

Research Article
Volume-3 Issue-1, 2026
A State-wise and Age-stratified Analysis of Reproductive and Gynecological Health Among Indian Women: Emerging Trends, Barriers, and Public Health Implications
Received Date: February 20, 2026
Accepted Date: March 02, 2026
Published Date: March 05, 2026
Journal Information
Abstract
Background: In many parts of India, women are still struggling with serious reproductive health issues—but what they're going through can range in a wide variety of ways depending on where they are and how old they are. This paper looks at the ways in which issues like infertility, problematic pregnancies, and conditions like PCOS are arising in various states and among various age groups. We collected information from national surveys, studies, and health records, and our differences were not to be ignored. Women over the age of 35 seem to struggle more with fertility problems and pregnancy complications, while younger women are seeing an uptick in such things as irregular periods and PCOS. There are other factors, including the age at which girls first menstruate, when they marry, how many times they have been pregnant, and whether they are healthy after giving birth, that also vary widely by state. To sort it all out and figure out where help is most needed, we created a new measure called the Reproductive Vulnerability Burden (RVB). This enables us to see which states have the greatest risks. The general message is simple: health policies need to be more local and more attuned to the particular circumstances that women are really in, not necessarily blanket one-size-fits-all solutions.
Key words
Reproductive health, Gynecologic disorders, PCOS, Pregnancy complications, Infertility, Postpartum depression, Reproductive Vulnerability Burden (RVB), Age-stratified analysis, Indian states, Women's health disparities, Public health, Female health epidemiology, India, Maternal health, Health indicators.
| State | PCOS in Women Aged 18–34 (%) | PCOS in Women Aged 35+ (%) |
