

Research Article
Volume-2 Issue-1, 2022
Check laparoscopy following the vaginal hysterectomy by electrosurgery in cases with known or suspected extrauterine pelvic pathology
Received Date: December 29, 2021
Accepted Date: January 31, 2022
Published Date: February 28, 2022
Journal Information
Abstract
Objective: This study demonstrates a short check laparoscopy (CL) following the vaginal hysterectomy (VH) in cases with known or suspected extrauterine pelvic pathology to detect and treat if any remnant pathology to fulfill the requirements of laparoscopy. VH is the least invasive and should be the preferred method of the hysterectomy. The vaginal hysterectomy may not be sufficient to surgically treat the high-level extrauterine pelvic pathologies in candidates with known or suspected extrauterine pelvic pathology.
Design: A prospective observational study was conducted on 169 cases from January 2019 through March 2020.
Participants/Materials, Setting, Methods: The study was conducted in a private setup. Consecutive candidates of the hysterectomy for benign indications with known or suspected extrauterine pelvic pathology such as chronic pelvic pain, dysmenorrhea, pelvic inflammatory diseases, previous pelvic surgeries, broad ligament fibroids, and adnexal diseases were recruited from January 2019 and to March 2020 for the study. Cases with uterine size above 16 weeks, associated ventrofixed uteri following previous CS, and associated prolapse uteri were excluded. Elected cases were allowed to undergo the below described CL following VH using electrosurgery. Preoperative,intraoperative and postoperative data were recorded and analyzed using descriptive statistics: percentage, mean, standard deviation, and 95% Confidence interval(CI). The primary outcome of interest was to detect the remnant pathology following VH in these elected cases. Secondary outcomes of interest were laparoscopic operation time, and risk of CL following VH.
Results: The check laparoscopy detected and surgically treated the vaginally unreached remnant extrauterine pelvic pathologies in 17.75% of cases. VH with additional surgeries was sufficient to surgically treat the vaginally reached extrauterine pathologies in the rest 82.24% cases. The mean laparoscopic operation time was 12.08±5.18(5-30) minutes (95% CI=11.29-12.87). The mean VH operation time was 75.81 ± 27.21(35-190) minutes (95% CI=71.99-79.95). The majority of vaginal work up to the level of adnexa and the minority of laparoscopic work above the level of adnexa minimised the laparoscopic time and minimised the risk of visceral injuries. There were no major perioperative complications.
Limitations: It requires a comparative study to compare the present VH plus CL with LAVH to access the benefit of the present approach.
Conclusions A check laparoscopy following VH assists to find and treat the vaginally unreached high-up remnant pathologies in cases with known or suspected extrauterine pelvic pathology. Without CL,remnant pathologies will be retained in some of these patients. The CL assists a vaginal surgeon to complete the laparoscopic surgical requirements in these patients in a short laparoscopic operation time. Thus, VH plus CL was done in place of the direct laparoscopic hysterectomy in these cases. As a whole, a patient gets the benefit of least invasive VH by electrosurgery, and of less risky laparoscopy in this strategy. A comparative study of the present VH plus CL with LAVH in the future can ascertain the better clinical practice of the present approach.
Key words
Vaginal hysterectomy; extrauterine pelvic pathology; check laparoscopy; remnant pelvic pathology; safe umbilical trocar insertion
Introduction
The vaginal hysterectomy (VH) is the least invasive method for the benign uterus without prolapse and should be the preferred route of the hysterectomy[1,2].However, suspicion of the remnant additional pathologies following VH arises in cases with known or suspected extrauterine pelvic pathology such as chronic pelvic pain, dysmenorrhea, pelvic inflammatory diseases, previous pelvic surgeries, broad ligament fibroids, and adnexal diseases [3].
Despite the advances in vaginal hysterectomy techniques, the extrauterine pathologies high-up in the upper part, anterolateral wall of the pelvis, and anterior to bladder remain unreached vaginally and are suspected to be left behind without surgical treatment in these cases [3,4]. This small portion of high- up pathology following VH, needs a laparoscopy to fulfill the surgical treatment of the patient [5].
