neovasculature growth and also inhibits metastasis. Combining bevacizumab with docetaxel did not significantly affect the overall safety profile of the treatment avenues [88]. It has been also reported that combination of docetaxel and cyclophosphamide with bevacizumab provides excellent results for triple negative breast cancer patients [89] (Figure 11).
EGFR inhibitors
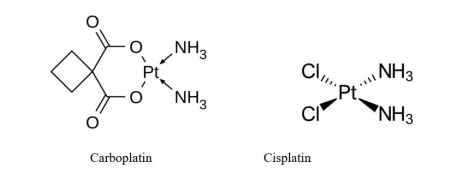
Epidermal growth factor receptor (EGFR) is highly overexpressed in TNBC, which may provide an itinerary as a potential target for EGFR targeting treatment [90]. Phase II studies have evaluated the efficiency of an anti-EGFR monoclonal antibody cetuximab in combination with carboplatin in the metastatic TNBC. This study indicated that combination cetuximab of carboplatin produced response in less than 20% of patients having metastatic TNBC [91]. Combination of cetuximab with cisplatin showed significant response rate with an increase in progression-free survival in metastatic TNBC patients as compared to cisplatin monotherapy [92] (Figure 12).
SRC inhibitors
SRC, a non-receptor signalling kinase involved in the downstream of several growth factor receptors such as EGFR, PDGFR, IGF-1R, and HGFR that get deregulated in TNBC. Dasatinib, an inhibitor of multiple tyrosine kinases such as SRC, has shown unsatisfactory results in TNBC patients during phase II trial (CA180059) [93]. However, in-vitro analysis of dasatinib combined with cetuximab and cisplatin showed synergistic anticancer activity in TNBC cell lines. This threedrug combination produced noticeable apoptosis induction and inhibiting MAPK and EGFR phosphorylation than by employing either a single or two-drug variety. Moreover, it was observed that cancer cell migration and invasion were significantly inhibited by only dasatinib treatment or dasatinib enclosing combination treatment in TNBC cell lines [94] (Figure 13).
Monoclonal antibodies
Glembatumumab Vedotin is monoclonal antibody cytotoxic drug-conjugate designed to target glycoprotein-NMBoverexpressing (GPNMB) in TNBC patients95. The GPNMB is mainly associated with tumor invasion and metastasis, and also, it is overexpressed in around 40% of TNBC. GPNMB is one of the immune modulator and and plays significant role in tumor progression and metastasis in numerous solid cancers [96].
Immunotherapies
Pembrolizumab is a human monoclonal IgG4-ĸ antibody that works against the programmed cell death 1 receptor (PD-1). It has been demonstrated with clinical efficiency and safety in advanced TNBC patients. PD-1 inhibits the immune system from killing cancer cells by preventing autoimmunity by destroying T cells. Although PD-L1 (a ligand of PD-1)-positive advanced TNBC patients were screened for the examination in a phase Ib study, the anticancer activity of pembrolizumab seems to be independent of PD-L1 expression as per another ongoing phase II study [97]. Importantly, pembrolizumab has shown durable antitumor activity with heavily pretreated metastatic TNBC patients [98].
Chemical scaffolds used in breast cancer drug discovery
Most of the approved drugs contain one or more heterocyclic components in them. Some of the essential heterocyclic motifs widely used in drug development include isoxazole, quinolines, isoquinoline, pyrolle, furan, pyridine, indole, pyrazole, oxazole, imidazole, 1,3,4-oxadiazole, 1,3,4-thiadiazole, triazole, etc [99] (Figure 14). Heterocycles that are naturally derived play a crucial role in the biochemical reactions existing in cell metabolism. Their reactivity of these molecules with cells and tissues makes them regulated in a strongly controlled manner, and as a result, any disturbance might be linked with pathological conditions. Thus, the synthetic cyclic compounds employed as anticancer drugs imitate natural ligands and substrates to disturb the obscure balance in cells [100].
Heterocyclic compounds are the privileged scaffolds that have emerged as a promising agent for designing and developing drugs [101, 102]. They can serve as useful tools to alter the polarity, lipophilicity, and hydrogen-bonding capacity of molecules, resulting in improved pharmacological, physicochemical, pharmacokinetic, and toxicological properties of drug candidates103. In addition, heterocyclic natural products and their derivatives have been well recognized for many years as a source of promising therapeutic agents and structural diversity104. Some of the natural products that possess heterocyclic moiety like antibiotics, namely penicillin, cephalosporin, vinblastine, morphine, reserpine, etc [105]. Heterocycles are widely used by medicinal chemists in drug design for cancer treatment [106, 107]. Some available heterocyclic anticancer drugs in the market are methotrexate, doxorubicin, daunorubicin, etc. Majority of the drugs approved for various cancers and other diseases contain one or more heterocyclic moieties in them [108, 109].