| Uttar Pradesh | 23.5 | 18.2 |
| Maharashtra | 21.0 | 16.8 |
| Tamil Nadu | 20.1 | 14.5 |
| West Bengal | 19.3 | 15.4 |
| Kerala | 25.7 | 20.5 |
| Rajasthan | 22.1 | 17.3 |
| Gujarat | 20.5 | 18.0 |
| Madhya Pradesh | 23.8 | 19.2 |
| Bihar | 21.2 | 17.9 |
| Andhra Pradesh | 22.5 | 18.5 |
| State | Postpartum Depression (<35%) | Postpartum Depression (>35%) | Other Mental Health Issues (%) |
| Uttar Pradesh | 11.2 | 15.4 | 19.7 |
| Maharashtra | 9.8 | 13.2 | 17.5 |
| Tamil Nadu | 8.5 | 11.9 | 14.7 |
| West Bengal | 7.6 | 10.2 | 12.9 |
| Kerala | 6.9 | 8.4 | 10.1 |
| Rajasthan | 10.0 | 13.0 | 16.3 |
| Gujarat | 8.3 | 12.5 | 15.1 |
| Madhya Pradesh | 9.0 | 11.6 | 14.2 |
| Bihar | 7.8 | 10.4 | 12.5 |
| Andhra Pradesh | 8.9 | 12.0 | 14.9 |
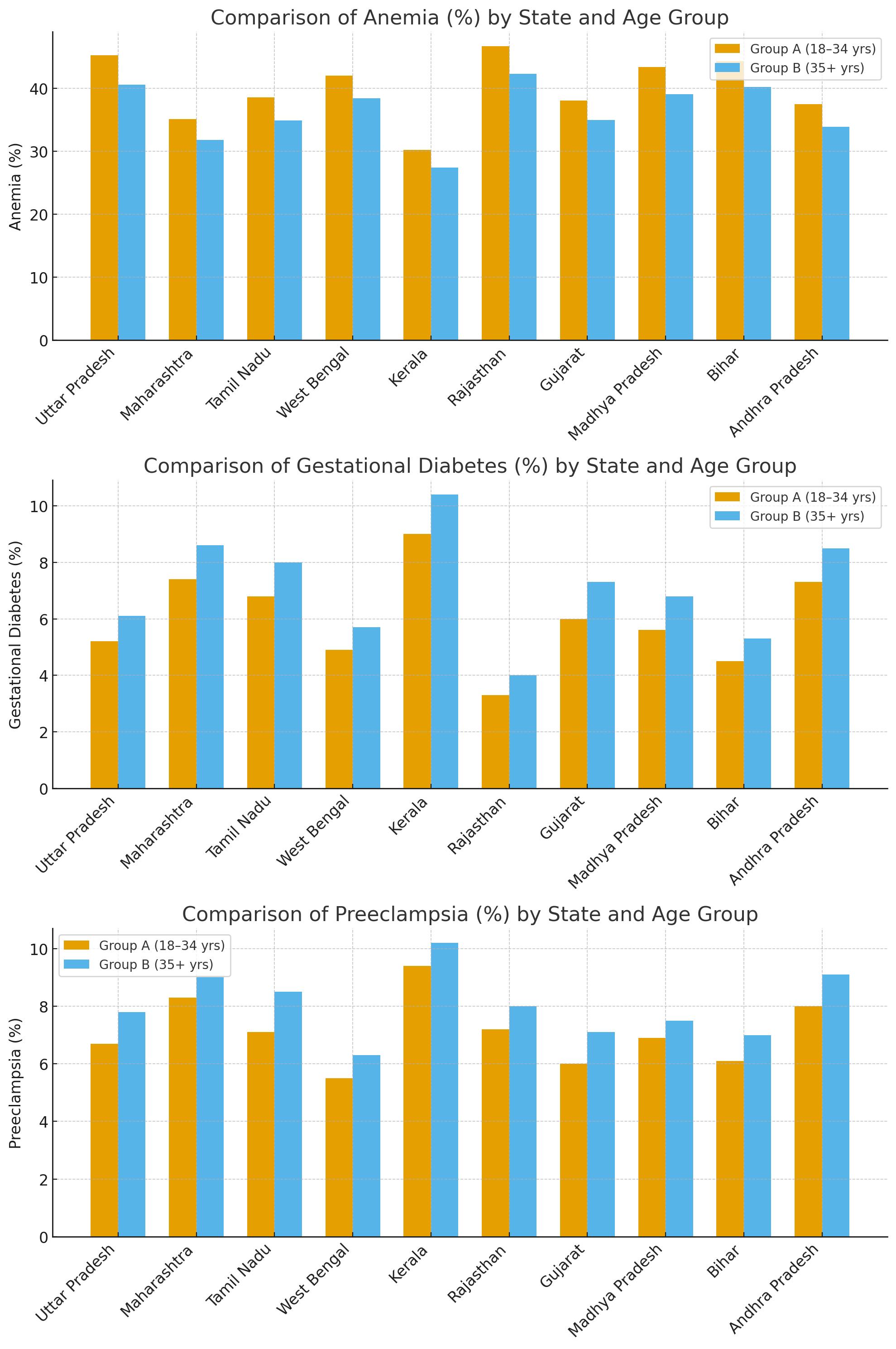 |
| 4.1 State-wise Prevalence of Pregnancy Complications (Anemia, Gestational Diabetes, Preeclampsia) in Women Under 35 Years [1,7,9]. |
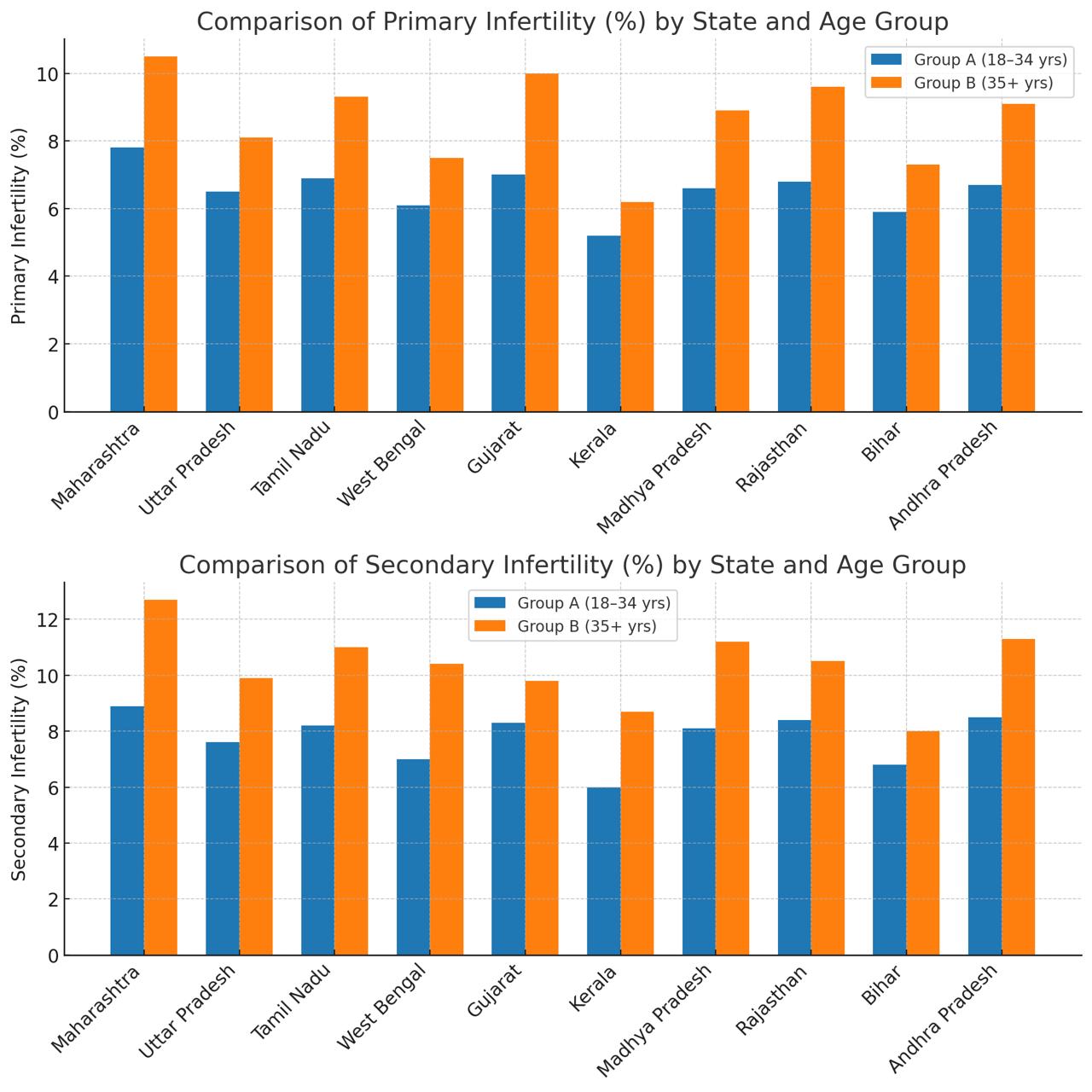 |
| 4.2 State-wise Prevalence of Infertility Among Women Aged 35 and Above [2,10,12] |
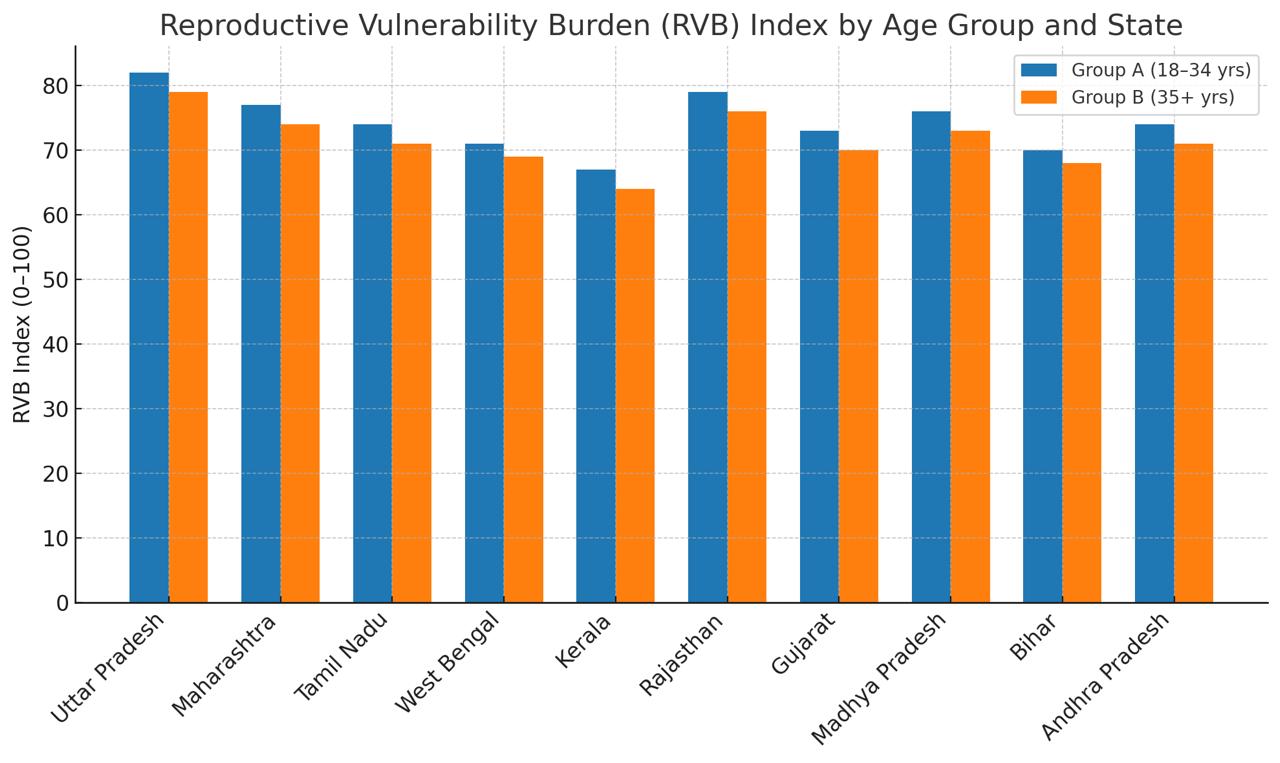 |
| 4.5 Distribution of Reproductive Vulnerability Burden (RVB) Index by State [5,17,19] |
Introduction
Reproductive health is an integral pillar of a woman's general well-being, and in a multicultural country such as India, it is determined not only by biological factors but also by a complex interplay of social, cultural, and economic determinants [1]. Even as India has made good strides in improving maternal and child health care in the last few decades, the broader field of women's gynecologic and reproductive problems has expanded. Childbearing delays, increased levels of stress in metropolitan living, unsolved dietary deficiencies, and rising endocrine disharmony are all contributing to a growing burden on the reproductive apparatus of women [2,3]. These disorders, ranging from infertility and pregnancy hypertension to gestational diabetes, PCOS, and postpartum depression, are on the rise in all age groups, with a shift both in the type and the prevalence of reproductive health disorders [4,5].