Therefore, to fulfill the surgical requirements of the patient, we planned a check laparoscopy following the vaginal hysterectomy with a goal to find and treat surgically, if any the remnant extrauterine upper pelvic pathology in cases with known or suspected extrauterine pelvic pathologies such as chronic pelvic pain, dysmenorrhea, pelvic inflammatory diseases, previous pelvic surgeries, broad ligament fibroids, and adnexal diseases, and studied the outcomes
Material and Methods
A prospective observational study was carried out in our private setup at Purohit General Hospital.It was started in January 2019 and ended in March 2020.
Consecutive candidates of the hysterectomy for benign indications associated with known or suspected extrauterine pelvic pathology such as chronic pelvic pain, dysmenorrhea, pelvic inflammatory diseases, previous pelvic surgeries, broad ligament fibroids, and adnexal diseases were recruited.
Cases with uterine size above 16 weeks, associated ventrofixed uteri following previous CS[6], and associated prolapse uteri were excluded from the study. The selected candidates were allowed to undergo the intervention of check laparoscopy following the vaginal hysterectomy by electrosurgery. Each elected candidate signed the informed consent before entering the study. Purohit General Hospital Ethics Committee approved the study before the inclusion of the first case. Preoperative patients’ clinical characteristics, intraoperative and postoperative data were recorded during the study period.
Data were analysed using descriptive statistics: percentage, mean, standard deviation and 95% CI. Primary outcome of interest was to detect cases with remnant pathologies after VH in these elected cases. Secondary outcomes of interest were laparoscopic operation time and risk of check laparoscopy following VH from perioperative complications.
Operation procedure Vaginal hysterectomy with concurrent proceduresThe hysterectomy was performed by the Purohit technique of the vaginal hysterectomy [7], and its supplementary techniques using 22cm long bipolar forceps or a short (18 cm) bipolar cutter/shear. Supplementary procedures such as the posteroanterior approach in all cases with previous caesarean sections [6,8] to dissect uterovesical adhesions to avoid bladder injury, the anteroposterior approach in cases with the obliterated posterior cul-de-sac to dissect recto-uterine adhesions to avoid rectum injury [9] were used. Following the vaginal hysterectomy, the adhered adnexa, if any to the pelvic sidewall was mobilized down towards the surgeon by the technique of transvaginal mobilization of adhered adnexa from the lateral wall using tactile feel [10] before an attempt of salpingo-oophorectomy, and the visible adhesion if any was lysed between prongs of rightangle forceps[10]. Indicated ovarian cystectomy was performed to preserve an ovary [9]. Opportunistic salpingectomy or indicated salpingo-oophorectomy was done. The anterior wall of the rectum,pararectal space,uterosacrals,and rectovaginal space were thoroughly inspected using Deaver retractors, and occasionally fibre optic light source to find any visible pathology(9), and treated appropriately surgically,Rectovaginal space, uterosacrals and posterior vaginal wall were palpated by fingers to find any nodule in cases with the obliterated posterior cul-de-sac and excised under vision using bipolar haemostasis [9].Visible endometriotic spots were coagulated[9].Bladder and rectal integrity was checked in cases with previous CS and pelvic adhesions. Then, the check laparoscopy was performed.
Check laparoscopy following the vaginal hysterectomyBefore going for CL, the distal end of a Ryle’s tube (keeping all holes above the vault) was placed in-situ on the right side of the pelvis, and the vaginal vault was closed horizontally by two Alli’s forceps, one on each side of the Ryle’s tube.
Carbon dioxide gas was passed through the Ryle’s tube to create pneumoperitoneum to avoid transabdominal Veres’s needle insertion. Then, a primary intra-umbilical trocar was inserted to perform the laparoscopy.