Conclusion
Several resources have been utilized for developing a preventive, diagnostic, and therapeutic approach for breast cancer treatment. However, recurrence and resistance of malignant cells are the demerits associated with current treatment regimens. Substantial anticancer drug candidates suffer from lack of selectivity and participate in drug resistance thereby limiting the efficacy of these drugs. Therefore, novel therapeutic strategies are being developed to overcome these complications, which may discover novel anticancer drugs with low toxicity and tackle resistance challenges. There is the immense need for uncovering the alternative molecular targets that are expressed while genesis of breast cancers. The novel drug candidates are required at urgent to tackle the resistance and target specificity issues in breast cancer treatment. Molecular hybridization approach seems an important platform for the design and development of novel drug prototypes with improved pharmacokinetics and pharmacodynamics activity
Acknowledgment
Khan, N.S acknowledges the Indian Council of Medical Research for providing financial support in the form of a Senior Research fellowship (45/9/2019-PHA/BMS).
Conflict of Interest
Authors declare no conflict of interest.
References
- Hanahan D, Weinberg RA (2000) The Hallmarks of Cancer. Cell 100: 57-70. https://doi.org/10.1016/S0092-8674(00)81683-9.
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. (2020) Cancer Statistics: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J Clin. 71: 209-249. https://doi.org/10.3322/caac.21660.
- Siegel RL, Miller KD, Fuchs HE, Jemal A (2022) Cancer Statistics. CA. Cancer J Clin 72: 7-33. https://doi.org/10.3322/ caac.21708.
- Wu S, Powers S, Zhu W, Hannun YA (2016) Substantial Contribution of Extrinsic Risk Factors to Cancer Development. Nature 529: 43–47. https://doi.org/10.1038/nature16166.
- Irigaray P, Newby JA, Clapp R, Hardell L, Howard V, et al. (2007) Lifestyle-Related Factors and Environmental Agents Causing Cancer: An Overview. Biomed. Pharmacother 61: 640- 658. https://doi.org/10.1016/j.biopha.2007.10.006.
- Coughlin SS (2019) Epidemiology of Breast Cancer in Women 9-29. https://doi.org/10.1007/978-3-030-20301-6_2.
- Majeed W, Aslam B, Javed I, Khaliq T, Muhammad F, et al. (2014) A. Breast Cancer: Major Risk Factors and Recent Developments in Treatment. Asian Pacific J. Cancer Prev 2014, 15: 3353-3358. https://doi.org/10.7314/APJCP.2014.15.8.3353.
- Sun YS, Zhao Z, Yang ZN, Xu F, Lu HJ (2017) Risk Factors and Preventions of Breast Cancer. Int J Biol Sci 13: 1387-1397. https://doi.org/10.7150/ijbs.21635.
- Rebbeck TR, Mitra N, Wan F, Sinilnikova OM, Healey S, et al. (2015) Association of Type and Location of BRCA1 and BRCA2 Mutations With Risk of Breast and Ovarian Cancer. JAMA 313: 1347. https://doi.org/10.1001/jama.2014.5985.
- Cardoso F, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, et al. (2019) Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol 30: 1194-1220. https://doi.org/10.1093/annonc/mdz173.
- PaulA (2014) The BreastCancer Susceptibility Genes (BRCA) in Breast and Ovarian Cancers. Front. Biosci. 19: 605. https://doi. org/10.2741/4230.
- Iqbal N (2014) Human Epidermal Growth Factor Receptor 2 (HER2) inCancers: OverexpressionandTherapeuticImplications. Mol Biol Int 1-9. https://doi.org/10.1155/2014/852748.
- Davis NM, Sokolosky M, Stadelman K, Abrams SL, Libra M, et al. (2014) Deregulation of the EGFR/PI3K/PTEN/Akt/ MTORC1 Pathway in Breast Cancer: PossibilitiesforTherapeutic Intervention. Oncotarget 5: 4603-4650. https://doi.org/10.18632/ oncotarget.2209.
- Neve RM, Lane HA, Hynes NE (2001) The Role of Overexpressed HER2 in Transformation. Ann Oncol 12: S9- S13. https://doi.org/10.1093/annonc/12.suppl_1.S9.
- Appert-Collin A, Hubert P, Crémel G, Bennasroune A (2015) Role of ErbB Receptors in Cancer Cell Migration and Invasion. Front Pharmacol 6. https://doi.org/10.3389/fphar.2015.00283.
- Ali R, Wendt MK (2017) The Paradoxical Functions of EGFR during Breast Cancer Progression. Signal Transduct. Target. Ther 2: 16042. https://doi.org/10.1038/sigtrans.2016.42.
- Masuda H, Zhang D, Bartholomeusz C, Doihara H, Hortobagyi GN, et al. (2012) Role of Epidermal Growth Factor Receptor in Breast Cancer. Breast Cancer Res. Treat. 136: 331- 345. https://doi.org/10.1007/s10549-012-2289-9.