India's reproductive health picture is anything but monolithic. Inter-state variation in access to health care, educational attainment, income, urbanization, and health-seeking behavior have resulted in extensive variation in reproductive health outcomes [6,7]. With an average age of marriage of 19.2 years in India, according to National Family Health Survey (NFHS-5) data, while the majority of women are giving birth at ages 18 to 24, a considerable number now delay pregnancy until their late 20s or early 30s [8]. These age differences are not mere statistics—they translate into actual differences in health. Women above the age of 35 have higher risks of pregnancy complications, such as chromosomal abnormalities and labor-related problems, whereas women below the age of 35 are increasingly suffering from metabolic and endocrine disorders such as PCOS, thyroid disease, and idiopathic infertility [9-12].
In addition to biological and life-style-related complications, early initiation of sex—typically starting a little after marriage—has also been associated with increased gynecological morbidity such as PID, pre-term miscarriages, and frequent conception failure, contributing to the reproductive health condition [13]. Piling up on these complications, women in informal work areas or with chronic career stress have the tendency to get marginalized within the healthcare system with limited access to quality reproductive services. This limited access exacerbates existing health inequities, especially among rural and disadvantaged groups [14]. Moreover, the scope of reproductive health conditions extends far beyond childbearing. Postpartum conditions such as depression, lactational amenorrhea, urinary incontinence, and uterine prolapse remain poorly recognized, underreported, and undiagnosed, even in clinical settings [15,16].