The intraabdominal pressure was maintained at 8 — 10mm for check laparoscopy and 12 — 14 mm of Hg for operative laparoscopy procedures. In CL, blood clots, if any were aspirated through the suction cannula. Bleeder if any was coagulated. Remnant pelvic adhesion if any was lysed (Figure 1). Endometriotic spot if any was coagulated. Remnant endometriotic nodules, broad ligament fibroid, and adnexal pathologies if any were excised. The excised specimens were removed through the vaginal vault. A laparoscopic bipolar sealer-shearer or cutter was used for laparoscopic procedures. Laparoscopic lavage was done. Then, the laparoscopy was concluded and the vault was closed.
Primary abdominal port insertion under transvaginal endoscopic guidanceIt was done in cases with a long previous anterior abdominal wall incision extending up to the umbilicus and multiple previous pelvic surgeries. In the place of the Ryle’s tube, a 10mm telescope with cannula was inserted, and the abdomen was inflated with CO2 gas through the side channel. In Trendelenburg position, the anterior abdominal wall was inspected intraperitoneally to locate adhesion -free the safe site for insertion of transumbilical or supraumbilical trocar under vision to avoid visceral injury.
Patients were followed up for 6 weeks after the operation
Factors affecting breastfeeding practice
Total 169 candidates with known or suspected extrauterine pelvic pathology underwent CL following VH during the study period. The mean age of cases was 43 ± 4.47(35-51) years.
Table 1 shows the preoperative clinical characteristics and vaginal procedures performed. Of 169 cases, 47(27.81%) chronic pelvic pain, 84(49.70%) dysmenorrhea, 2 (1.18%) previous pelvic laparotomy, 59(34.91%) adenomyosis uterus,15 (8.87%) pelvic endometriosis, 9(5.32%) pelvic inflammatory diseases,21 (12.42%) adnexal cysts ,5(2.95%) hydrosalpinx underwent CL following VH. Among them, 48(28.40%) cases had history of previous 1-3 caesarean sections, and 49 (28.99%) cases had large fibroid uterus of 12- 16 weeks of gestation. Some cases had more than one clinical characteristic. None of the cases had ureteric obstruction or gut obstruction.
They received the following different concurrent operative procedures used during the vaginal hysterectomy: posteroanterior approach in 48(28.40%) cases with history of previous CS, anteroposterior approach in 11(6.50%) cases with the obliterated posterior cul-de-sac, transvaginal mobilization of adhered adnexa from the lateral pelvic wall, and vaginal adhesiolysis in 24(14.20%) cases, ovarian cystectomy in two(1.18%) cases, salpingo-oophorectomy in 28(16.56%) cases.
Primary abdominal port insertion under transvaginal endoscopic guidance was done in two (1.18%) casesTable 2 shows different types of remnant pathology detected during CL, and laparoscopic procedures required
Remnant pathologies were found in only 17.75%. In the rest 82.24% of cases, the vaginal hysterectomy and concurrent procedures were sufficient to treat the extrauterine pathologies thus; no remnant pathology was found. High-up remnant pathologies such as adhesions of the sigmoid colon to the lateral pelvic wall, of upper part of the rectum to the appendix, of the sigmoid to the bladder and intestine, of omentum to the lateral pelvic wall, round ligament, iliac fossa and bladder, of adnexa to broad ligament above upper pole of the ovary, of omentum to anterior abdominal wall scar following previous CS were detected during the check laparoscopy. In addition, endometriotic spots on the ovary and pelvic wall, endometriotic nodules on the lateral pelvic wall, and small broad ligament fibroid (1cm) were found during CL. The majority of remnant pathologies were located above the level of upper pedicle stumps and adnexa and were unreached vaginally.