- Jung M, Russell AJ, Liu B, George J, Liu PY, et al. (2017) A Myc Activity Signature Predicts Poor Clinical Outcomes in Myc-Associated Cancers. Cancer Res 77: 971-981. https://doi. org/10.1158/0008-5472.CAN-15-2906
- Ray AlpRay ARB (2015) I. of R. by
SAF ‐1/MAZ through a feed‐forward loop promotes angiogenesisin breast cancer. C M 4: 224-234. https://doi. org/10. 1002/cam4. 362an - Ray BK (2015) Induction of Ras by
SAF ‐1/MAZ through a Feed‐forward Loop Promotes Angiogenesis in Breast Cancer. Cancer Med 4: 224-234. https:// doi.org/10.1002/cam4.362. - Hientz K, Mohr A, Bhakta-Guha D, Efferth T (2017) The Role of P53 in Cancer Drug Resistance and Targeted Chemotherapy. Oncotarget 8: 8921-8946. https://doi.org/10.18632/ oncotarget.13475.
- Maffini MV, Soto AM, Calabro JM, Ucci AA, Sonnenschein C (2004) The Stroma as a Crucial Target in Rat Mammary Gland Carcinogenesis. J Cell Sci 117: 1495-1502. https://doi. org/10.1242/jcs.01000.
- Qian BZ, Pollard JW (2010) Macrophage Diversity Enhances Tumor Progression and Metastasis. Cell 141: 39-51. https://doi. org/10.1016/j.cell.2010.03.014.
- Niu Y, Chen J, Qiao Y (2022) Epigenetic Modifications in Tumor-Associated Macrophages: A New Perspective for an Old Foe. Front Immunol 13. https://doi.org/10.3389/ fimmu.2022.836223.
- Basse C, Arock M (2015) The Increasing Roles of Epigenetics in Breast Cancer: Implications for Pathogenicity, Biomarkers, Prevention and Treatment. Int J Cancer 137: 2785-2794. https:// doi.org/10.1002/ijc.29347.
- Smalley M, Piggott L, Clarkson R (2013) Breast Cancer Stem Cells: Obstacles to Therapy. Cancer Lett. 338: 57-62. https://doi. org/10.1016/j.canlet.2012.04.023.
- Walcher L, Kistenmacher AK, Suo H, Kitte R, Dluczek S, et al. (2020) Cancer Stem Cells-Origins and Biomarkers: Perspectives for Targeted Personalized Therapies. Front. Immunol 11 https:// doi.org/10.3389/fimmu.2020.01280.
- Czerwinska P, Kaminska B (2015) Review Regulation of Breast Cancer Stem Cell Features. Współczesna Onkol 1: 7-15. https://doi.org/10.5114/wo.2014.47126.
- Cadoo KA, Fornier MN, Morris PG (2013) Biological Subtypes of Breast Cancer: Current Concepts and Implications for Recurrence Patterns. Q J Nucl Med Mol Imaging 57: 312-321.
- Haque R, Ahmed SA, Inzhakova G, Shi J, Avila C, et al. (2012) Impact of Breast Cancer Subtypes and Treatment on Survival: An Analysis Spanning Two Decades. Cancer Epidemiol Biomarkers Prev 2012 21: 1848-1855. https://doi.org/10.1158/1055-9965. EPI-12-0474.
- Turashvili G, Brogi E (2017) Tumor Heterogeneity in Breast Cancer. Front. Med. 4. https://doi.org/10.3389/fmed.2017.00227.
- Lee YT, Tan YJ, Oon CE (2018) Molecular Targeted Therapy: Treating Cancer with Specificity. Eur J Pharmacol 834: 188-196. https://doi.org/10.1016/j.ejphar.2018.07.034.
- Sledge GW, Mamounas EP, Hortobagyi GN, Burstein HJ, et al. (2014) Past, Present, and Future Challenges in Breast Cancer Treatment. J Clin Oncol 32: 1979-1986. https://doi.org/10.1200/ JCO.2014.55.4139.
- Howell SJ (2013) Advances in the Treatment of Luminal Breast Cancer. Curr Opin Obstet Gynecol 25: 49-54. https://doi. org/10.1097/GCO.0b013e32835c0410.
- ReinertT, BarriosCH (2015) OptimalManagementofHormone Receptor Positive Metastatic Breast Cancer in Ther Adv Med Oncol 7: 304-320. https://doi.org/10.1177/1758834015608993.
- Baker SJ, Reddy EP (2012) CDK4: A Key Player in the Cell Cycle, Development, and Cancer. Genes Cancer 3: 658–669. https://doi.org/10.1177/1947601913478972.
