

Case Report
Volume-1 Issue-2, 2025
A Case Report on Partial HELLP Syndrome in Lagos, Nigeria
Received Date: August 03, 2025
Accepted Date: August 21, 2025
Published Date: August 28, 2025
Journal Information
Abstract
Background: HELLP syndrome is a complication of the spectrum of hypertensive disorders of pregnancy [1]. It is an acronym which refers to the triad of Haemolysis, Elevated Liver enzymes and a Low Platelet count [1]. It may represent a complication or progression of severe preeclampsia; however, this relationship has been challenged by evidence that preceding hypertension or proteinuria is absent in about 15 to 20% of patients with HELLP syndrome [2].
Case presentation: A 23yrs old unbooked G2P0+1 presented at the Lagos state University Teaching Hospital (LASUTH) at an estimated gestational age of 32 weeks and 4 days with complaints of elevated blood pressure that was first noticed 4 days prior to presentation. She also complained of Headache and Drowsiness which were noticed 4 days prior to presentation at our facility. There was history of decreased urination and decreased maternal perception of fetal movements in the last 24 hours. Examination revealed that the patient was conscious but drowsy with pallor,febrile, bilateral pitting pedal edema, tachycardia, tachypnea, absent fetal heart sounds, palpable contractions and a 2cm dilated cervix. Investigation findings revealed anemia, deranged liver enzymes, Low platelets, elevated urea and creatinine. She was managed as a case of a case of Partial HELLP syndrome complicated with Acute kidney injury and Intrauterine fetal death with a septic focus. She received 5 units of whole blood, 5 units of platelet concentrates, had 1 session of haemodialysis and was discharged on the 10th day of admission after clinical condition improved.
Key words
Partial HELLP Syndrome, Acute Kidney Injury, Preeclampsia, Liver Enzymes, Platelets
| DAY 1 | DAY 2 | DAY 3 | DAY 4 | DAY 5 | DAY 7 | DAY 9 | |
| ELECTROLYTES, UREA & CREATININE | |||||||
| Sodium/mmol/l(135-145) | 136 | 141 | 143 | 136 | 140 | 141 | 140 |
| Pottasium/mmol/l(3.5-5.5) | 4.4 | 3.9 | 4.3 | 3.5 | 3.6 | 3.6 | 4 |
| Chloride/mmol/l(98-110) | 107 | 112 | 111 | 105 | 92 | 96 | 100 |
| Bicarbonate/mmol/l(22-30) | 13 | 20 | 19 | 23 | 18 | 16 | 17 |
| Urea/mmol/l(2.5-6.4) | 20 | 33.3 | 37.7 | 18.4 | 13.9 | 5.24 | 3.97 |
| Creatinine/micromol/l(53-115) | 378 | 464 | 430 | 158 | 123 | 65 | 52 |
| eGFR/ml/min/1.73m2(>90) | 16 | 13 | 14 | 46 | 62 | 90 | 90 |
| FULL BLOOD COUNT | |||||||
| PCV/%(35-48) | 29.6 | 26.4 | 18.1 | 24.7 | 24.7 | 26 | 30.8 |
| Hb/12.0-16(g/dl) | 9.7 | 8.5 | 6 | 8.4 | 8.6 | 8.7 | 10.2 |
| WBC/cc/mm3(4,000-11,000) | 11800 | 21500 | 24200 | 26300 | 33370 | 29360 | 16930 |
| NEUTROPHILS/% | 74.7 | 63.9 | 12 | 65.8 | 68.1 | 73.2 | 66.7 |
| LYMPHOCYTES/% | 21.7 | 28.5 | 12 | 24 | 7.32 | 5.25 | 22.8 |
| Platelets/cc/mm3(150,000-450,000 | 17000 | 21000 | 24000 | 41000 | 66000 | 239000 | 473000 |
| LIVER FUNCTION TEST | |||||||
| AST /U/L) (10-42) | 76 | ||||||
| ALT (U/L) (10-40) | 27 | ||||||
| TOTAL BILIRUBIN (mcmol/l) (2-20) | 17.6 | ||||||
| CONJUGATED BILIRUBIN (mcmol/l) (0-3.4) | 7.2 | ||||||
| CLOTTING PROFILE | |||||||
| PROTHROMBIN TIME/Secs(11.5-14.5) | 11.9 | ||||||
| INR (0.8-1.2) | 0.84 | ||||||
| PTT/Secs(26.5-40) | 37.3 | ||||||
| PERIPHERAL BLOOD FILM | |||||||
| Normochromic normocytic red cells with few nucleated red cells seen. | |||||||
| White blood cells were slightly increased on film with a predominance of mature neutrophils and a left shift up to the and stage lymphocytes seen appear mature. | |||||||
| Platelets were also reduced on the film | |||||||
| LACTATE DEHYDROGENASE/U/L(<237) | 1310 |
 |
| Figure 1 |
 |
| Figure 2 |
| Source [15] |
Introduction
A 23yrs old unbooked G2P0+1 presented at the Lagos state University Teaching Hospital (LASUTH) at an estimated gestational age of 32 weeks and 4 days with complaints of elevated blood pressure that was first noticed 4 days prior to presentation. She also complained of Headache and Drowsiness which were noticed 4 days prior to presentation at our facility. There was history of decreased urination and decreased maternal perception of fetal movements in the last 24 hours.
