

Research Article
Volume-1 Issue-1, 2021
Effect of NMES on Quadriceps Strength and Endurance in Chronic Obstructive Pulmonary Disease Patients: A Narrative Review
-
Received Date: April 21, 2024
-
Accepted Date: May 21, 2024
-
Published Date: May 24, 2024
Journal Information
Switch to Full Text Menu
Abstract
Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) is known to causeprimary respiratory complications and secondary musculoskeletal affects, The use of Neuromuscular Electrical Nerve stimulation (NMES) is investigated for treatment in patients suffering from AECOPD, however, the current literature is limiting its effects on muscle strength and endurance in moderate to severe acute exacerbating COPD patients. The authors aimed at identifying literature on the efficacy of NMFS on quadriceps strength and endurance in moderate to severe COPD patients during an acute exacerbation requiring hospitalization. The research ques. tion was formulated using the PICO framework (P) males or females over the age of 45, (I) NMES, (C) pulmonary rehabilitation (PR), work-rate cycling endurance test (CWRT), two exercise programmers or two different uencies, (O) improved quadriceps strength and endurance. A thorough search of academic literature was carried out using various electronic databases and manual reference searching. Filters and specific criteria were used to narrow down the search results. 10 Randomized controlled trials (RCTs) written in English were included in this review. 'Ihe CASP tool was utilized for the critical assessment and evaluation of the literature. Literature reports that both quadriceps strength and endurance improve following the application of NMES, with high. frequency NMES proving to be more beneficial than low. frequency and duration of Intervention. The prime limitation in all the studies analyzed was the small sample size, while other limitations included the inability to mask assessors and hence bias and short study duration. Findings from the reviewed articles suggest that NMES aids in improving quadriceps strength and endurance through various tests for either of the outcome measures.
Key words
NMES; COPD; Quadriceps; Exacerbation; Acute
Population |
Intervention |
Comparison |
Outcome |
Males and females over the age of 40 |
NMES |
NMES intervention on COPD patients admitted to ICU with a COPD exacerbation |
Quadriceps Maximal Voluntary Contraction |
COPD patients with a moderate to |
|
Different NMFS frequency in combination with |
Quadriceps Endurance |
|
|
NMES intervention compared to a non- stimulated lower limb |
|
Criterion |
Inclusion |
Exclusion |
Language of article |
Published in English |
Published in another language other than English |
Publication date |
A study published less than 13 years ago |
Study published more than 13 years ago |
Statistical method used |
Descpription of the statiscial method used is present |
Description of the statistical method used is not present |
Patient selection |
Information on patient selection needed to |
Information on patient selection was not provided study |
Age |
Above the age of 40 |
Under the age of 40 |
Study design |
Randomised control trial with pre-test and post-test experimental design |
Systematic Review, Meta-analysis, Non-randomised control trial, Randomised control trial with another experimental design |
Outcome measures |
The study eximained one or more of the |
Does not assess any of the primary outcome measures |
Intervention period |
The acute effects of NMES was investigated |
The chronic effects of NMES in combination of |
| Author and Year of Publication | Title | Research Design and Data Collection Instrument | Results | Strengths and Limitations |
|---|---|---|---|---|
| Abdellaoui et al., (2011) | Skeletal muscle effects of electro. stimulation after COPD Exacerbation: A Pilot Study |
Patients were randomly assigned to sham or NMES training The Sham group had weekly therapeutic education sessions, daily active–passive mobilisation and sham electrostirnulation. The ICU, atter baseline NMES group followed the same programme but received effective electro- |
At the end of the study, quadriceps force improvement was statistically different between groups (p50.02), with a significant increase only in the NMES group (median (interquartile range) 10 (4.7– 11.5) kg; p50.01). Changes in the 6-min walking distance increase only in the NMES group (median (interquartile range) 10 (4.7– 11.5) kg; p50.01). Changes in the 6-min walking distance Were statisticallv different between groups (p50.008), with a significant increase in the NMES group (165 (125–203) m; p50.003). NMES did not lead to higher muscle oxidative stress, as indicated by the decrease in total protein carbonylation (p50.02) and myosin heavy chain carbonylation (p50.01) levels. Finally, we observed a significantincrease in type i fiber proporties in the NMES group. |
