

Review Article
Volume-1 Issue-1, 2025
Physicians’ Guideline Adherence Assessment in the Management of Hypertension Working in Public Teaching Hospitals in Addis Ababa, Ethiopia
-
Received Date: February 01, 2025
-
Accepted Date: February 18, 2025
-
Published Date: February 25, 2025
Journal Information
Abstract
Background: Clinical guidelines are systematically proven statements that help physicians to make healthcare decisions for specific medical conditions. Non-adherence to clinical guidelines is believed to contribute significantly to poor delivery of clinical care, and hence poor clinical outcomes. This study aimed at investigating adherence of doctors to hypertension clinical guidelines in public Teaching Hospitals, Addis Ababa, Ethiopia.
Methods: A Facility based descriptive cross-sectional study was conducted from November 2017 to March 2018 on a sample of 217 doctors. Adherence of doctors to hypertension guidelines was measured through the modified JNC7, and 8 adherence tool. Descriptive statistics was used to summarize the data (mean, standard deviation, median) and analyzed by frequency tables. Chi square test was used to determine the association among categorized variables. Logistic regression analysis was used to determine the relationship between adherence to hypertension guidelines and the explanatory variables. All statistical tests were considered statistically significant when p value < 0.05.
Results: Of the 204 participants, 75.9% (155/204) were aware of the major hypertension treatment guidelines. PHGA score among male and female physicians was 34.9% and 20.6% respectively. In this study, the overall physicians’ hypertension guideline adherence mean score was 54.7% with a standard deviation ±17.8. Only 28.1% of the physicians score 70% and above. The chi square test shows that there is statistical significant difference between males and females regarding PHGA score (χ2(1, N = 203) = 4.437, P < 0.05) and OR=0.484, 95% CI: (0.257, 0.913). This study showed that male physicians and female physicians were almost equally likely to adhere the guideline.
Conclusion: The overall adherence of physicians to hypertension treatment guidelines was very low. This study highlights how a gap in clinical governance contributes to low adherence to clinical guidelines. Establishing regular clinical audit, issuing regulations to enforce the use of updated guidelines, along with introducing training programs in hospitals and continuous assessment to the practicing physicians are suggested as crucial interventions. Considerable efforts to build clinical governance in Ethiopia are required.
Key words
Physicians; Adherence; Hypertension; Clinical guidelines; Clinical governance; Ethiopia
List of abbreviations: JNC: Joint National Committee; OPD: Outpatient Department; PHGA: Physicians’ Hypertension Guideline Adherence
Variables |
Frequency |
PHGA score ≥ 70 |
Percentage |
Gender |
|
|
|
|
106 |
37 |
34.9 |
|
97 |
20 |
20.6 |
Age |
|
|
|
|
45 |
13 |
28.9 |
|
102 |
30 |
29.4 |
|
43 |
14 |
32.6 |
School of graduation |
|
|
|
|
36 |
12 |
33.3 |
|
29 |
8 |
27.6 |
|
24 |
6 |
25 |
|
17 |
7 |
41.2 |
|
17 |
6 |
35.3 |
|
13 |
3 |
23.1 |
|
8 |
2 |
25 |
|
59 |
13 |
22 |
Year of graduation |
|
|
|
|
29 |
14 |
48.3 |
|
117 |
39 |
33.3 |
Service year |
|
|
|
|
88 |
22 |
25 |
|
88 |
31 |
35.2 |
|
27 |
4 |
14.8 |
 |
| Figure 1: Majority (78.8%) of the respondents reported as having exposure and awareness about JNC 8 guideline |
Introduction
Hypertension (HTN) is the most common modifiable risk factor for cardiovascular diseases, stroke, and renal failure. It is the second leading cause of chronic kidney disease (CKD). It is estimated that more than one billion adults are hypertensive worldwide currently and this figure is projected to increase to 1.56 billion by the year 2025, which is an increase of 60 % from 2000 [1]. Cardiovascular diseases and Hypertension are accounting for loss of 4 % gross domestic product for low and middle-income countries annually. Clinical evidence suggests that lowering blood pressure (BP) with antihypertensive drugs reduces the risk of myocardial infarction, stroke, heart failure, revascularization procedures and end-stage renal diseases in hypertensive patients. The increasing prevalence of hypertension has been attributed to population growth, ageing and behavioral risk factors, such as unhealthy diet, excess use of alcohol, sedentary lifestyle, obesity, and exposure to persistent stress. A total of 9.4 million deaths occur worldwide every year because of hypertension, with it being responsible for about 50% of mortality due to heart disease and stroke. Epidemiological studies demonstrated that prevalence of hypertension is increasing rapidly in Ethiopia. Recent survey in Addis Ababa revealed that the prevalence of HTN is 31% and 28% in men and women respectively [2].