There was no history of fainting, convulsion, blurring of vision or upper abdominal pain. There was no frothiness of urine or early morning facial puffiness.
She had no previous history of hypertension, diabetes or kidney disease. There was also no family history of the above chronic medical illnesses.
One day prior to her presentation at our facility, She presented at a private hospital where her blood pressure was noted to range between a systolic blood pressure of 158 to 173mmHg and diastolic of 113 to 122 mmHg. She was given intravenous labetalol in escalated doses totaling about 200mg and referred to our facility.
She had not booked index pregnancy at any facility up to this point. She had however had an ultrasound scan done 4 weeks prior to this point which revealed a normal live singleton fetus. Index Pregnancy was not adversely eventful until now.
Physical examination in our facility noted the patient being conscious but drowsy, Glasgow coma scale was 14/15 with confused speech. Respiratory distress was evidenced by flaring of the ala nasi and fast breathing. She was febrile (Temperature 38.1c) and moderately dehydrated. She was mildly pale with bilateral pedal edema up till distal third of the leg. She was however neither cyanosed nor jaundiced.
She had a pulse rate of 128 beats per minute, blood pressure of 139/113 mmHg, respiratory rate of 34 cycles per minute and oxygen saturation of 99% in room air. She had a uniformly enlarged abdomen, the liver was not palpably enlarged and both kidneys were not ballotable. The symphysiofundal height was 29cm judged to be small for date. There was a singleton foetus in longitudinal lie, cephalic presentation. There were 2 palpable uterine contractions in 10 minutes lasting 35 seconds each. The foetal heart sound was not present. The urine from catheter was coke coloured. Pelvic examination revealed a normal vulvovagina with a posterior cervix which was medium in consitency, 2cm long with the cervical os 2cm dilated. Fetus was vertex presenting at Station -1 with membrane intact and adhered to the presenting part.
An initial assessment of Severe preeclampsia complicated with Acute kidney injury and suspected Intrauterine fetal death in latent phase of Labour was made. The patient was counseled on the diagnosis and she consented for admission. She had blood investigations (Full blood count, packed cell volume, urea, electrolytes with creatinine, liver function tests and clotting profile), grouping and crossmatching of 2 units of blood. Bed side clotting time was 4 minutes and urinalysis revealed protein of 2+. She had an abdominal ultrasound which revealed intrauterine fetal death with foetus in cephalic presentation, normal fundal placenta with estimated foetal weight of 1.9kg at an average gestational age of 31 weeks and 6 days. She was resuscitated with intranasal oxygen and had Intravenous Magnesium sulphate according to the Zuspan regimen. Plans were made to administer intravenous labetalol in escalator doses if blood pressure was equal or greater than 160/110mmHg. She was also placed on oral antihypertensives (Nifedipine and Labetalol). Intravenous fluid was restricted to 2L/ day.
Other admitting investigations revealed anaemia(Hemoglobin concentration 9.7g/dl), thrombocytopenia(Platelet count 17,000 cc/mm3), azotemia and an abnormal liver function test. A further assessment of Partial HELLP syndrome complicated with Acute kidney injury, suspected Intrauterine fetal death with septic focus in latent phase of Labour was made.