Small sample size, Muscle biopsy resulting in COPD exacerbating patients to withdrawn or refuse |
| Chaplin et al., (2012) | Neuromuscular Stimulation of Quadriceps in Patients Hospitalised during an Exacerbation of COPD: A Comparison of Low (35 Hz) and High (50 Hz) Frequencies | Experimental study - Pilot Study Tests carried out: Quadriceps maximal voluntary contraction and Endurance Shuttle walk test (ESWT) | A total of 10 patients in each treatment group underwent NMES during hospitalisation (mean [SD] age 68.0 [7.4] years, characteristics between groups. Muscle strength (legs combined) increased in both groups regardless of the NMES frequency used (35 Hz - 3.8 ±4.9; 50 Hz - 3.4 |
Small sample size, and number of assessors recorded the baseline and discharge outcome measures, thus inter- assessor reliability may have been compromised |
Giavedoni et al., (2012) |
Neuromuscular electrical stimulation prevents muscle function deterioration in exacerbated COPD: A pilot study. |
Pilot study Tests carried out: Anthropometric measures, lung function, muscle strength using the QMVC. |
Mean quadriceps muscle strength decreased in control legs (DQMVC 2.9 ±5.3 N, p Z ns) but |
Abstance of a sham control leg as an unbiased control, relatively small number of subjects of participants while the muscle measuring technique was dependent on the
|
Zanotti et al., (2012) |
Combination of Pulmonary Rehabilitation and Neuromuscular ElectricalStimulation in COPD Patients: A Randomised Clinical trail of efficacy
|
Randomised Clinical of efficacy test carried |
Quadriceps strength was enhanced by SSPR (STST + 7±1.7 repetitions; p≤0.001); NMPRfurther increased strength (+10±1.6 repetitions; p≤0.001) |
The method to |
Sillen et al., (2014) |
Efficacy of lower limb |
A prospective, single- blind, randomised controlled trial was designed.Tests carried out: isokinetic quadriceps muscle function – Biodex, 6MWT, work-rate cycling endurance test (CWRT), Hopsital Anxiety and Depression Scale (HAD Score), St. George’s Repiratory Questionnaire, Canadian Occupational Performance Measure (COPM), BMI, Fat-free mass index, mMRC and Anthropometric measures. |
Quadriceps muscle strength increase in quadriceps muscle strength and muscle endurance was greater after H F-NN'I ES than |
Strength: Largest RCT till date and outcome assessors were blinded for group allocation Limitations: underpowered to detect statistically |
Vieria et al., (2014) |
Neuromuscular electrical stimulation improves clinical and physiological function in COPD patient. |
A prospective double- blind, randomised, pilot study was conducted to compare the use of NMES to a control intervention. Tests carried out: Fat free mass (FFM) and thigh circumference, spirometry, cardiopulmonary exercises test using an electronically braked cycle ergometer, 6MWT, NF-a and b- endorphin analysisand quality of life using the SGRQ. |
Compared with the control group, NMES increased FEV1 and FEV1/FVC, 6-MWD and Tlim (P < 0.01) and reduced BDS and SGRQ (P < 0.01). |
N/A |
Maddocks et al., (2015) |
Neuromuscular electrical stimulation to improve exercise capacity in patients with severe COPD: a randomised double-blind, placebo- controlled trial |
A double-blind, placebo- controlled trial. Tests carried out: 6MWT, quadriceps twitch tension (TwQ), isometric quadriceps maximum voluntary contraction (QMVC), rectus femoris cross-sectional area (RFCSA) assessed by ultrasonography, whole- body fat-free mass assessed by bioelectrical impedance analysis, daily step count, time spent upright, number of sit-to-stand transitions, health-related quality of life using the EuroQol 5-dimension |
Change in 6MWT distance was greater in the active NMES group (mean 29·9 [95% CI 8·9 to 51·0]) compared with in the placebo group (–5·7 [–19·9 to 8·4]; mean |
Limitations: not able to mask the nurses and physiotherapists who were involved in recording of adverse event data, although events |
Kucio et al., (2016) |
Evaluation of the Effects |
Randomised control trial Tests carried out: Exercise tolerance – 6MWT, Spirometric test and Gasometric test |
Pre-intervention the distance walked amounted to 397.2 ± 70.65m and 421.4 ± 69.4 m in the |
Limitations: Short period of observation of COPD patients, low number of participants. |
López- López et al., (2021) |
A Feasibility and Efficacy |
A randomised single-blind clinical trial. Tests carried out: Quadriceps strength, balance through the One- leg standing balance test (OLS), Health related QoL through the EuroQol-5D (EQ-5D) and adverse reactions. |
At the end of the intervention, |
Limitations: lack of long-term follow up and a small sample size. |
Péran et al., (2022) |
Effect of neurom uscular |
Randomised Control Trial: Tests carried out: 1-MSTS, 6MWT, isometric quadriceps maximal voluntary contraction, quadriceps endurance, SGRQ, Borg Scale and spirometry – dynamic hyperinflation.
