

Research Article
Volume-1 Issue-1, 2021
Giant Segmental Emphysema: Itinerary and Care Circuit in a Resource-Limited Country. A Case Report
-
Received Date: September 02, 2021
-
Accepted Date: October 02, 2021
-
Published Date: October 04, 2021
Journal Information
Switch to Full Text Menu
Abstract
Giant lobar emphysema is a congenital lung malformation characterized by hyper-expansion of a segment, a lobe or several lobes. It is classically obstructive, causing compression of the adjacent parenchyma, leading to neonatal respiratory distress. This is a case study of an 11-month-old infant treated surgically at Kamenge University Teaching Hospital (KUTH)for congenital segmental emphysema. We described the difficulties encountered for the positive diagnosis and the itinerary followed by the patient since the prenatal consultations with his mother. It is one of the bronchopulmonary malformations that, when the diagnosis and management are done correctly, the prognosis is excellent. The left lung side is more affected and the male sex is predominant. Diagnosis can be antenatal by imaging or postnatal by respiratory signs. The standard X-ray strongly suspects the diagnosis which is confirmed by the thoracic CT scan. Its confinement to a given segment is often known intraoperatively. Thoracic drainage of the bulla would cause a pneumothorax or simply a recurrence with the risk of a mass effect when the drain is removed. The radical treatment is surgical and consists in a segmentectomy (exeresis of the area with emphysema). The evolution is favorable in our case and in the literature.
Key words
Segmental Emphysema; Congenital; Diagnostic Difficulties; Surgery
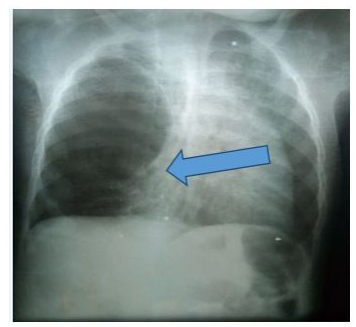 |
| Figure 1: Standard radiograph showing a clear image of the lung must, upper lobe, compression mass effect (large arrow) |
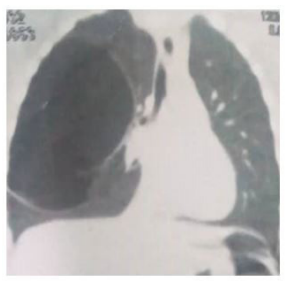 |
| Figure 2: Chest CT scan, coronal section, hypodense image involving the right upper lobe |
 |
| Figure 3: Intraoperative image, emphysema (thin arrow in blue), healthy segment of the right upper lobe (solid arrow in blue) |
 |
| Figure 4: Drained bullectomy area (thin arrow) |
 |
| Figure 5: X-ray D1PO, drain in place, pulmonary expansion |
 |
| Figure 6: Control radiograph after respiratory physiotherapy (at D30PO), good right pulmonary expansion |
Introduction
HIV/AIDS Bronchopulmonary malformations (BPMs) result from developmental accidents of the bronchopulmonary system. They are rare and polymorphic conditions among which congenital giant lobar emphysema (GLE) represents 3 to 15% [1, 2]. They constitute a spectrum of developmental anomalies whose classification and pathophysiology remain controversial [4]. They are secondary to abnormal embryonic lung development occurring between the sixth and 17th week of gestation [3]. They may involve different anatomical components of the lung, the parenchyma, the airways, the arterial supply and/or the venous drainage [5]. The modes of clinical presentation vary greatly from neonatal respiratory distress to incidental detection in an asymptomatic adult [5]. Congenital giant segmental emphysema is an even rarer topographic variant of giant lobar emphysema, which can also progress to respiratory distress [6]. Nowadays, its diagnosis is more and more often antenatal, and it is then called fetal lobar emphysema (FLE), by detection of a pulmonary signal abnormality during morphological ultrasound [7]. We report a case of congenital emphysema confined to the inferior segment of the right upper lobe, managed at the University Hospital of Kamenge. The treatment performed was bullectomy by removal of the segment affected by the emphysema.