She was transferred to the labour ward when judged to be in active phase of labour. She delivered a macerated female neonate with residual weight of 2025g and placenta completely expelled. No dysmorphic feature, no evidence of cord accident.
She was managed in a multidisciplinary fashion involving the nephrologists, Intensivists and hematologists.
The nephrologists noted Acute kidney injury and reiterated the need for fluid restriction, commenced intravenous Meropenem, intravenous frusemide and intravenous paracetamol. A mean arterial blood pressure target was set at 70-80mmHg. The hematologists noted severe thrombocytopenia with AKI to rule out microangiopathic hemolytic anemia. She was transfused with 5 units of platelet concentrate. The Intensivists suggested the need for close monitoring and possible intensive care admission for optimal management. She was also placed on supplemental oxygen using non rebreathable face mask.
Her post-delivery blood pressure was 142/78mmHg. Post-delivery full blood count and electrolytes revealed severe anemia (18.1%) leukocytosis (24,00cc/mm3) thrombocytopenia and azotemia. She was transfused with 5 units of blood and had a session of hemodialysis on the 3rd day on admission. She was also noticed by the Nephrologists to be in polyuric phase of Acute Kidney injury and had intravenous fluids at 2/3rds of the previous day’s urinary output.
Full blood count and renal function tests were subsequently done daily. Blood pressure attained normal values on the 3rd day on admission.
Urea, Creatinine and platelets had attained normal values by the 6th day on admission and 3rd day post dialysis.
She was discharged on the 10th day on admission and scheduled for follow-up visits in the gynecology and nephrology clinics.
She was subsequently seen two weeks later at the postnatal and nephrology clinics and her clinical and laboratory parameters were normal.
Literature Review
HELLP syndrome is a complication of the spectrum of hypertensive disorders of pregnancy [1].
It is an acronym which refers to the triad of Haemolysis, Elevated Liver enzymes and a Low Platelet count [1].
It may represent a complication or progression of severe preeclampsia; however, this relationship has been challenged by evidence that preceding hypertension or proteinuria is absent in about 15 to 20% of patients with HELLP syndrome [2].
HELLP syndrome complicates 0.1% to 0.8% of pregnancies. 10% to 20% of HELLP occur with severe preeclampsia [1,3]. It coexists in 70–80% of cases with preeclampsia [4].
HELLP syndrome occurs mostly in the second and third trimesters of pregnancy (usually after 27 weeks of gestation), and 15–30% of women present in the puerperium (usually within 7 days after delivery) [3].
About 70% of cases occur in the third trimester of pregnancy, and the remainder occurs within 48 hours of delivery. the mortality rate of pregnant women is 3.4–24.2%, and the mortality rate of children in the perinatal period is as high as 7.7–60.0% [2,3].
Preeclampsia when severe or when associated with HELLP syndrome can lead to AKI and in the setting of HELLP syndrome alone, AKI has been reported to occur in 7–60% of patients [1].
The classification of HELLP syndrome is based on two main diagnostic definitions.
The Tennessee classification is widely used for diagnosis [4]. The Mississippi classification underlines the severity of the disorder according to the nadir of the platelet count [4].
Tennessee classification is used to diagnose HELLP syndrome and requires the presence of all three criteria [2].
1) Hemolysis confirmed with at least 2 of the findings: Peripheral smear with schistocytes and burr cells, Serum bilirubin >1.2 mg/dl, Low serum haptoglobin(<25mg/dl) or LDH> two times the upper level of the normal, serum lactate dehydrogenase > 600 IU/L [5], Severe anemia with hemoglobin <8 to 10 g/dl depending on the pregnancy stage, unrelated to blood loss.
2) Elevated liver enzymes: AST or ALT > 2 times the upper level of normal. [5] (based on laboratory-specific reference ranges). (The use of twice the upper limit of normal threshold was chosen, in part, to avoid problems related to differences in assays, which may result in an elevated absolute value in one hospital that is considered near normal in another).