|
No significant difference was seen |
Limitations: Duration of PR was too short, patients feeling during NMES program was not collected, no sham stimulation group, |
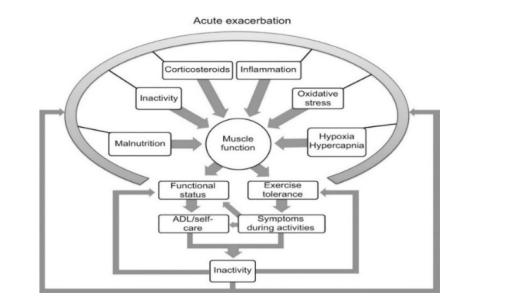 |
| Figure 1: The Acute Exacerbation as illustrated by Buttin et (2011) |
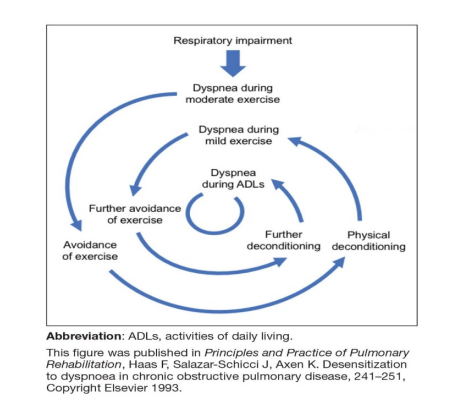 |
| Figure 2: The Dyspnoea Spiral adopted from Haas F. et, ( 1993) |
 |
| Figure 3: The PRISMA Flow Diagram (Page MJ et al.. PRISMA 2020 statement) |
 |
| Figure 4: Cochrane Risk-of-Bias Tool |
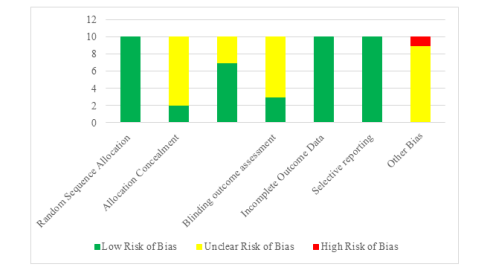 |
| Figure 5: Summary of Risk-of-Bias |
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a respira- tory condition characterised by a combination of small airway disease and destruction, features typical of emphysema Ill. De Brandt et al., 12,31 further emphasise that COPD is distinguished by persistent airflow limitation, a significant contributor to global morbidity and disease burden, as noted by Mathur et ale, [41. Maddocks et al 151 report that one in every 8 patients experiencing an exacerbation requires hospitalisation.
In addition to pulmonary changes and respiratory impairments, patients diagnosed with COPD also undergo systemic morphological and biomechanical alterations leading to modified muscle morphology, particularly affecting strength, and physiology, especially in the lower limbs [6]. Bicxhemical changes primarily result from long-term steroid use and Chronic Systemic Inflammatory Syndrome (CSIS) (7) , impacting the patient's physical capacity for activity, as depicted in Figures 1 and 2. Such changes result in more energy expenditure during activities of daily living (ADLs), resulting in short. ness of breath (SOB) following minimal exercises.