Though effective pharmacological treatments for the management and control of hypertension are available, it remains among the priority public health concerns due to its associated morbidity, mortality, and economic impact on the society [1-9]. To lessen its profound impacts, professional categories in various parts of the globe have devised clinical guidelines for the management of hypertension [9]. The guidelines are ‘systematically developed statements that assist practitioners and patients to make healthcare decisions for specific clinical circumstances’ [10]. They help to maintain consistent high quality standard health care services and minimize the economic burden that the treatment bear to patients [11].
Treatment has repeatedly proven effective in outcome studies in preventing stroke, heart failure, deteriorated renal function, new onset diabetes and, to some extent, coronary heart disease and other complications [12]. Randomized control trials (RCTs) have shown that most hypertensive patients will require at least two and often three or more medications of different drug classes plus lifestyle modification to control their hypertension [13].
Several guidelines have been developed worldwide for the management of hypertension, and these serve as reference standards for clinical practitioners. However, many clinicians practice their own prescribing pattern in treating hypertensive patients according to their clinical experience [10].
A case report-based survey carried out in southern Sweden to assess general practitioners (GPs) (n=109) adherence to HTN treatment guidelines showed that either under- or overtreatment in relation to current guidelines for the treatment of hypertension [14]. According to the study, despite international and national clinical guidelines on the treatment of hypertension, general practitioners often fail to correctly assess the cardiovascular risk for patients in a clinical setting. Most GPs use target blood pressure levels but do not consider other cardiovascular risk factors. Both under- and overtreatment of high and low cardiovascular risk groups were seen in this study.
Another cross-sectional study conducted in Germany implied that physicians’ knowledge of the guideline doesn’t lead to better adherence in practice. Therefore, the study recommends further investigation to address the determinants of the physicians’ guideline adherence [11].
A cross-sectional study conducted in north west province of South Africa to assess the adherence of physicians to clinical guidelines in district hospitals showed that low guidelines adherence rate in the management of hypertension. Age of physicians and less clinical experience were also identified as covariates of low guidelines adherence [10].
Uncontrolled blood pressure (UBP) is an independent risk factor leading to enormous complications and mortalities secondary to HTN. Inappropriate provision of medications could also lead to extra expense incurred to the patient due to ineffective treatment and adverse drug reactions. Lack of improvement and appearance of untoward side effects with the prescribed medication could result in distrust between the patient and the clinician. Ineffective drugs also provoke the physicians to frequently change the regimen and dose, thereby leading to fluctuation in patients’ blood pressure (BP) control.
Recent retrospective cohort study (n=897) conducted in Ethiopia to examine determinants of achieving BP control showed that only 37% of patient’s BP was controlled. The study also revealed that place of treatment, duration of treatment, treatment regimen and patient age were determinants of controlled BP [5]. Hypertension is often associated with additional cardiovascular disease risk factors, and the risk of cardiovascular disease increases with the total burden of risk factors [13].
Recently, high prevalence of Hypertension, evidences of prevalent uncontrolled Blood pressure and low physician’s guideline adherence rates have been seeking attention globally [11].
Methods
Study design and population
A Facility(hospital)based descriptive cross-sectional study was conducted in the public hospitals of Addis Ababa, Ethiopia, during the period from November 2017 to march 2018 on a simple of 217 medical doctors. Two hundred three physicians were voluntarily participated in the study with a response rate of 93.6%. One doctor refused to participate in the study. Data were collected using standardized pre coded structured questionnaires [15,17,18].