The remnant pathologies were seen in 50% of cases with a history of previous pelvic surgery, in 44.44% of cases with chronic pelvic inflammatory disease, in 37.5 % of cases with previous CS, in 26.66 of cases with pelvic endometriosis, in 13.55% cases of with adenomyosis uterus and in 5.26% of cases with fibroid uterus. Thus, all hysterectomy candidates associated with pelvic pain were suspected cases for extrauterine pathologies and needed a laparoscopic survey. The following different laparoscopic procedures were performed during the check laparoscopy. 82.24% of cases did not require any laparoscopic procedure following the VH and concurrent procedures. In them, a check laparoscopy without or with lavage was sufficient. Only, 17.75% required operative laparoscopic procedures. The majority of operative procedures was adhesiolysis of the omentum in the upper wider part of the pelvis and did not need a high skill surgery. Few had adhesiolysis of organ-to-organ adhesions. Excision of the endometriotic nodule of the lateral pelvic wall and broad ligament fibroid was done in four 4(2.36%) cases, and the excised specimens were removed through the vaginal vault. Incidentally, oozing of blood from an upper pedicle stump was seen in one (0.59%) case and needed laparoscopic coagulation. Endometriotic spots were coagulated in three (1.77%) cases. None of the cases required laparoscopic adnexectomy after concurrent vaginal procedures.
Table 3 shows perioperative outcomes of CL following VH.
88.16% of cases needed only 2 ports, and 11.83% of cases needed 3 laparoscopic ports to complete CL. Laparoscopic sealer-shear with simultaneous coagulation and cut facility helped reduction of the eded for laparoscopic adhesiolysis. Low intraabdominal pressure of 8-10 mm of Hg was sufficient in 82.24% of cases. Standard intraabdominal pressure of 12-14 mm was needed in operative laparoscopy in 17.75% of cases. The stumps produced by a vaginal procedure using the bipolar cutter/shear, and that after laparoscopic procedures by bipolar sealer-shear appeared physically similar.
Mean laparoscopic operation (CL) time was 12.08 ± 5.18(5- 30) minutes (95% CI=11.29-12.87). The CL time increased with an increasing amount of laparoscopic surgery.
Mean VH time was 75.81 ± 27.21(35-190) minutes (95% CI=71.99-79.95).
Mean VH time was 75.81 ± 27.21(35-190) minutes (95% CI=71.99-79.95).
None of the cases had failed VH or failed planned adnexectomy. None of the cases needed conversion to laparotomy. None of the cases had intraoperative organ injury during the vaginal hysterectomy or during the CL. Majority of vaginal work up to the level of adnexa and the minority of laparoscopic work above the level of adnexa reduced risk of laparoscopic injuries to organs. No postoperative fistula was seen. Two cases had vault seromas and required ultrasound-guided vaginal aspiration. Two cases had vault infection in the 2nd postoperative week, one case had incomplete vault dehiscence in the 4th week, all healed with conservative management.
Discussion
Using the described techniques (Table 1), vaginal hysterectomy had been done successfully by the set of skilled surgeons in all cases. The vaginally reached extrauterine pathologies were surgically treated in of 82.24% cases. However, the operating surgeons fell short of reaching the upper pelvic extrauterine pathologies vaginally in of 17.75% cases, therefore, took the assistance of laparoscopy to reach and surgically treat precisely, these pathologies after the vaginal hysterectomy in this study. Thus, the novel check laparoscopy fulfilled the diagnostic and simplified the therapeutic purpose of utilisation of laparoscopy in hysterectomy, and avoided the conventional laparoscopic hysterectomy in all cases in this study. A laparoscopic-assisted vaginal hysterectomy (LAVH) is a vaginal hysterectomy that is assisted by laparoscopy[11] .In the LAVH (laparo-vaginal strategy),extrauterine pathologies are surgically treated before the start of hysterectomy. In the present method, in a reverse style (vagino-laparoscopic strategy), the remnant extrauterine pathologies were surgically treated after finishing the vaginal hysterectomy [9] during check laparoscopy.In the vagino-laparoscopic strategy, most of the extrauterine pathologies were treated surgically during vaginal hysterectomy including indicated adnexectomy. Thus,the check laparoscopy in this study had not found remnant pathology (Table 2) in 82.24% of cases and ended with a diagnostic laparoscopy similar to that of stage-0 of LAVH. The rest 17.75% of cases required a short laparoscopic procedure for the remnant pathologies, similar to that of stage 1 of the staging system/classification for the laparoscopic hysterectomy [11], and completed the laparoscopic surgery of the patient. There was no need of pre-hysterectomy laparoscopy similar to stage -0 or stage -1 of LAVH, rather, a direct CL after VH was sufficient in the present approach. None of these cases required a conventional laparoscopic hysterectomy (LAVH/TLH) in this approach
The present approach has the benefit of a short mean laparoscopic exposure (CL) time of 12.08 ± 5.18(5-30) minutes (Table 3) similar to that of diagnostic laparoscopy. It is far less than what is required for a laparoscopic hysterectomy. This is a result of less quantity of laparoscopic work left after a vaginal hysterectomy. Thus, the mean operation time of combined CL plus VH by electrosurgery is far less than that of a laparoscopic hysterectomy in our previous study for the benign condition of the uterus following previous CS [6] (88.34 ± 29.94 vs 149.71 ± 38.6min), as well as that of a recent randomized control trial study [12] (88.34 ± 29.94 vs 126 ± 42.7 min). Therefore,the short check laparoscopy was sufficient to address the retained pathologies after the vaginal hysterectomy in this study.