Neuro Muscular Electrical Stimulation (NMES) is a non-invasive method of muscle contraction initially introduced for post-muscle injury and surgery rehabilitation and later extended to certain diseases [8]. It is a self-administered device that does not necessitate supervision and imposes a low metabolic load, offering a viable therapy for patients with a high symptom burden [5].
Literature discussing NMES in COPD suggests its applicability during both medically stable and unstable phases [9-11], serving as an alternative to mobilisation and exercise due to its lack of requirement for active patient participation. Hill et al., [12] document how NMES, either alone or combined with conventional exercise training, enhances peripheral muscle condition, exercise capacity, endurance, functional performance, symptom reduction, and health-related quality of life (HRQoL). The additional application of electrical nerve stimulation to an exercise programme has shown to reduce the duration of bed confinement during acute severe stages of the disease [12].
While research on NMES’s effect on lower limb muscle strength spans over two decades, limited research is available on its use during acute exacerbations of COPD (AECOPD), with most studies conducted in a home-based environment. Studies by Abdellaoui et al., [13], Giavedoni et al., [11], Vieira et al., [10] and Kucia et al., [14], recruited small populations, thereby limiting the validity and reliability of outcomes. The primary focus of this review was not directed towards the detailed analysis of NMES protocols. Instead, this aspect is considered an avenue for exploration and investigation in future research projects. This deliberate decision highlights the intention to pave the way for future exploration and in-depth scrutiny of diverse protocols within the scope of research. However, all the articles included had similar NMES protocols, with frequencies ranging from 35Hz to 50Hz. They also stimulated similar groups of muscles and enrolled patients with a similar severity category.
Methodology
A narrative review design was chosen for this study to facilitate comprehensive research. The Population (P), Intervention (I), Comparator (C) and Outcome (O) (PICO) framework guided the inclusion criteria and reporting of study characteristics. Papers were retrieved through thorough searches using Google Scholar, HyDi (Hybrid Discovery), EBSCO, Pubmed, Medline, Cochrane Central Register of Controlled Trials, and Science Direct.
Table 1 illustrates the key PICO search terms. Data extraction and critical appraisal were conducted using the Critical Appraisal Skills Programme (CASP) tool to ensure quality research appraisal, focusing on study characteristics, participant demographics, intervention details, and results.
Search StrategyThe search strategy yielded over 20,000 research articles following a preliminary search through the selected databases. After eliminating duplicates (n=1740), records marked as ineligible (n=9573), records excluded based on publication date (n=1400), further elimination of excluded articles (n=478), and reports that were not retrieved (n=1432), as well as reports that were excluded (n=5366), a total of 10 full-text randomised-control trials (RCTs) with pre-test and post-test experimental designs were retained as potentially main articles. The PRISMA flow chart (Figure 3) illustrates the search strategy trail, summarising the entire screening process used by the reviewer and resulting in the selection of 10 RCT articles. Studies were then further screened according to the inclusion and exclusion criteria (see Table 2).
Different CASP checklists are utilised for different research designs. In this narrative review, an RCI' CASP (2020) was deemed suitable as all the reviewed articles were RCTs. CASP enables a thorough and methodical assessment of the quality of selected studies, highlighting their methodological strengths and weaknesses while elucidating the significance of their conclusions (15).
Study Selection and Quality AppraisalA total of 10 articles were reviewed. Table 3 summarises these articles, discussing the effects of NMES as an adjunct to chest and mobility exercises, breathing exercises, and breathing and chest mobility exercises during the acute phase.