3) Low platelets: <100,000 cells/microL
Class 1 and class 2 are associated with Hemolysis (LDH≥ 600 IU/L) and elevated AST or ALT (≥ 70 IU/L) levels. Platelet counts are ≤ 50,000 cells/mm3, for class 1, and ≤ 100,000 cells/mm3 for class 2, while class 3 requires LDH ≥ 600 IU/L, AST or ALT ≥ 40 IU/L, and platelet count >100,000 or ≤ 150,000/ µL [6].
Complete HELLP syndrome was defined by the presence of all of the following three laboratory criteria according to the Tennessee Classification System [5].
Partial HELLP syndrome was defined as the presence of one or two features of c-HELLP [5,6].
Patients with partial HELLP syndrome may progress to meet all criteria and hence should be monitored carefully [2]. The incidence of HELLP syndrome complicating preeclampsia is 10 to 20% while that of partial HELLP syndrome is around 21 to 24% [7,8]. A study in India in patients with preeclampsia revealed 11.33% patient had HELLP syndrome and 14.66% patient had partial HELLP syndrome [7].
Mississippi triple class system classifies HELLP syndrome based on severity as [9,10];
Class 1 is defined by the presence of micro-angiopathic haemolytic anaemia and hepatic dysfunction in addition to a maternal platelet count ≤ 50000/mm3.
Class 2 is defined by a platelet nadir > 50000 to ≤ 100000mm3
Class 3 is defined by a platelet nadir > 100000 to ≤ 150000mm3.
Complete HELLP was associated with more serious short-term adverse outcomes at index pregnancy compared to partial HELLP, yet both forms had similar long-term obstetric and medical outcomes [5].
Nevertheless, both types have similar sequelae in subsequent pregnancies and later life and, as such, both can be regarded as a continuum in the natural evolution of the same disease [5].
HELLP syndrome implies impaired placentation during the early stages of pregnancy, associated with hepatic and coagulation cascade involvement [4].
The pathophysiology of HELLP is not entirely clear but it is proposed that an ischemic-reperfusion injury triggers the systemic inflammatory process in HELLP syndrome. [2] The spiral arteries which fail to remodel because of inadequate trophoblast invasion or defective endothelial apoptosis result in ischemia of the placenta. [2] This causes activation of endothelium, which is accompanied by an increased release of antiangiogenic factors, which leads to multiorgan microvascular injury [2].
In addition, abnormal oxidation of fatty acids by the fetus and release of metabolic intermediates into the mother's circulation causes liver and vascular dysfunction. The coagulation cascade is activated by the adhesion of platelets on the activated and damaged endothelium [2].
Platelets release thromboxane A and serotonin, causing vasospasm, platelet aggregation, and further endothelial damage [2]. This causes the usage of platelets and hence, thrombocytopenia [2]. The red blood cells break down while passing through these platelet-fibrin-rich capillaries, causing microangiopathic hemolytic anemia [2]. Multiorgan microvascular injury and hepatic necrosis lead to the development of HELLP syndrome. The cascade terminates with the delivery of the fetus [2].
Schistocytes or helmet cells present on a peripheral blood smear are diagnostic of microangiopathic hemolytic anemia [2]. Hepatic histology shows fatty infiltration, intravascular fibrin deposits, neutrophilic infiltrate, sinusoidal obstruction, intrahepatic vascular congestion, hepatic necrosis, and periportal hemorrhage. [2] This may eventually result in intraparenchymal or subcapsular hemorrhage and capsular rupture.
The endothelial damage in the liver is thought to be responsible for the obstruction with red blood cells of the Disse space, an area between liver sinusoidal endothelial cells and hepatocytes [4]. This leads to an increased formation of microthrombi, ischemia of the hepatocytes, and ultimately liver failure.
Symptoms include epigastric/right upper quadrant pain (40–100%), hypertension and proteinuria (80–85%), fatigue, nausea and vomiting, sudden weight gain and headache.
Patients are usually multiparous and over the age of 35 years old. Patients usually present between 28 to 37 weeks of pregnancy (third trimester)or immediate postpartum within seven days of delivery. Associated features may include jaundice, increasing abdominal girth, leg swelling, headache, and visual changes.2 Patients may present with severe bleeding, placental abruption, acute kidney injury, liver hematoma, or retinal detachment.
Examination reveals patients with blood pressure >140/90 mmHg and may have ascites or pedal edema. Right upper quadrant or epigastric tenderness,Icterus, Visual disturbances may be present.