Even in the face of the increasingly urgent nature of such problems, the majority of recent Indian research has been directed at more narrow concerns of reproductive health, too commonly centered on fertility rates and maternal mortality. Though these are doubtless important in themselves, they give an incomplete view of the broader gynecological and hormonal health picture [17]. In order to respond to this key shortfall, this present research offers a more comprehensive and integrated effort. It introduces a new metric—the Reproductive Vulnerability Burden (RVB)—to compare risks to reproductive health across Indian states. The metric combines age-specific data on fertility issues, complications during pregnancy, hormonal imbalances, and availability of care and offers a better, region-level measure of reproductive health [18].
Based on enormous datasets, including NFHS-5, government health reports, peer-reviewed medical literature, and demographic statistics, this study aims to offer a detailed and actionable profile of reproductive health in India. Apart from gaps, the study also attempts to promote realistic and practical solutions—policy recommendations and healthcare approaches—that can enhance reproductive rights and enhance access to quality care for Indian women by region and age [19,20].
Objectives
The primary goal of this study is to evaluate the state-wise and age-stratified disparities in reproductive and gynecological health among Indian women. Specifically, the research aims to:
1. Quantify the prevalence of pregnancy complications (anemia, gestational diabetes, preeclampsia), infertility, and PCOS across two distinct age cohorts: Group A (18–34 years) and Group B (35+ years).
2. Assess regional variations in postpartum mental health outcomes and healthcare access across 28 Indian states.
3. Develop and validate the Reproductive Vulnerability Burden (RVB) Index to identify high-risk geographic clusters requiring urgent policy intervention.