Results
Outcome Measures used in these InterventionsThe identified studies focus on 7 outcome measures which in- clude the Quadriceps Maximal Voluntary Contraction (QMVC), 1 -minute Sit-to-stand (IMSTS), 6-minute walk test (6MWT), St- George's Respiratory Questionnaire (SGRQ), Medical Research Council (MRC) scale and lung function test. FEVI/FVC ratio or prediction was investigated in all 10 studies and QMVC was investigated in 7 studies (Abdellaouui et Chaplin et al., [16] [p< 0.04], Zanotti et al., [17] [p< 0.001], Sillen et al., [18] [p< 0.01], Maddocks et al., [5] [p=0.028], López- López et al., [19] [p< 0.001] and Péran et al., [20] [p< 0.001]). e 1-minute Sit-to-stand was investigated in 2 studies (Sillen et al., [18] [p≤0.05] and Péran et al., [20] [p< 0.01]), the 6MWT was investigated in 6 studies (Abdellaoui et al., [13] [p=0.008], Sillen et al., [18] [p< 0.01], Vieria et al., 2014 [p< 0.01], Maddocks et al., [5] [p=0.005], Kucio et al., [14] [p=0.001], López- López et al., [19] [p< 0.001] and Péran et al., [20] [p< 0.001]). The Endurance Shuttle walk test (ESWR) and work-rate cycling endurance test (CWRT) were investigated in 1 study respectively (Chaplin et al., [16] [p=0.001] and Sillen et al., [18] [p< 0.01]). Five studies investigated the St. George’s Respiratory Questionnaire (Zanotti et al., [17] [p=0.01], Sillen et al., [18] [p< 0.01], Vieria et al., [10] [p< 0.01], Maddoks et al., [5] [p=0.78] and Péran et al., [20] [p< 0.001]). Health-related quality of life was also investigated by 2 more studies using the EuroQol-5D questionnaire (Maddocks et al., [5] [p< 0.05]) and López- López et al., [19] [p< 0.05]) and the Canadian Occupational Performance Measure COPM (Sillen et al., [18] [p< 0.05] with no statistical difference between the groups. MRC was investigated in 1 study (Chaplin et al., [16] [p< 0.75] for both the experimental and control groups) while Modified Medical Research Council (mMRC) was investigated in 2 studies (Zanotti et al., [17] [p=0.01] and Sillen et al., [18] [p< 0.01]).
Critical Evaluation of ArticlesAll studies included had an unclear risk of bias and limitations in reporting quality when assessed using the Cochrainerisk of bias 2.0 toll (Cochrane RoB2) for randomized trials. All studies reported adequate random sequence generation. Two studies used an appropriate method of patient allocation concealment while the other 8 studies were judged at unclear risk of bias because they failed to provide details about allocation concealment. In seven of the studies included, blinding of participants and personnel was described, leaving 4 studies that did not describe despite the use of sham control, thus making it unclear whether the lack of blinding would have affected outcomes. All of the articles had published protocols, therefore, the selective outcomes reporting domain was judged at a low risk of bias (Figures 4 and 5). Information about patient allocation procedures and concealment, together with sham controls are important when evaluating data due to researcher - patient influences on outcomes. Despite this procedure not being clearly outlined in some of the included articles, the majority of those reporting outcomes from NMES in the management of COPD discuss this in depth, allowing for reliability of results as well as repeatability of the intervention.
Discussion
This review outlines the effects of NMFS in conjunction with physiotherapy, demonstrating favourable improvements in quadriceps strength, endurance and HRQoL among patients experiencing moderate to severe COPD exacerbations. Previous systemic reviews have primarily focused on investigating the impact of NMES on various outcome measures, including quadriceps maximal voluntary contraction (QMVC), the endurance shuttle walk test (ESWT), work-rate cycling endurance test (CWRT), anthropometric measures, fat-free mass (FFM), one-leg standing balance, electronically braked cycle ergometer, quadriceps twitch tension (TwQ), Biodex, Bioelectrical impedance analysis, lung function test and spirometry, 1-minute sit-to-stand, 6MWT, muscle biopsy, rectus femoris ultrasonography, SGRQ, EQ-5D, HAD Score, COPM, the Borg dyspnoea scale and the Medical Research Council or the Modified Medical Research Council. As a result of the small number of studies, limited sample size, difference in NMES treatment and parameters used and methodological approaches used, and unclear risk of bias, potential improvements reported should be carefully rellected upon.