Complications of HELLP syndrome include; 1. Eclampsia 2. Placental abruption 3. Cesarean section 4. DIC 5. Recurrent thrombosis 6. Liver rupture/hematoma 7. Fulminant liver failure 8. Cerebral infarction 9. Cerebral hemorrhage 10. Pulmonary/cerebral edema 11. Cardiovascular instability 12. Acute kidney injury 13. Infection/sepsis 14. retinal detachment 15. severe peripartum bleeding 16. Maternal death.
Fetal complications include: 1. Perinatal death 2. Intrauterine growth restriction (IUGR) 3. Preterm birth 4. Neonatal thrombocytopenia,leukopenia,neutropenia 5. Respiratory distress syndrome.
The mortality rate of women with HELLP syndrome is 0%-24%, while the perinatal mortality rate is about 37%.
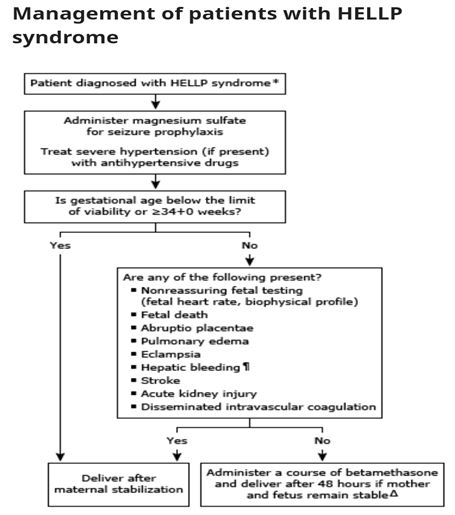
Management is multidisciplinary and is mainly supportive. The first step in managing these seriously ill patients is to stabilize them and assess fetal status with a nonstress test and ultrasound examination for a biophysical profile.
Overall, there are three main treatment options for women with severe preeclampsia and HELLP syndrome viz; 1. Immediate delivery from the 34th week of pregnancy. 2. Delivery within 48 hours after examination, clinical stabilization of the mother and caesarean section. 3. Conservative management for a waiting period greater than 48-72 hours may be considered for pregnant women less than 27 weeks gestation.
Consider patients for red cell transfusion if hemoglobin is <7gm/dl or if the patient has ecchymosis, severe hematuria, or suspected placental abruption.
All actively bleeding patients with any degree of thrombocytopenia should be transfused with platelets. Patients with coexisting DIC may need fresh frozen plasma and cryoprecipitate.
Betamethasone administration is recommended for fetal lung maturity when the patient presents at <34 weeks of gestation. Magnesium sulfate should be initiated at the time of admission to prevent maternal seizures and neuroprotective effects on the fetus/neonate.
Control/Prevention of seizures. Magnesium sulphate is the drug of choice (gold standard) for the prevention and control of seizures. As an anti-convulsant, magnesium sulphate has been found to be superior to both diazepam and phenytoin.
In acute situations, intravenous agents like hydralazine and βblockers like labetalol may be used.
Patients still have a 4–27% chance of recurrence when they become pregnant again. Therefore, early detection and provision of timely and effective interventions are particularly important.
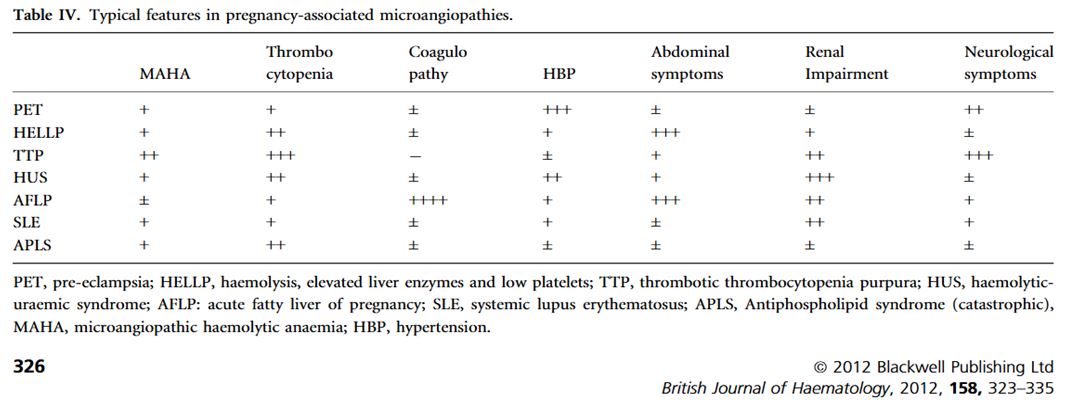
Differential Diagnosis include; Pre-eclampsia with DIC, Acute fatty liver of pregnancy, Thrombotic thrombocytopenic purpura, Pregnancy-related hemolytic-uremic syndrome, Systemic Lupus erythematosus flare-up, Antiphospholipid syndrome, Fulminant Viral hepatitis.