- Sherr CJ, Beach D, Shapiro GI (2016) Targeting CDK4 and CDK6: From Discovery to Therapy. Cancer Discov 6: 353-367. https://doi.org/10.1158/2159-8290.CD-15-0894.
- Sammons SL, Topping DL, Blackwell KL (2017) HR+, HER2– Advanced Breast Cancer and CDK4/6 Inhibitors: Mode of Action, ClinicalActivity, and Safety Profiles. Curr Cancer Drug Targets 17. https://doi.org/10.2174/1568009617666170330120452.
- Braal CL, Jongbloed EM, Wilting SM, Mathijssen RHJ, Koolen SLW, et al. (2021) Inhibiting CDK4/6 in Breast Cancer with Palbociclib, Ribociclib, and Abemaciclib: Similarities and Differences. Drugs 81: 317-331. https://doi.org/10.1007/s40265- 020-01461-2.
- Paplomata E, O’Regan R (2014) The PI3K/AKT/ MTOR Pathway in Breast Cancer: Targets, Trials and Biomarkers. Ther Adv Med Oncol 6: 154-166. https://doi. org/10.1177/1758834014530023.
- Miller TW, Hennessy BT, González-Angulo AM, Fox EM, Mills GB, et al. (2010) Hyperactivation of Phosphatidylinositol-3 Kinase Promotes Escape from Hormone Dependence in Estrogen Receptor–Positive Human Breast Cancer. J Clin Invest 120: 2406-2413. https://doi.org/10.1172/JCI41680.
- Miller TW, Rexer BN, Garrett JT, Arteaga CL (2011) Mutations in the Phosphatidylinositol 3-Kinase Pathway: Role in Tumor Progression and Therapeutic Implications in Breast Cancer. Breast Cancer Res 13: 224. https://doi.org/10.1186/ bcr3039.
- Lee YR, Chen M, Pandolfi PP (2018) The Functions and Regulation of the PTEN Tumour Suppressor: New Modes and Prospects. Nat Rev Mol Cell Biol 19: 547-562. https://doi. org/10.1038/s41580-018-0015-0.
- Guerrero-ZotanoA, MayerIA, ArteagaCL (2016) PI3K/AKT/ MTOR: Role in Breast Cancer Progression, Drug Resistance, and Treatment. Cancer Metastasis Rev 35: 515-524. https://doi. org/10.1007/s10555-016-9637-x.
- Garrido-Castro AC, Saura C, Barroso-Sousa R, Guo H, Ciruelos E, et al. (2020) Phase 2 Study of Buparlisib (BKM120), a Pan-Class I PI3K Inhibitor, in Patients with Metastatic TripleNegative Breast Cancer. Breast Cancer Res 22: 120. https://doi. org/10.1186/s13058-020-01354-y.
- Rodon J, Dienstmann R, Serra V, Tabernero J (2013) Development of PI3K Inhibitors: Lessons Learned from Early Clinical Trials. Nat. Rev. Clin Oncol 10: 143-153. https://doi. org/10.1038/nrclinonc.2013.10.
- Juric D, Castel P, Griffith M, Griffith OL, Won HH, et al. (2015) Convergent Loss of PTEN LeadstoClinicalResistance to a PI(3)Kα Inhibitor. Nature 518: 240-244. https://doi.org/10.1038/ nature13948.
- Ellis MJ, Perou CM (2013) The Genomic Landscape of Breast Cancer as a Therapeutic Roadmap. Cancer Discov. 3: 27-34. https://doi.org/10.1158/2159-8290.CD-12-0462.
- Fruman DA, Rommel C (2014) PI3K and Cancer: Lessons, Challenges and Opportunities. Nat Rev Drug Discov 13: 140- 156. https://doi.org/10.1038/nrd4204.
- Lee JJ, Loh K, Yap YS (2015) PI3K/Akt/MTOR Inhibitors in Breast Cancer. Cancer Biol Med 12: 342-354. https://doi. org/10.7497/j.issn.2095-3941.2015.0089.
- Barchiesi G, Mazzotta M, Krasniqi E, Pizzuti L, Marinelli, D, et al (2020) Neoadjuvant Endocrine Therapy in Breast Cancer: Current Knowledge and Future Perspectives. Int J Mol Sci 21: 3528. https://doi.org/10.3390/ijms21103528.
- Ellis H, Ma CX (2019) PI3K Inhibitors in Breast Cancer Therapy. Curr Oncol Rep 21: 110. https://doi.org/10.1007/ s11912-019-0846-7.
- Juric D, Janku F, Rodón J, Burris HA, Mayer IA, et al. (2019) Alpelisib Plus Fulvestrant in PIK3CA -Altered and PIK3CA -Wild-Type Estrogen Receptor–Positive Advanced Breast Cancer. JAMA Oncol 5: e184475. https://doi.org/10.1001/ jamaoncol.2018.4475.