The primary port insertion through the anterior abdominal wall under the novel transvaginal endoscopic guidance following VH in cases with multiple previous abdominal wall scars in this study, helped the surgeon to find adhesion free site in two (1.18%) cases with suspected severe anterior abdominal adhesions. The pneumoperitoneum created using a Ryle’s tube inserted through the vaginal vault avoided Veres’s needle insertion. Thus, these were helpful to avoid the risk of incidental primary trocar injury of the viscera in cases with multiple previous pelvic operations, and long anterior abdominal wall incisions.
In addition, most of CL was completed with two abdominal ports. Laparoscopic surgery in the narrow lower part of the pelvis during the laparoscopic hysterectomy requires standard intraperitoneal pressure to expose the anatomy. In CL, most of the laparoscopic procedures were required in the wider upper part of the pelvis than the narrower lower part , thus, accomplished at low intraabdominal pressure (Table 3). The present CL, therefore, is expected to reduce the postoperative abdominal wall and shoulder pain, similar to findings of the previous study [13]. It was easy to perform CL by our averagely skilled laparoscopic surgeons who were able to perform a VH in this study. Thus, VH plus CL was done in place of the direct laparoscopic hysterectomy in this study. As a whole, a patient gets the benefit of least invasive VH, and of minimally invasive laparoscopy in this strategy.
Conclusion
A check laparoscopy following the vaginal hysterectomy can be performed to find and surgically treat the vaginally unreached remnant upper pelvic pathologies in cases with a known or suspected extrauterine pelvic pathology. It completes the surgical requirements of the patient and minimises the laparoscopic operation time. A comparative study of the present VH plus CL with LAVH in the future can ascertain the better clinical practice of the present approach.
Contribution to authorship
All authors qualified for the authorship.
Disclosure of interests
All authors have nothing disclosure of the interest to declare.
Funding
No external funding was received for the study.
Acknowledgement
The authors would like to thank Vijay Babar for the statistical assistance in the planning of the study.
References
- Aarts JW, Nieboer TE, Johnson N. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2015;2015(8)
- Lee, S.H, Oh, S.R., Cho, Y.J. Comparison of vaginal hysterectomy and laparoscopic hysterectomy: a systematic review and meta-analysis. BMC Women's Health. 2019:19, 83.
- Garry R, Fountain J, Mason S, et al.The eVALuate study: two parallel randomised trials, one comparing laparoscopic with abdominal hysterectomy, the other comparing laparoscopic with vaginal hysterectomy.BMJ.2004: 328:129–38.