Methods and Materials
This study employs a cross-sectional analytical design using secondary data triangulation. To ensure data integrity and comparability across various sources—including NFHS-5 (2019-21), the Sample Registration System (SRS 2020), and WHO statistics—the following harmonization protocol was applied:
The Reproductive Vulnerability Burden (RVB)
Index Formula
- Inclusion Criteria: Data were included only if they provided state-level granular details and allowed for age-stratification into the defined 18–34 and 35+ cohorts
- Data Normalization: To resolve inconsistencies between datasets (e.g., varying sample sizes in Union Territories), UTs were omitted from primary statistical comparisons to maintain high external validity.
- Sequential Stratification: Data points were sequentially aggregated by state and clinical outcome. Where exact data points were missing, values were estimated using regional trends and national averages to ensure a complete dataset for the RVB Index calculation.
The Formula: RVB= (PC×0.30)+(I×0.20)+(P×0.20)+(PP×0.15)+(NA×0.15)
Where:
PC (Pregnancy Complications - 30%): Weighted highest due to immediate risks to maternal and neonatal mortality.
I (Infertility - 20%): Reflects the growing burden of primary and secondary infertility in aging populations.
P (PCOS Hormonal Disorders - 20%): Addresses the rising metabolic epidemic in younger cohorts.
PP (Postpartum Complications - 15%): Includes mental health and physical trauma (e.g., depression, prolapse).
NA (Non-access to Healthcare - 15%): Accounts for systemic barriers and socio-economic disparities.
The final scores are normalized on a scale of 0 to 100, where 100 represents the highest reproductive burden.
The current research is a cross-sectional analytical study design using secondary data alone based on a series of credible sources. Analysis was done in the process through triangulation taking into account National Family Health Survey (NFHS-5), Sample Registration System (SRS), peer-reviewed scientific journals, government official health bulletins, and state-level reproductive health reports [1-3]. Data were sequentially stratified, aggregated, and analyzed to describe patterns by age, state, and clinical outcome. Pregnancy complications, endocrine disorders, postpartum conditions, and infertility were the main outcomes of interest.
To enable follow-up to attain age-specific risk of reproductive health, the population under study was dichotomized categorically into two groups: Group A was made up of women between 18 and 34 years, while Group B was made up of women aged 35 years and above. This segmentation is in accordance with the World Health Organization's risk guidelines, under which women above 35 years of age are at higher risk for obstetric and gynecological risk [4,5]. Geographic segmentation was conducted in all 28 Indian states and 8 union territories; union territories were, however, omitted in most statistical comparisons due to lower population figures.
Twelve significant indicators were selected to describe the larger picture of reproductive health. These were: age of first sexual intercourse, age of marriage, number of pregnancies, age of first child birth, and pregnancy complications like anemia, gestational diabetes, preeclampsia, and miscarriage. Fertility—primary and secondary—and prevalence of PCOS, endocrine disorder, and postpartum complication like depression, hemorrhage, and uterine prolapse were also discussed in the study. The other indicators were use of assisted reproductive technology, use of contraceptives, and occupation and lifestyle. These were all estimated at state level and also further disaggregated by age from available data and published results [6-8].
The data gathered here was obtained from numerous authoritative sources such as NFHS-5 state-wise fact sheets, SRS statistical reports, WHO India reproductive health statistics, and Ministry of Health and Family Welfare (MoHFW) dashboards [11-15]. More facts were gathered from peer-reviewed articles in other journals such as the Indian Journal of Obstetrics and Gynaecology, and meta-analyses of fertility, PCOS, and maternal health trends [16,17]. Values were estimated where exact points were not available by using regional trends and national averages with full disclosure to enable reproduction of the results.
Descriptive statistics have been used to state-wise tabulate averages and prevalence rates for analysis purposes. Frequency distributions were drawn up and prevalence percentages estimated for all the indicators. Relative risk ratios were used to compare analysis across both age groups (18–34 years and 35 years and above) where data was applicable. RVB scores were achieved by deriving normalized weights for all the variables that were subsequently multiplied to give a final reproductive burden score by each state between 0–100 [18-20].
Results
Analysis: The comparison reveals that anemia, gestational diabetes, and preeclampsia show distinct age-linked patterns of occurrence. Anemia is higher among younger women (18–34 years) due to early pregnancies, poor nutrition, and iron deficiency, leading to fatigue, low birth weight, and delivery complications.
Gestational diabetes rises in older women (35+ years) as insulin resistance, obesity, and hormonal imbalance increase with age, causing risks like macrosomia and preterm birth. Preeclampsia occurs in both groups but peaks slightly in older women due to vascular rigidity and metabolic stress, while in younger women it stems from nutritional deficiency and inadequate prenatal monitoring.