Case Report
This was an 11-month-old infant, male, first of his siblings and born by caesarean section who was referred to us for assessment and management of mild respiratory distress. In this history there is a notion of fetal pulmonary cyst discovered during obstetrical ultrasounds and repetitive episodes of cough, rhinorrhea and fever attributed to repetitive pneumopathies followed regularly. On the other hand, small attacks of dyspnea associated with cough that occurred intermittently since birth were treated medically. Elsewhere, the interrogation did not reveal any notion of malformation in the family. On admission, the infant presented with mild respiratory distress with a respiratory rate of 28 cycles per minute, a room air saturation of 92%, a pulse rate of 100 beats per minute, a good general condition with a weight of 8.9 kg. Physical examination revealed thoracic asymmetry without a draw. A tympanum of the right hemothorax was found on percussion associated with a homolateral decrease in vesicular murmurs. The chest X-ray showed a hyperclar image (Figure 1) and the thoracic CT scan that was performed to better understand the cause of this hyper clarity noted a very large aerial cavity filling the right lung thus concluding to an image in favor of congenital giant emphysema occupying the right upper lobe (Figures 2). A multidisciplinary analysis then decided on a right upper lobectomy. During the procedure, the emphysema was localized in the lower segment of the upper lobe. Thus, a segmental congenital emphysema was retained as a positive diagnosis. A bullectomy and thoracic drainage were performed (Figures 3 and 4). The postoperative course was simple. The radiological control was done at Day (D)1 post-operatively (PO), (Figure 5), then at D8PO and the drain was removed at D9PO. Respiratory physiotherapy was performed as soon as the chest tube was removed in the outpatient clinic, with a good clinical and radiological evolution (Figure 6).
Discussion
Congenital lobar emphysema is a rare condition, with a prevalence of 1/20,000 to 1/30,000 births [8]. It is usually a unilateral pathology. It classically affects more boys than girls. In its typical form, it most often affects the left upper lobe (42% of cases), the middle lobe (35%) and the right upper lobe (20%) [9]. Our case was a boy with segmental emphysema involving the lower segment of the right upper lobe. Bilateral ELC is extremely rare and has been reported in the international literature only exceptionally, in about ten children. The vast majority of cases involved left upper and right middle lobar involvement [7].
A few familial cases of ELC have been reported, in a father and son by Robert [10] in 2002 or in a mother and daughter by Wall [11] in 1982, or within the same sibling by Hendren [12] and Sloan [13], suggesting a genetic cause. However, in our situation, it seems to be a sporadic congenital pathology.ELC is classically described as the consequence of a bronchial obstruction. This obstacle can be either intrinsic by anomaly or absence of the bronchial cartilage, a left sliding bronchus, a mucus plug, an endo-luminal tumor. It can also be extrinsic due to compression by a pulmonary vessel, a bronchogenic cyst or a tumor (teratoma, neuroblastoma) [4]. Rare causes such as a mediastinal mass, a polyalveolar lobe, a bronchial torsion, a bronchial septum have been described [7]. No etiology is found in 50% of cases [14]. In our situation, the etiological investigation was not done. Right segmental emphysema (RSE), our case study, is a rare topographic variant of right lobar emphysema (RLE) as reported by Moussa Outtara et al but in them the segmental emphysema was on the left [6]. The diagnosis of congenital emphysema is important, especially in antenatal care, because most of these lesions, when they remain asymptomatic and reach a restricted pulmonary territory, do not require surgical management, unlike other bronchopulmonary malformations which are more likely to become complicated and require preventive removal. This diagnosis can be antenatal, although rarely made, as noted by Ankermann in a meta-analysis that reports 12 cases of antenatal lung lesions confirmed histologically as ELC [1, 2, 6, 15]. The diagnosis usually occurs during the 2nd trimester ultrasound, where the lung then takes on a homogeneous hyperechoic appearance. In our patient, prenatal ultrasound had suspected a fetal lung lesion of cystic nature.