- Schnitzbauer AA, Zuelke C, Graeb C, Rochon J, Bilbao I, et al. (2010) A Prospective Randomised, Open-Labeled, Trial Comparing Sirolimus-Containing versus MTOR-InhibitorFree Immunosuppression in Patients Undergoing Liver Transplantation for Hepatocellular Carcinoma. BMC Cancer 10: 190. https://doi.org/10.1186/1471-2407-10-190.
- Baselga J, Campone M, Piccart M, Burris HA, Rugo HS, et al. (2012) Everolimus in Postmenopausal Hormone-Receptor– Positive Advanced Breast Cancer. N Engl J Med 366: 520-529. https://doi.org/10.1056/NEJMoa1109653.
- Sabnis GJ, Goloubeva O, Chumsri S, Nguyen N, Sukumar S, et al. (2011) Functional Activation of the Estrogen Receptor-α and Aromatase by the HDAC Inhibitor Entinostat Sensitizes ER-Negative Tumors to Letrozole. Cancer Res 71: 1893-1903. https://doi.org/10.1158/0008-5472.CAN-10-2458.
- Tong CWS, Wu M, Cho WCS, To KKW (2018) Recent Advances in the Treatment of Breast Cancer. Front. Oncol 8. https://doi.org/10.3389/fonc.2018.00227.
- Purohit A, Woo LWL, Potte, BVL (2011) Steroid Sulfatase: A Pivotal Player in Estrogen Synthesis and Metabolism. Mol Cell Endocrinol 340: 154-160. https://doi.org/10.1016/j. mce.2011.06.012.
- Stanway SJ, Delavault P, Purohit, A, Woo LWL, et al. (2007) Steroid Sulfatase: A New Target for the Endocrine Therapy of Breast Cancer. Oncologist 12: 370-374. https://doi.org/10.1634/ theoncologist.12-4-370.
- Rausch L, Green C, Steinmetz K, LeValley S, Catz P, et al.(2011) Preclinical Pharmacokinetic, Toxicological and Biomarker Evaluation of SR16157, a Novel Dual-Acting Steroid Sulfatase Inhibitor and Selective Estrogen Receptor Modulator. Cancer Chemother Pharmacol 67: 1341-1352. https://doi. org/10.1007/s00280-010-1430-x.
- Swaim SM, Miles D, Kim SB, Im, YH., Im SA, et al. (2020) Pertuzumab, Trastuzumab, and Docetaxel for HER2-Positive Metastatic Breast Cancer (CLEOPATRA): End-of-Study Results from a Double-Blind, Randomised, Placebo-Controlled, Phase 3 Study. Lancet Oncol 21: 519-530. https://doi.org/10.1016/S1470- 2045(19)30863-0.
- Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, et al. (2001) Use of Chemotherapy plus a Monoclonal Antibody against HER2 for Metastatic Breast Cancer That Overexpresses HER2. N Engl. J Med 344: 783-792. https://doi.org/10.1056/ NEJM200103153441101.
- Swain SM, Baselga J, Kim SB, Ro J, Semiglazov V, et al. (2015) Pertuzumab, Trastuzumab, and Docetaxel in HER2-Positive Metastatic Breast Cancer. N Engl J Med 372: 724-734. https:// doi.org/10.1056/NEJMoa1413513.
- Lewis Phillips GD, Li G, Dugger DL, Crocker LM, Parsons KL, et al. (2008) Targeting HER2-Positive Breast Cancer with Trastuzumab-DM1, an Antibody-Cytotoxic Drug Conjugate. Cancer Res 68: 9280-9290. https://doi.org/10.1158/0008-5472. CAN-08-1776.
- Junttila TT, Li G, Parsons K, Phillips GL, Sliwkowski MX (2011) Trastuzumab-DM1 (T-DM1) Retains All the Mechanisms of Action of Trastuzumab and Efficiently Inhibits Growth of Lapatinib Insensitive Breast Cancer. Breast Cancer Res Treat 128: 347-356. https://doi.org/10.1007/s10549-010-1090-x.
- Takada M, Toi M (2020) Neoadjuvant Treatment for HER2- Positive Breast Cancer. Chinese Clin Oncol 9: 32-32. https://doi. org/10.21037/cco-20-123.
- Figueroa-Magalhães MC, Jelovac D, Connolly RM, Wolff AC (2014) Treatment of HER2-Positive Breast Cancer. The Breast 23: 128-136. https://doi.org/10.1016/j.breast.2013.11.011.
- Tolaney S, Burris H, Gartner E, Mayer IA, et al. (2015) Phase I/II Study of Pilaralisib (SAR245408) in Combination with Trastuzumab or Trastuzumab plus Paclitaxel in TrastuzumabRefractory HER2-Positive Metastatic Breast Cancer. Breast Cancer Res Treat 149: 151-161. https://doi.org/10.1007/s10549- 014-3248-4.