Improvements in quadriceps strength have been attributed to the additional stimulation of the quadriceps muscles, leading to changes in muscle tissue morphology, such as a shi towards type-1 muscle fibers. This was observed through various assessments, including ultrasonography, biodex, bioelec trical impedance analysis, and thigh circumference measurements. Studies consistently reported significant improvements in quadriceps strength across different NMES parameters and frequencies, suggesting its efficacy in mitigating muscle atrophy during an AECOPD (Abdellaouui et al., [13] [p< 0.001], Chaplin et al., [16] [p< 0.04], Zanotti et al., [17] [p≤0.001], Sillen et al., [18] [p< 0.01], Maddocks et al., [5] [p=0.028], López- López et al., [19] [p< 0.001] and Péran et al., [20] [p< 0.001]).
Studies also demonstrated improvements in other outcome measures, such as endurance, balance, and overall HRQoL. NMES was associated with significant enhancements in the 6MWT, the 1MSTS, ESWT and endurance. These improvements are particularly significant given the observed decline in quadriceps strength and endurance among patients with moderate to severe COPD with an exacerbation, which can further limit mobility and decrease overall functional capacity.
The integration of NMES with other physiotherapy modalities, primarily chest physiotherapy or Pulmonary Rehabilitation, yielded better outcomes compared to control groups. By increasing both quadriceps strength and endurance, NMES interventions facilitated improvements in functional capacity and HRQoL without exacerbating breathlessness. Moreover, NMES was well tolerated with no reported adverse reactions, further supporting its safety and feasibility in the management of AECOPD [5,11,13,16,18]
Limitations of ReviewDespite these promising findings, limitations in the reviewed studies, such as small sample populations, strict inclusion criteria, and limited observational periods, warrant cautious interpretation of the results. Additionally, challenges in maintaining inter-rater reliability and blinding of personnel may have introduced bias in outcome assessments. Future research should address these limitations and explore the optimal use of NMES interventions in AECOPD management through large-scale trials.
Conclusion
In conclusion, this review provides compelling evidence for the beneficial effects of NMES in patients with acute exacerbations of COPD. Integration of NMES into comprehensive management strategies holds promise for improving quadriceps strength, endurance and HRQoL. Despite recommendations for high-frequency NMES, which showed better outcomes in the literature, further research to explore the optimal parameters is required. Varying more than one parameter might produce a likelihood that the intervention may wrongly appear to be benficial irrespective of which parameters were used. Larger sample sizes should be used to obtain more reliable results. Investigation of patient perspectives and acceptability of this intervention would also be recommended for future research in order to evaluate the holistic outcome from this intervention.
Key points- NMES demonstrates favourable improvements in quadriceps strength during acute exacerbations of COPD.
- NMES contributes to enhanced endurance and functional capacity when integrated into pulmonary rehabilitation programmes.
- NMES interventions are associated with improvements in overall HRQoL following AECOPD.
- NMES is well tolerated and produces no adverse reactions in patients with COPD
- Future research should explore the optimal parameters and effects of NMES interventions through larger-scale trials.
Funding
This research did not receive a specific grant from any public, commercial, or not-for-profit agency.
Contributions
All authors were involved in the literature search and review process, manuscript preparation and review of all dra and final version of this paper.
Conflict of Interest
The authors report no conflict of interest.
References
- Gosker HR, Zeegers MP, Wouters EFM, Schols AMWJ (2007) Muscle fibre type shifting in the vastus lateralis of patients with COPD is associated with disease severity: A systematic review and meta-analysis BMJ.
- De Brandt J, Spruit MA, Derave W, Hansen D, Vanfleteren LEGW et al. (2016) Changes in structural and metabolic muscle characteristics following exercise-based interventions in patients with COPD: A systematic review Informa UK Limited.
- De Brandt J, Spruit MA, Hansen D, Franssen FM, Derave W, Sillen MJ et al. (2017). Changes in lower limb muscle function and muscle mass following exercise-based interventions in patients with chronic obstructive pulmonary disease: A review of the English-language literature SAGE Publications.
- Mathur S, Dechman G, Bui K, Camp PG, Saey D (2019) Evaluation of limb muscle strength and function in people with chronic obstructive pulmonary disease Ovid Technologies (Wolters Kluwer Health).
- Maddocks M, Nolan CM, Man NC, Polkey MI, Hart N et al. (2015) Neuromuscular electrical stimulation to improve exercise capacity in patients with severe COPD: A randomised double-blind, placebo-controlled trial Elsevier BV.