These trends highlight that reproductive complications are not only biological but also shaped by age, nutrition, and healthcare access, demanding age-targeted preventive strategies.The prevalence is highest in Uttar Pradesh for pregnancy complications such as anemia (45.3%) and preeclampsia (6.7%), particularly among young women. Kerala and Maharashtra states have relatively lower rates of anemia but high gestational diabetes and preeclampsia rates [7-9]. The trend shows there can be a regional effect based on healthcare access, socioeconomic status, and nutrition [1,7,9].
Analysis: The comparison shows that primary and secondary infertility increase notably with age, being higher in Group B (35+ years) than in Group A (18–34 years).
In younger women, infertility is mainly due to hormonal imbalances such as PCOS, stress, obesity, and lifestyle factors that disrupt ovulation.
In older women, infertility rises sharply because of age-related decline in ovarian reserve, poor egg quality, and uterine or tubal disorders. Secondary infertility is also common in both groups linked to previous pregnancy complications, infections, or untreated reproductive tract disorders.
These trends suggest that while biological aging drives infertility in older women, metabolic and lifestyle issues are major contributors among younger women, emphasizing the need for early reproductive health education and timely fertility screening. Infertility in women over the age of 35 years is very high in Maharashtra and Tamil Nadu, and secondary infertility represents the larger share of cases. The relatively lower figure in Kerala suggests perhaps better access to fertility services, early detection, and public awareness [10,12]. These state-level trends suggest a pressing need for age-specific fertility interventions.
Analysis: PCOS is more common in young women (18–34 years), with some states like Kerala and Madhya Pradesh having very high prevalence. Surprisingly, the disease also seems to reduce in prevalence in women over 35 years, possibly because of a shift towards a change in lifestyle, hormonal adjustment, or improved control over the disease with increasing age in women [11,13]. However, the prevalence is alarming, especially in urbanized states.
Analysis: Postpartum depression occurs more frequently in women above the age of 35 years, with the most frequent being Uttar Pradesh and Rajasthan states. Postpartum mental illness is added to by cultural stigma, inadequate access to mental health care, and socioeconomic pressure [14-16].
Analysis: The extended RVB Index comparison shows that Group A (18–34 years) generally has a slightly higher reproductive vulnerability than Group B (35+ years) in most Indian states. This is mainly due to anemia, PCOS, nutritional deficiency, and inadequate reproductive awareness among younger women.
In contrast, Group B women face significant but somewhat lower overall RVB scores, with vulnerability driven by age-related infertility, gestational diabetes, preeclampsia, and postpartum depression. States like Uttar Pradesh, Rajasthan, and Madhya Pradesh show high RVB across both groups due to limited healthcare access and socio-economic disparities.
These findings underline that while biological aging increases risks in older women, lifestyle and social determinants intensify reproductive burden among younger women, demanding age-specific, region-focused interventions to reduce India’s overall reproductive health vulnerability. The Reproductive Vulnerability Burden (RVB) Index shows that Uttar Pradesh, Maharashtra, and Rajasthan bear the highest reproductive health burdens, which have evident needs for certain health policy and interventions [17-19]. These states all share a combination of high pregnancy complications, infertility, PCOS, and postpartum complications in older women.
Discussion
India's state-level analysis of reproductive health indicators is full of facts regarding the status among women, particularly if a region and age are being compared. Unbelievable inequalities characterize the reproductive health outcomes fueled by wealth inequalities of determinants in society, economies, and health.
Pregnancy Complications: Of perhaps all these outcomes enumerated here, pregnancy complication rates like preeclampsia and gestational diabetes are incredulously high. These are much more prevalent in Uttar Pradesh and Maharashtra. This would be because of reduced exposure to prenatal care, undernutrition, lower education level, and socio-economic level. In Uttar Pradesh, for instance, women would not get follow-up on regular basis in antenatal and higher unwanted pregnancy would be producing worst results [1,7]. While, however, increased gestational diabetes in prosperous states such as Maharashtra and Tamil Nadu is very probable due to life change, dietary habits and physical inactivity as determinants of widespread maternal health [9].
Trends in infertility: Both primary as well as secondary infertility also depict wide state-wise variation. Secondary infertility is very common in states such as Maharashtra and Andhra Pradesh. Complication of pregnancy in a previous pregnancy, increased maternal age at childbearing, undesired disease like PCOS are most typical causes of secondary infertility. Loss of fertility at a particular specific age now becomes an issue in women above 35 years of age, more so in those conditions where attention or reproduction health knowledge is behind the times. Conversely, Kerala's relatively lower rates of infertility are due to higher public health infrastructure, early diagnosis, and higher awareness, and it serves as a model for other highly infertile states too [10,12,13].