- Baselga J, Bradbury I, Eidtmann H, Di Cosimo S, de Azambuja E, et al (2012) Lapatinib with Trastuzumab for HER2- Positive Early Breast Cancer (NeoALTTO): A Randomised, Open-Label, Multicentre, Phase 3 Trial. Lancet 379: 633-640. https://doi.org/10.1016/S0140-6736(11)61847-3.
- Hudis C, Swanton C, Janjigian YY, Lee R, Sutherland S, et al. (2013) A Phase 1 Study Evaluating the Combination of an Allosteric AKT Inhibitor (MK-2206) and Trastuzumab in Patients with HER2-Positive Solid Tumors. Breast Cancer Res 15: R110. https://doi.org/10.1186/bcr3577.
- Chien AJ, Cockerill A, Fancourt C, Schmidt E, Moasser MM, et al. (2016) A Phase 1b Study of the Akt-Inhibitor MK2206 in Combination with Weekly Paclitaxel and Trastuzumab in Patients with Advanced HER2-Amplified Solid Tumor Malignancies. Breast Cancer Res Treat 155: 521-530. https://doi. org/10.1007/s10549-016-3701-7.
- Hurvitz SA, Andre F, Jiang Z, Shao Z, Mano MS, et al. (2015) Combination of Everolimus with Trastuzumab plus Paclitaxel as First-Line Treatment for Patients with HER2-Positive Advanced Breast Cancer (BOLERO-1): A Phase 3, Randomised, DoubleBlind, Multicentre Trial. Lancet Oncol 16: 816-829. https://doi. org/10.1016/S1470-2045(15)00051-0.
- Acevedo-Gadea C, Hatzis C, Chung G, Fishbach N, LezonGeyda K, et al. (2015) Sirolimus and Trastuzumab Combination Therapy for HER2-Positive Metastatic Breast Cancer after Progression on Prior Trastuzumab Therapy. Breast Cancer Res Treat 150: 157-167. https://doi.org/10.1007/s10549-015-3292-8.
- Seiler M, Ray-Coquard I, Melichar B, Yardley DA, Wang, RX, et al. (2015) Oral Ridaforolimus Plus Trastuzumab for Patients With HER2+ Trastuzumab-Refractory Metastatic Breast Cancer. Clin. Breast Cancer 15: 60-65. https://doi.org/10.1016/j.clbc.2014.07.008.
- Chan A, Delaloge S, Holmes FA, Moy B, Iwata H, et al. (2016) Neratinib after Trastuzumab-Based Adjuvant Therapy in Patients with HER2-Positive Breast Cancer (Exte NET): A Multicentre, Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Oncol 17: 367-377. https://doi.org/10.1016/ S1470-2045(15)00551-3.
- Mukai H, Saeki T, Aogi K, Naito Y, Matsubara N, et al. (2016) Patritumab plus Trastuzumab and Paclitaxel in Human Epidermal Growth Factor Receptor 2‐overexpressing Metastatic Breast Cancer. Cancer Sci 107: 1465-1470. https://doi. org/10.1111/cas.13017.
- Verma S, Miles D, Gianni L, Krop IE, Welslau M, et al. (2012) Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N Engl J Med 367: 1783-1791. https://doi.org/10.1056/ NEJMoa1209124.
- Roukos DH, Lianos G, Bali C, Vlachos K, Zoras O, et al. (2014) Potential of Antibody&Ndash;Drug Conjugates and Novel Therapeutics in Breast Cancer Management. Onco Targets Ther 491. https://doi.org/10.2147/OTT.S34235.
- SmithCA, PolliceAA, GuLP, BrownKA, SinghSG, et al. (2000) Correlations among P53, Her-2/Neu, and Ras Overexpression and Aneuploidy by Multiparameter Flow Cytometry in Human Breast Cancer: Evidence for a Common Phenotypic Evolutionary Pattern in Infiltrating Ductal Carcinomas. Clin Cancer Res 6: 112-126.
- Kerklaan BM, Diéras V, Le Tourneau C, Mergui-Roelvink M, Huitema ADR, et al. (2013) Phase I Study of Lonafarnib (SCH66336) in Combination with Trastuzumab plus Paclitaxel in Her2/Neu Overexpressing Breast Cancer: EORTC Study 16023. Cancer Chemother. Pharmacol 71: 53-62. https://doi. org/10.1007/s00280-012-1972-1.
- Mehanna J, Haddad FG, Eid R, Lambertini M, Kourie HR (2019) Triple-Negative Breast Cancer: Current Perspective on the Evolving Therapeutic Landscape. Int J Womens Health 11: 431-437. https://doi.org/10.2147/IJWH.S178349.
- Akshata Desai KA (2012) Triple Negative Breast Cancer – An Overview. Hered Genet https://doi.org/10.4172/2161-1041. S2-001 .