- Aliverti A, Macklem PT Aliverti et al. (2020) - THE MAJOR LIMITATION TO EXERCISE PERFORMANCE IN COPD IS LOWER LIMB MUSCLE DYSFUNCTION
- Gea J, Pascual S, Casadevall C, Orozco-Levi M, Barreiro E Gea et al. (2015) - muscle dysfunction in chronic obstructive pulmonary disease- update on causes and biological findings.
- Nuhr MJ, Pette D, Berger R, Quittan M, Crevenna R, Huelsman M et al. (2014) Beneficial effects of chronic low-frequency stimulation of thigh muscles in patients with advanced chronic heart failure Oxford University Press (OUP)
- Neder JA, Sword D, Ward SA, Mackay E, Cochrane LM et al. (2002) Home-based neuromuscular electrical stimulation as a new rehabilitative strategy for severely disabled patients with chronic obstructive pulmonary disease (COPD) BMJ.
- Vieira PJC, Güntzel Chiappa AM, Cipriano G, Umpierre D, Arena R (2014) Neuromuscular electrical stimulation improves clinical and physiological function in COPD patients Elsevier BV.
- Giavedoni S, Deans A, Mccaughey P, Drost E, Macnee W (2012) Neuromuscular electrical stimulation prevents muscle function deterioration in exacerbated COPD: A pilot study Elsevier BV.
- Hill K, Cavalheri V, Mathur S, Roig M, Janaudis-Ferreira T et al. (2018) Neuromuscular electrostimulation for adults with chronic obstructive pulmonary disease Wiley.
- Abdellaoui A, Prefaut C, Gouzi F, Couillard A, CoisyQuivy M, et al. (2011) Skeletal muscle effects of electrostimulation after COPD exacerbation: A pilot study European Respiratory Society (ERS).
- Kucio C, Niesporek J, Kucio E, Narloch D, Węgrzyn B (2016) Evaluation of the effects of neuromuscular electrical stimulation of the lower limbs combined with pulmonary rehabilitation on exercise tolerance in patients with chronic obstructive pulmonary disease Walter de Gruyter GmbH.
- Singh J (2013) Critical appraisal skills programme SAGE Publications.
- Chaplin EJL, Houchen L, Greening NJ, Harvey-Dunstan T, Morgan MD, et al. (2019) Neuromuscular stimulation of quadriceps in patients hospitalised during an exacerbation of COPD: A comparison of low (35 hz) and high (50 hz) frequencies Wiley
- Zanotti E, Bizzarri C, Grasso R (2012) Combination of pulmonary rehabilitation and neuromuscular electrical stimulation in COPD patients: A randomized clinical trial of efficacy OMICS Publishing Group.
- Sillen MJH, Franssen FME, Delbressine JML, Vaes AW, Wouters EFM, et al. (2014) Efficacy of lower-limb muscle training modalities in severely dyspnoeic individuals with COPD and quadriceps muscle weakness: Results from the DICES trial BMJ.
- López-López L, Calvache-Mateo A, Rodríguez-Torres J, Granados-Santiago M, Ortiz-Rubio A, Valenza MC (2021) A feasibility and efficacy randomized controlled trial of two exercise programs in severe AECOPD patients with resting hypoxemia MDPI AG
- Péran L, Beaumont M, Le Ber C, Le Mevel P, Berriet AC, Nowak E, et al. (2022) Effect of neuromuscular electrical stimulation on exercise capacity in patients with severe chronic obstructive pulmonary disease: A randomised controlled trial SAGE Publications.
Article Information
Research Article
Received Date: April 21, 2024
Accepted Date: May 21, 2024
Published Date: May 24, 2024
Journal of Pulmonary Research and Therapeutics
Volume 2 | Issue 1
Citation
Randall Debattista, Anabel Sciriha, Tonio. P. Agius (2024) Effect of NMES on Quadriceps Strength and Endurance in Chronic Obstructive Pulmonary Disease Patients: A Narrative Review. J Pulm Res and the 2: 1-14
Copyright
©2024 Anabel Sciriha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jaar.2024.2.101