- Sizzi O, Paparella P, Bonito C. Laparoscopic Assistance After Vaginal Hysterectomy and Unsuccessful Access to the Ovaries or Failed Uterine Mobilization: Changing Trends.JSLS. 2004; 8(4): 339–346
- Kovac SR.Vaginal hysterectomy.In:Rock JA,Jones HW,eds. Telinde’s Operative Gynaecology. 10th ed; Philadelphia: Lippinvott Williams and Wilkins; 2008:744-45
- Purohit R, Sharma JG, Meher D, Rakh SR, Choudhary M. A laparovaginal strategy to avoid bladder injury during laparoscopic-assisted vaginal hysterectomy in cases with ventrofixed uterus following previous cesarean section. Int J Womens Health. 2018;10:579-587.
- Purohit RK. Purohit technique of vaginal hysterectomy: a new approach. BJOG. 2003;110(12):1115–1119.
- Purohit R, Sharma JG, Singh S, Giri DK. Vaginal Hysterectomy by Electrosurgery for Benign Indications Associated with Previous Cesarean Section. J Gynecol Surg. 2013;29(1):7–12
- Purohit R, Sharma J, Meher D, Rakh SR, Malik S. Completion of vaginal hysterectomy by electro surgery using anteroposterior approach in benign cases faced with obliterated posterior cul-desac. Int J Womens Health. 2018;10:529-536
- Purohit R, Joshi S, Sharma JG.Adnexectomy During Vaginal Hysterectomy for Benign Indications Using Bipolar Hemostasis of Lateral Pedicles and Transvaginal Adnexa Mobilization.J GYNECOL SURG 31(2):86-91
- Fred M.Howard.Laparoscopic hysterectomy.In:Rock JA,Jones HW,eds. Telinde’s Operative Gynaecology. 10th ed; Philadelphia: Lippinvott Williams and Wilkins; 2008:763-65
- Allam IS, Makled AK, Gomaa IA. Total laparoscopic hysterectomy, vaginal hysterectomy and total abdominal hysterectomy using electrosurgical bipolar vessel sealing technique: a randomized controlled trial. Arch Gynecol Obstet. 2015;291(6):1341- 1345.
- J C Radosa, M P Radosa, P A Schweitzer. Impact of different Intraoperative CO 2 pressure levels (8 and 15 mmHg) during laparoscopic hysterectomy performed due to benign uterine pathologies on postoperative pain and arterial pCO2 : A prospective randomised controlled clinical trial. BJOG. 2019 ;126(10):1276-1285
|
N=169 |
% |
Characteristics |
47 48
5 169 48
11
24
2
2 |
|
Chronic pelvic pain |
|
|
Dysmenorrhea |
27.81 |
|
|
49.70 |
|
Previous Caesarean section |
|
|
1cs |
28.40 |
|
2cs |
8.87 |
|
3cs |
14.79 |
|
Previous pelvic laparotomy |
4.73 |
|
Uterus size of 12 -16 weeks |
1.18 |
|
Fibroid uterus |
28.99 |
|
Adenomyosis uterus |
44.97 |
|
Pelvic Endometriosis |
34.91 |
|
Pelvic inflammatory disease |
8.87 |
|
Adnexal cyst (including largest size |
5.32 |
|
-9.2cm,3 twisted adnexal cysts) |
12.42 |
|
Hydrosalpinx |
|
|
Vaginal procedures performed |
2.95 |
|
VH with or without debulking |
|
|
|
100 |
|
Posteroanterior approach in cases |
|
|
with previous CS |
|
|
|
28.40 |
|
Anteroposterior approach in cases |
|
|
with obliterated posterior cul-de- |
|
|