- Berrada N, Delaloge S, André F (2010) Treatment of TripleNegative Metastatic Breast Cancer: Toward Individualized Targeted Treatments or Chemosensitization? Ann Oncol 21: vii30–vii35. https://doi.org/10.1093/annonc/mdq279.
- Comen EA, Robson M (2010) Poly(ADP-Ribose) Polymerase Inhibitors in Triple-Negative Breast Cancer. Cancer J 16: 48-52. https://doi.org/10.1097/PPO.0b013e3181cf01eb.
- Telli ML, Hellyer J, Audeh W, Jensen KC, Bose S, et al. (2018) Homologous Recombination Deficiency (HRD) Status Predicts Response to Standard Neoadjuvant Chemotherapy in Patients with Triple-Negative or BRCA1/2 Mutation-Associated Breast Cancer. Breast Cancer Res. Treat. 168: 625-630. https://doi. org/10.1007/s10549-017-4624-7.
- Castrellon AB, Pidhorecky I, Valero V, Raez LE (2017) The Role of Carboplatin in the Neoadjuvant Chemotherapy Treatment of Triple Negative Breast Cancer. Oncol Rev https:// doi.org/10.4081/oncol.2017.324.
- Bryant HE, Schultz N, Thomas HD, Parker KM, Flower D, et al. (2005) Specific Killing of BRCA2-Deficient Tumours with Inhibitors of Poly(ADP-Ribose) Polymerase. Nature 434: 913- 917. https://doi.org/10.1038/nature03443.
- Turner NC, Telli ML, Rugo HS, Mailliez A, Ettl J, et al. (2017) Final Results of a Phase 2 Study of Talazoparib (TALA) Following Platinum or Multiple Cytotoxic Regimens in Advanced Breast Cancer Patients (Pts) with Germline BRCA1/2 Mutations (ABRAZO). J Clin Oncol 35: 1007-1007. https://doi.org/10.1200/ JCO.2017.35.15_suppl.1007.
- Linderholm BK, Hellborg H, Johansson U, Elmberger G, Skoog L, et al. (2009) Significantly Higher Levels of Vascular Endothelial Growth Factor (VEGF) and Shorter Survival Times for Patients with Primary Operable Triple-Negative Breast Cancer. Ann Oncol 20: 1639-1646. https://doi.org/10.1093/ annonc/mdp062.
- Gullo G, Eustace AJ, Canonici A, Collins DM, Kennedy MJ, et al. (2019) Pilot Study of Bevacizumab in Combination with Docetaxel and Cyclophosphamide as Adjuvant Treatment for Patients with Early Stage HER-2 Negative Breast Cancer, Including Analysis of Candidate Circulating Markers of Cardiac Toxicity: ICORG 08–10 Trial. Ther Adv Med Oncol 11: 175883591986423. https://doi.org/10.1177/1758835919864236.
- Hashmi AA, Naz S, Hashmi SK, Irfan M, Hussain ZF (2019) Epidermal Growth Factor Receptor (EGFR) Overexpression in Triple-Negative Breast Cancer: Association with Clinicopathologic Features and Prognostic Parameters. Surg Exp Pathol 2: 6. https://doi.org/10.1186/s42047-018-0029-0.
- Carey LA, Rugo HS, Marcom PK, Mayer EL, Esteva FJ, et al (2012) TBCRC 001: Randomized Phase II Study of Cetuximab in CombinationwithCarboplatin in Stage IV Triple-NegativeBreast Cancer J Clin Oncol 30: 2615-2623. https://doi.org/10.1200/ JCO.2010.34.5579.
- Baselga J, Gómez P, Greil R, Braga S, Climent MA, et al. (2013) Randomized Phase II Study of the Anti–Epidermal Growth Factor Receptor Monoclonal Antibody Cetuximab With Cisplatin Versus Cisplatin Alone in Patients With Metastatic Triple-Negative Breast Cancer. J Clin Oncol 31: 2586-2592. https://doi.org/10.1200/JCO.2012.46.2408.
- Finn RS, Bengala C, Ibrahim N, Roché H, Sparano J, et al. (2011) Dasatinib as a Single Agent in Triple-Negative Breas Cancer: Results of an Open-Label Phase 2 Study. Clin Cancer Res 17: 6905-6913. https://doi.org/10.1158/1078-0432.CCR-11-0288.
- Kim EMH, Mueller K, Gartner E, Boerner J, (2013) Dasatinib Is Synergistic with Cetuximab and Cisplatin in Triple-Negative Breast Cancer Cells. J Surg Res 185: 231-239. https://doi. org/10.1016/j.jss.2013.06.041.
- Rose AAN, Biondini M, Curiel R, Siegel PM (2017) Targeting GPNMB with Glembatumumab Vedotin: Current Developments and Future Opportunities for the Treatment of Cancer Pharmacol Ther 179: 127-141. https://doi.org/10.1016/j. pharmthera.2017.05.010.