Discussion
We presented a case of Partial HELLP syndrome complicated with Acute kidney injury and Intrauterine fetal death with a septic focus. She was admitted into our facility and spent a total of 10 days in the hospital. She received 5 units of whole blood, 5 units of platelet concentrates and had 1 session of haemodialysis.
Symptoms of HELLP syndrome usually occur after 27 weeks of gestation [3]. A retrospective study in Iran noted 35.84±2.9 weeks as the average gestational age of subjects with Partial HELLP syndrome which is in agreement with that of our patient at 32.57 weeks. The average age of subjects with Partial HELLP syndrome in that study was 26.67±6.03 [8]. which is within the age bracket of our 23 year old patient.
Our patient presented with complaints of Elevated blood pressure, headache, drowsiness and reduced urinary output which are known symptoms and complications of HELLP syndrome. In tandem with a case reported in India our patient did not present with epigastric or right upper quadrant pain. A retrospective study at the Makassed General Hospital however found that epigastric pain occurred in 23.7% of subjects with partial HELLP syndrome in contrast with 70.8% of subjects with complete HELLP syndrome [5]. Headache however had close proportions of occurrence between both groups at 30.3% and 37.5% respectively.
Fetal death which was a feature in our patient was found to occur in 5.4% of subjects in the retrospective study at the Babol University of Medical Science but in 20% in another study. and 18.75% in another Preterm labour as seen in our patient also accounted for 50.2% of subjects in the prior study. The proportion of subjects with Partial HELLP syndrome like our patient who had blood transfusion in the study was only 3.4% however a case report in India [11] reported transfusion with blood products. A study at the Chang Gung Medical Center also noted transfusion with blood products as an appropriate management strategy. A study in Lebanon however found the use of blood products to be 10.5% in partial versus 25% in complete HELLP syndrome.
Acute renal failure as seen in our patient was also found in 23.9% of subjects with HELLP syndrome in a study and 12.5% of Partial HELLP syndrome in another study.
Our patient presented with symptoms suggestive of hemolysis, elevated liver enzymes and low platelet counts and is diagnosed with Partial HELLP syndrome according to the Tennessee classification; She was anemic (Hemoglobin concentration 9.7g/dl) and had elevated Lactate dehydrogenase (1310 ng/dl) however, serum bilirubin was 1mg/dl, and a peripheral blood smear showed no shistocytes or barbels. The liver transaminases are also less than twice the upper limit of normal which are 80 and 84U/L for ALT and AST respectively by our laboratory reference range. This brings to fore the intricacies of evaluating liver transaminase levels not by absolute values but in respect to individual laboratory reference ranges.
According to the Missisipi classification of severity, our patient falls into class 1 which accounted for 34.6% of patients with HELLP syndrome in a study in Taiwan.
Thus our patient had partial HELLP syndrome that would have progressed to full HELLP syndrome without intervention.
A study at the Institute of Postgraduate Medical Education & Research, India found similar occurrence of maternal and perinatal adverse outcomes in both complete and partial HELLP syndromes. It is thus imperative that diagnosis and intervention occur as soon as possible
Management with MgSO4 and antihypertensives as carried out in our case was the treatment of choice as reported in a case in Abdul Moeloek Hospital, Indonesia [14].
A gradual improvement of her condition was observed after hemodialysis which was similar to that obtained in Jos, Nigeria [1].