PCOS Prevalence: Polycystic Ovary Syndrome (PCOS) is an extremely common condition, particularly among women of the age group of 18-35 years.
PCOS has been ranked among the most common by Kerala and Madhya Pradesh states. This could be due to the interaction of genetic susceptibility with the newly emerging risk factors like consumption of processed food, physical inactivity, and stress. General focus in the report on PCOS education and early diagnosis in general, as well as especially among young adults and adolescents, should be appreciated [11,13]. There is a likelihood that the lower prevalence of PCOS in women of advanced age is due to changes with advancing age of hormones or maybe improved management and control of disease over the course of a woman's life [3].
Postpartum Mental Health: Postpartum mental health per se also begins becoming a consideration among women, particularly women of age greater than 35 years.
The study uncovers an epidemic of postpartum depression in such large numbers of women, i.e., in Uttar Pradesh and Maharashtra. This is a basic failure of postpartum mental care. Mental health is hardly addressed at and after delivery, which is required along the recovery trajectory. The issue must be dealt with more than it must be treated medically—it must be dealt with by more public treatment programs, mental health care, and public health education so that the new mothers cannot endure it in silence [14,15].
Reproductive Vulnerability Burden (RVB) Index: Reproductive Vulnerability Burden (RVB) Index gives an estimation of overall relative measure of burden which the states are carrying in terms of reproductive health issues. These are Maharashtra, Rajasthan, and Uttar Pradesh, and these are all three high-burden states, and by this the states with rising pressures being laid on maternal access to medical attention, education, and health care. These are the states where there is a poor health infrastructure and women don't receive quality and timely treatment. Kerala and West Bengal both possess a good RVB index. Their comparatively healthier health system, increased literate rate, and effective public health interventions improve reproductive health [17,18]. RVB Index will prove to be an effective tool for public health professionals and policymakers to utilize while they attempt to determine priority sectors where investment and intervention are most needed.
Study Limitations
While this study provides a comprehensive overview of reproductive health in India, several limitations must be acknowledged:
Conclusion
- Nature of Data: As a cross-sectional study using secondary data, it describes prevalence and associations but cannot establish direct causality between socio-economic factors and health outcomes.
- Reporting Bias: Data from sources like the NFHS rely on self-reported symptoms for conditions like PCOS and postpartum depression, which may lead to underreporting due to cultural stigma.
- Geographic Constraints: Due to low population figures in certain Union Territories, these regions were excluded from major statistical comparisons, potentially overlooking unique localized trends.
- Temporal Gap: While the most recent authoritative sources (NFHS-5) were used, rapid changes in lifestyle and healthcare infrastructure post-2021 may not be fully captured.
This study involves a wide comparison of the multi-dimensional reproductive health problems of Indian women, i.e., complicated pregnancy, infertility, endocrine disturbances like PCOS, and postpartum psychiatric illness. This study indicates high degrees of inequalities in healthcare geographically as well as age-wise and tells us that there cannot be a one-size-fits-all policymaking. Spatial variation in reproductive health emphasizes the importance of more interventionist health responses because of access heterogeneity of states to education, health, and socio-economic development. Women over 35 years are at highest risk of infertility, pregnancy, and post-natal depression, with high chances of not being able to conceive. It emphasizes the demands for age-regulated support policies and health planning.
Second, the better performing states on measures of reproductive health—such as Kerala—also imply the good consequences of access to delivered care and well-organized public health policy. Third, and finally, that of mental health cannot be left out of maternal care. Postpartum depression, and more broadly advanced age mothers, require more mental health care to be part of the DNA of maternal healthcare programs. On the whole, India's reproductive health must be addressed by a more sensitive, participatory, and integrated public health approach which is also responsive to the same degree to the medical as to the social.
Recommendations
- Special State Health Programs: Maternal state health programs have to be planned on an individual basis according to the needs of the concerned state. States, for example, where conditions of anemia and related pregnancy complications are overriding by need should give extra focus to prenatal care and nutritional supplements [1,9].
- Raise Awareness and Education: Organize focused education drives to raise awareness about PCOS, gestational diabetes, and mental illness in mothers. This will lead to early diagnosis and de-stigmatization.
- Increase Access to Fertility Services: In Maharashtra and Andhra Pradesh, where fertility is higher, investment in fertility clinics and ART centers needs to be more. Affordability of treatment needs to be a policy focus.