- Rose AAN, Grosset AA, Dong Z, Russo C, MacDonald PA, et al. (2010) Glycoprotein Nonmetastatic B Is an Independent Prognostic Indicator of Recurrence and a Novel Therapeutic Target in Breast Cancer. Clin Cancer Res 16: 2147-2156. https:// doi.org/10.1158/1078-0432.CCR-09-1611.
- Nanda R, Chow LQM, Dees EC, Berger R, Gupta, S, et al. (2016) Pembrolizumab in Patients With Advanced TripleNegative Breast Cancer: Phase Ib KEYNOTE-012 Study. J Clin Oncol 34: 2460-2467. https://doi.org/10.1200/JCO.2015.64.8931.
- Adams S, Loi S, Toppmeyer D, Cescon DW, De Laurentiis M, et al. (2017) Phase 2 Study of Pembrolizumab as First-Line Therapy for PD-L1–Positive Metastatic Triple-Negative Breast Cancer (MTNBC): Preliminary Data from KEYNOTE-086 Cohort B J Clin Oncol 35: 1088-1088. https://doi.org/10.1200/ JCO.2017.35.15_suppl.1088.
- Martins P, Jesus J, Santos S, Raposo L, Roma-Rodrigues C, et al. (2015) Heterocyclic Anticancer Compounds: Recent Advances and the Paradigm Shift towards the Use of Nano medicine’s Tool Box. Molecules 20: 16852-16891. https://doi. org/10.3390/molecules200916852.
- Kalaria PN, Karad SC, Raval DK (2018) A Review on Diverse Heterocyclic Compounds as the Privileged Scaffolds in Antimalarial Drug Discovery. Eur J Med Chem 158: 917-936. https://doi.org/10.1016/j.ejmech.2018.08.040.
- Peerzada MN, Khan P, Khan NS, Gaur A, Avecilla FA, et al. (2020) Identification of Morpholine Based Hydroxylamine Analogues: Selective Inhibitors of MARK4/Par-1d Causing Cancer Cell Death through Apoptosis. New J Chem 44: 16626- 16637. https://doi.org/10.1039/D0NJ03474F
- Peerzada MN, Gaur A, Azam A (2021) Advances in Drug Discovery against Neglected Tropical Diseases: Human African and American Trypanosomiasis. Curr Med Chem https://doi.or g/10.2174/0929867328666210504111442.
- Taylor AP, Robinson RP, Fobian YM, Blakemore DC, Jones LH, et al. (2016) Modern Advances in Heterocyclic Chemistry in Drug Discovery. Org Biomol Chem 14: 6611-6637. (2015) https://doi.org/10.1039/C6OB00936K.
- Lahlou M (2013) The Success of Natural Products in Drug Discovery. Pharmacol & Pharm 04: 17-31. https://doi. org/10.4236/pp.2013.43A003.
- Atanasov AG, Zotchev SB, Dirsch VM, Supuran CT (2021) Natural Products in Drug Discovery: Advances and Opportunities. Nat. Rev. Drug Discov 20: 200-216. https://doi. org/10.1038/s41573-020-00114-z.
- Peerzada MN, Khan P, Khan NS, Avecilla F, Siddiqui SM, et al. (2020) Design and Development of Small-Molecule Arylaldoxime/5-Nitroimidazole Hybrids as Potent Inhibitors of MARK4: A Promising Approach for Target-Based Cancer Therapy. ACS Omega 5: 22759-22771. https://doi.org/10.1021/ acsomega.0c01703.
- Azam A, Peerzada MN, Ahmad K (2015) Parasitic Diarrheal Disease: Drug Development and Targets. Front. Microbiol 6. https://doi.org/10.3389/fmicb.2015.01183.
- Jampilek J (2019) Heterocycles in Medicinal Chemistry. Molecules 24: 3839. https://doi.org/10.3390/molecules24213839.
- Peerzada MN, Hamel E, Bai R, Supuran CT, Azam A (2021) Deciphering the Key Heterocyclic Scaffolds in Targeting Microtubules, Kinases and Carbonic Anhydrases for Cancer Drug Development. Pharmacol Ther 225: 107860. https://doi. org/10.1016/j.pharmthera.2021.107860.
Artcle Information
Review Article
Received Date: September 12, 2022
Accepted Date: October 12, 2022
Published Date: October 15, 2022
Journal of Pharmacogenetics and Precision Medicine
Volume 1 | Issue 1
Citation
ASharif KN, Nabi PM, Bashir S, Azam A (2022) Molecular Insight into Key Targets and Inhibitors for Breast Cancer Treatment. J Pharmacogenet and Precis Med 1: 1-20
Copyright
©2022 Azam A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jppm.2022.1.101