sac |
6.50 |
|
Transvaginal mobilization of |
|
|
adhered adnexa and vaginal |
14.20 |
|
adhesiolysis |
|
|
Ovarian cystectomy |
|
|
Salpingo-oophorectomy |
1.18 |
|
|
16.56 |
|
Primary abdominal port insertion |
|
|
under transvaginal endoscopic |
1.18 |
|
guidance |
|
Remnant pathologies |
N=169 |
% |
Remnant pathology not found |
139 |
82.24 |
Remnant pathology detected |
30 |
17.75 |
Adhesions found |
|
|
-of sigmoid colon to lateral pelvic wall |
4 |
2.36 |
-of rectum to appendix |
|
|
-of sigmoid to bladder to intestine |
1 |
0.59 |
-of omentum to lateral pelvic wall, |
1 |
0.59 |
roundligament, iliacfossa, bladder |
10 |
5.91 |
-of adnexa to broad ligament above upper |
2 |
1.18 |
pole of ovary |
|
|
-of omentum to anterior abdominal wall scar |
6 |
3.55 |
following previous cs |
|
|
Endometriotic spots on ovary and pelvic wall |
3 |
1.77 |
Endometriotic nodules lateral pelvic wall |
|
|
Broad ligament fibroid(1cm) |
2 |
1.18 |
Laparoscopic procedures performed |
|
|
Operative laparoscopy needed |
2 |
1.8 |
Check laparoscopy with or without lavage |
30 |
17.75 |
Adhesiolysis |
139 |
82.24 |
- of omentum from lateral pelvic wall, |
10 |
5.91 |
iliacfossa, roundligament, bladder |
|
|
-lysis of sigmoid colon from lateral pelvic |
4 |
2.36 |
wall |
|
|
-lysis of sigmoid from bladder |
1 |
0.59 |
-lysis of rectum from appendix |
1 |
0.59 |
-lysis of intestine from sigmoid |
1 |
0.59 |
-adhered adnexa mobilised |
2 |
1.18 |
Coagulation of endometriotic spots |
3 |
1.77 |
Excision of endometriotic |
2 |
1.18 |
nodule of lateral wall |
|
|
Excision of small broad ligament fibroid |
2 |
1.18 |
Coagulation of tiny oozing from right upper |
1 |
0.59 |
pedicle stump |
|
|
Laparoscopic Adnexectomy |
0 |
0.00 |
Vaginal removal of specimen |
4 |
2.36 |
Outcomes |
N=169 |
% |
Three Laparoscopic ports needed Two laparoscopic ports needed Intraabdominal pressure 8-10mm
Mean specimen uterus weight
Mean 24 hours Hb fall Blood transfusion Mean Hospital stay Postoperative complications Fever |
20
139 178.25±107.19(40-620) Gm 0.69±0.37(0.1-1.9) Gm%. (95% CI=0.64-0.76)
0 0
3 0 |
11.83 82.24
0.59
0 0 1.77 0 |
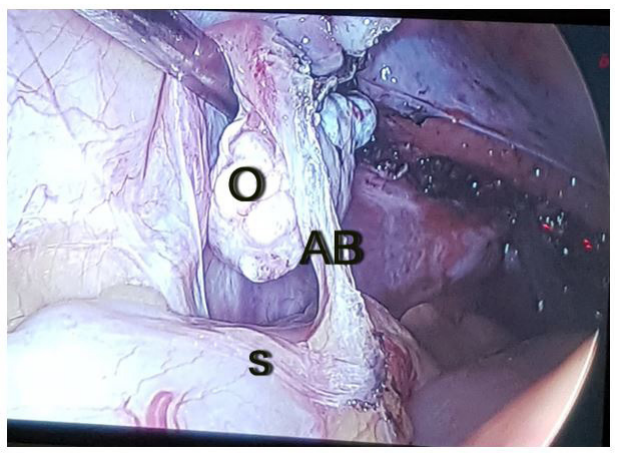 |
| Figure 1: Shows a remnant adhesion band (AB) between the left ovary(O) and the sigmoid colon(S) following VH, and was detected during PHCL |
Artcle Information
Research Article
Received Date: December 29, 2021
Accepted Date: January 31, 2022
Published Date: February 28, 2022
Journal of Women Health Care and Reproductive Medicine
Volume 2 | Issue 1
Citation
Ramkrishna Purohit (2022) Check laparoscopy following the vaginal hysterectomy by electrosurgery in cases with known or suspected extrauterine pelvic pathology J Women Health Care Reprod Med 2: 1-12
Copyright
©2022 Ramkrishna Purohit. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jwrm.2022.2.104