This diagnosis can also be post-natal, on clinical point of call, ranging from severe respiratory distress to discrete non-specific respiratory symptoms. At birth, the standard chest radiograph shows a lobar opacity as long as the lesion is filled with alveolar fluid. In our infant, the diagnosis was suspected clinically (recurrent pneumonitis) and by chest radiography and confirmed by chest CT. However, the segmental location in the right upper lobe was an intraoperative diagnosis, this would be explained by the importance of distension which made it difficult to identify the anatomical segmentation of the homolateral lung. Treatment consists of lobectomy or segmentectomy depending on the location of the emphysema after stabilization of respiratory function [6, 16, 17]. Thoracic pleural drainage is contraindicated, as it would only worsen the clinical scene, with perforation of the lung parenchyma, since there is no pneumothorax [3, 6]. Surgical abstention is possible for asymptomatic or pauci-symptomatic lesions. However, because of the risk of recurrent infection, some authors recommend a systematic elective lobectomy [18, 19].
In segmental forms, as in our case, because of the impact of the distended segment on the mediastinum, the homolateral and contralateral lung parenchyma, surgery seems to be the radical treatment because it allows to lift the compression [6, 7, 20, 21]. It has the advantage of allowing segmental anatomical exeresis and therefore a greater parenchymal sparing than in the lobar form. The postoperative course was simple in our infant who was followed for 2 months. Simple postoperative courses have been reported in the literature [18, 19, 20, 21].
Conclusion
Bronchopulmonary malformations are rare. They are most often revealed early. Antenatal screening by ultrasound would allow to transform their management which must be multidisciplinary. Congenital segmental emphysema is a topographic clinical form of giant lobar emphysema with the same evolutionary risks and a similar management. The prevention of possible complications leads to the recommendation of early surgery because rare cases evolve to spontaneous involution but most become complicated.
References
- Stocker JT (1994) Congenital and developmental diseases, In: Dail DH, Hammar SP, Editors. Pulmonary pathology. Berlin Springer-Verlag 155-81.
- P Monin, F Didier, P Vert, J Prevot, F Plena (1979) Giant lobar emphysema neonatal diagnosis. Pediatr Radiol 8: 259-60.
- Rabiaa Ben Abdallah, Habib Bouthour, Youssef Hellal, Mohamed Riadh Ben Malek, Youssef Gharbi (2013) Les Malformations Broncho-Pulmonaires: Radiological and therapeutic diagnostic aspects. Medical Tunisia - 91: 66 -9
- L Berteloot, A Bobbio, AE Millischer-Bellaïche, K Lambot, S Breton, et al. (2012) Congenital malformations of the lung, the radiologist’s point of view. Revue des Maladies Respirators 29: 820-35
- Pooja Abbey, Mahender K Narula, Rama Anand (2014) Congenital Malformations and Developmental Anomalies of the Lung. Curr Radiol Rep 2:71
- Moussa AbdoulayeOuattara, Seydou Togo, BouramaKané, SadioYena (2016) Congenital compressive giant segmental emphysema: diagnosis and treatment. Pan Afr Med J 23:17
- Pierre-Yves Rabattu (2015) Fetal lobar emphysema : about 21 observations. Human medicine and pathology. Dumas-01225719.
Article Information
Research Article
Received Date: September 02, 2021
Accepted Date: October 02, 2021
Published Date: October 04, 2021
Evaluation of the Antimicrobial Activity of the Bark Extracts of Tamarindus indica, Adansonia digitata and Vitellaria paradoxa, and their Combinations against Some Selected Clinical Pathogens
Volume 1 | Issue 1
Citation
JC Mbonicura, T Sibomana, F Ndikumwenayo, E Ndirahisha, C Murekatete, et al. (2021) Giant Segmental Emphysema: Itinerary and Care Circuit in a Resource-Limited Country. J Pulm Res and Ther 1101
Copyright
©2021 Thierry Sibomana. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jaar.2021.1.101