Thrombocytopenia associated microangiopathies occurs in other conditions in pregnancy creating a diagnostic dilemma. Differential diagnoses include; Thrombocytopenic purpura which would present with sensory disturbances with anemia, thrombocytopenia and renal dysfunction as observed in our patient, however, it usually occurs during the first trimester of pregnancy and occurs with normal blood pressure and no proteinuria. Antibody-associated autoimmune diseases may also present similarly, but liver function tests were normal.
The atypical presentation in this case of partial HELLP syndrome presents a diagnostic dilemma and could easily be missed with the need of a high index of suspicion.
Conflict of Interest
None
Funding
None
Ethical Approval
None
Contributions
The authors were directly involved in assessing, evaluating and administering treatment to the index patient.
References
- Anyaka CU, Pam VC, Dabu BA, Oyebode TA, Karshima JA, Pam IC, et al. (2020) Successful management of severe HELLP syndrome: A case report. Highland Medical Research Journal. 20: 56-60.
- Khalid F, Mahendraker N, Tonismae T (2020) HELLP syndrome.
- Huang H, Liu B, Gao X, Wang Y (2022) Clinical classification, pregnancy outcomes and risk factors analysis of severe preeclampsia complicated with HELLP syndrome. Frontiers in Surgery. 9: 859180.
- Petca A, Miron BC, Pacu I, Dumitrașcu MC, Mehedințu C, Șandru F, et al. (2022) HELLP syndrome—holistic insight into pathophysiology. Medicina. 58: 326.
- Ramadan MK, Malas A, El-Tal R, Itani SE, Rabah H, Badr DA (2021) Appraisal of short-and long-term outcomes of partial versus complete HELLP syndromes: A retrospective cohort study. Journal of Fetal Medicine. 8: 185-92.
- Rare but critical Obstetric; A Case study HELLP Syndrome: A rare but critical Obstetric Conundrum.
- Durugkar K, Bal H, Agrawal S (2017) A study of maternal and perinatal outcome in cases of HELLP and partial HELLP syndrome. Int J Reprod Contracept Obstet Gynecol. 6: 5491-6.
- Bouzari Z, Firoozabadi S, Hasannasab B, Emamimeybodi S, Golsorkhtabar-Amiri M (2013) Maternal and neonatal outcomes in HELLP syndrome, partial HELLP syndrome and severe pre-eclampsia: Eleven years experience of an obstetric center in the north of Iran. World Applied Sciences Journal. 26: 1459-63.
- Makinde O, Ife MCB, Omoniyi A. IFEMED. survival.4: 5.
- Paul BS, Juneja SK, Paul G, Gupta S (2013) Spectrum of neurological complications in HELLP syndrome. Neurology India. 61: 467-71.
- Dagar S, Gupta M, Shekhawat V, Minhas S (2021) Partial HELLP syndrome: case report. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 10: 4570-3.
- Rakshit A, Lahiri S, Biswas SC, Dey R, Roy BR, Saha MM (2014) A study to detect HELLP syndrome and partial HELLP syndrome among preeclamptic mothers and their impact on fetomaternal outcome. Al Ameen J Med Sci. 7: 20-5.
- Liu CM, Chang SD, Cheng PJ, Chao AS (2006) Comparisons of maternal and perinatal outcomes in Taiwanese women with complete and partial HELLP syndrome and women with severe pre‐eclampsia without HELLP. Journal of Obstetrics and Gynaecology Research. 32: 550-8.
- Wahyunindita RN, Sari RDP (2022) Severe Pre-Eclampsia with Partial Hellp Syndrome in Multigravida Preterm Pregnancy. Indonesian Journal of Global Health Research. 4: 1-8.
- Scully M, Hunt BJ, Benjamin S, Liesner R, Rose P, Peyvandi F, et al. (2012) Guidelines on the diagnosis and management of thrombotic thrombocytopenic purpura and other thrombotic microangiopathies. British journal of haematology. 158.
Article Information
Case Report
Received Date: August 03, 2025
Accepted Date: August 21, 2025
Published Date: August 28, 2025
A Case Report on Partial HELLP Syndrome in Lagos, Nigeria
Volume 1 | Issue 2
Citation
Dr Akinlusi, Dr Awusi (2025) A Case Report on Partial HELLP Syndrome in Lagos, Nigeria. Eur J Case Rep 1: 201
Copyright
©2025 Dr Akinlusi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: ejcr.2025.1.201