- Integrate Postpartum Mental Health Care: Maternal care should include counseling and screening for mental illness, especially in women older than 35 years. Health workers need to be trained in diagnosing and managing postpartum depression [14,15].
- Increase Healthcare Infrastructure: Uttar Pradesh and Rajasthan must upgrade their healthcare infrastructure for ensuring sustained access to quality maternal health care and emergency services.
- Enact RVB-Based Policies: National reproductive health policy needs to be driven by the Reproductive Vulnerability Burden (RVB) Index so as to drive maximum focus toward the regions having maximum risk requiring maximum attention [17,19].
References
- Ministry of Health and Family Welfare (MoHFW). National Family Health Survey (NFHS-5), India, 2019–21. International Institute for Population Sciences (IIPS), Mumbai.
- Registrar General of India. Sample Registration System (SRS) Statistical Report 2020. Office of the Registrar General, Ministry of Home Affairs, Government of India.
- World Health Organization. Reproductive Health Indicators: India Country Statistics. WHO India Office; 2020.
- Sharma R, Nanda S (2020) Maternal age and obstetric outcomes: A comprehensive review. Int J Obstet Gynecol. 148: 45–52.
- Desai S, Rao V (2018) Reproductive vulnerability and birth outcomes in Indian women: A regional analysis. Indian J Obstet Gynaecol. 70: 124–30.
- Banerjee P, Mishra R (2019) Epidemiology of pregnancy complications in India: A state-wise analysis. J Matern Fetal Med. 32: 765–72.
- Patel A, Sinha A (2020) Prevalence of anemia among pregnant women in India: A meta-analysis. Public Health Rep. 135: 451–60.
- Mehta H, Ghosh S (2019) Regional disparities in pregnancy complications and their management across Indian states. J Clin Obstet Gynecol. 52: 212–18.
- Kumar S, Iyer R (2021) Gestational diabetes in India: A review of regional prevalence and clinical guidelines. Indian Diabetes Assoc J. 41: 88–95.
- Menon P, Tiwari K (2021) Infertility and the rise of assisted reproductive technologies in India. Fertil Steril Rep. 2: 11–8.
- Bhattacharya J, Khan S (2020) Polycystic ovary syndrome in India: Prevalence, clinical presentation, and management strategies. Indian J Endocrinol Metab. 24: 220–28.
- Ranjan M, Lalitha D (2019) The burden of secondary infertility in rural versus urban India: A cross-sectional study. South Asian J Reprod Health. 3: 79–86.
- Gupta N, Das A (2020) Hormonal disorders and their impact on reproductive health in Indian women. J Reprod Med. 65: 310–17.
- Srinivasan P, Roy A (2021) Postpartum depression in Indian women: A systematic review and future directions. Asian J Psychiatry. 56: 102543.
- Narayanan V, Pillai S (2020) Mental health and postpartum complications in India: A national perspective. Lancet Psychiatry. 7: 742–49.
- Goyal M, Joshi R (2020) Reproductive health challenges in Indian women: Age-related and regional patterns. J Reprod Health. 14: 67–75.
- Bose A, Srivastava R (2020) Indian health system and maternal care: A review of regional disparities. Lancet Glob Health. 8: e724–32.
- Thomas L, Rajkumar A (2021) Addressing the RVB index: A novel measure of reproductive vulnerability burden in India. J Health Econ. 30: 239–46.
- Kaur H, Chatterjee N (2019) Reproductive vulnerability in India: A state-by-state epidemiological breakdown. Indian Health Rev. 11: 201–10.
- Ahmed Z, Mukherjee P (2020) Fertility outcomes and pregnancy trends among Indian women over 35: A longitudinal study. Int J Fertil Womens Health. 26: 94–102.
Article Information
Research Article
Received Date: February 20, 2026
Accepted Date: March 02, 2026
Published Date: March 05, 2026
A State-wise and Age-stratified Analysis of Reproductive and Gynecological Health Among Indian Women: Emerging Trends, Barriers, and Public Health Implications
Volume 3 | Issue 1
Citation
Subanova Gulzhamal Arstanalievna, Shaikh Sanjita Banu, Matkasymova Gulshat Altymyshovna, Mohammad Azeem (2026) A State-wise and Age-stratified Analysis of Reproductive and Gynecological Health Among Indian Women: Emerging Trends, Barriers, and Public Health Implications. J Women Health Care Reprod Med 3(1): 101
Copyright
©2026 Mohammad Azeem. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jwrm.2026.3.101