Questionnaires were adapted from the standardized sources and checked for consistency in our contexts. Pre-test was conducted and questionnaires were checked immediately for completeness and consistency
Statistical Analysis
Epi Info 7.1. was used to data entry and the entered data was exported to SPSS version 20 software for the final analysis. SPSS 20 was used to summarize the data numerically (mean, standard deviation, median) and graphically (frequency tables). Chi-squared (χ2) tests was used to determine the associations between categorical variables. A binary logistic regression analysis was performed to determine the relationship between adherence to hypertension guidelines and its associated factors. All statistical tests were considered as significant when p-value < 0.05.
Results
From the 203 study participants, 106(52.2%) were males, 93.6% (190/203) of the respondents were aged between 21 to 32 years and 184(90.6%) have year of experience of 1.75 year with a standard deviation of ± 1.78 year of experience. (Figure 1)
Case scenarios
Seven standardized scenarios were selected from different sources to assess hypertensive guideline adherence among physicians working in government teaching hospitals. The respondents were asked to respond accordingly for each of the scenarios. Their responses were evaluated against the truth value/correct answer that the guideline recommends
Therefore, by using the seven case scenarios each of the physicians were given twenty questions to respond accordingly in a selfadministered questionnaire. A cut off point < 70% considered as a poor adherence and ≥ 70% considered as a good adherence by the researcher. The cut off points were set by considering the post graduate grading system since the participants were a graduate and working independently at the OPD clinics.
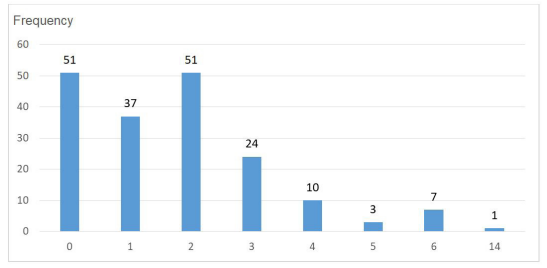
In this study, the overall physicians’ hypertension guideline adherence mean score was 54.7% with a standard deviation ±17.8%. It ranges from 0 to 85%. Only 28.1% of the physicians score 70% and above. Figure presents the frequency distribution of the adherence score.
Discussion
This study evaluated provider adherence with JNC 8 guidelines of physicians working in public teaching hospitals of Addis Ababa using a comprehensive questionnaire focusing on the common problems in the management of hypertension. Providers in these public teaching hospitals have lower adherence than other studies. The highest quality score was obtained in the area of cardiovascular risk assessment, which suggest that providers are cognizant of the risk factors contributing to target organ damage.
Lifestyle modification was the category with the lowest quality score and the only guideline area in which there were significant provider differences. The deficits in addressing LSM warrant comment in light of the current trend of practice. “pay for performance” quality monitoring. Moreover, recent analyses suggest that “paying” for performance may not be an effective incentive for improved quality [18], especially in patients with comorbid conditions [19]. Yet, as the pay for performance assessments move from a productivity-based incentive plan to a focus on quality, the documentation of care according to established guidelines will become a critical factor in provider evaluations. Until such time that electronic health records are standard within most health systems and a balance between productivity and quality assessments are the norm, documentation of teaching and counseling will continue to be a challenge to the quality monitoring process.
low-income African-American patients, stringent blood pressure goals were met among 44% of the patients, and 50% achieved the blood pressure goal of less than 140/90 mm Hg, which is comparable with national averages [4]. Although providers were 69% adherent with pharmacologic treatment guidelines, 62% of the patients who were not at goal were taking less than 3 antihypertensive medications.
Numerous studies have shown that it takes an average of 3.4 medications to achieve blood pressure control [3]. Additionally, 64% of patients not at goal at a particular visit did not have their medication intensified.
Follow-up visit schedule was the only factor significantly related to blood pressure goal attainment, but there was no correlation between visit schedule and medication adjustment. Follow-up visits without a purposeful link to treatment intensification may not be a cost-effective strategy for hypertension management. Although blood pressure goals were not achieved for half of the patients, a decrease of 5 mm Hg in systolic blood pressure and of 6 mm Hg in diastolic blood pressure in the physician group is an important finding. Contrary to previous research, provider consistency was inversely related to changes in blood pressure, raising the question of whether being unfamiliar with the patient or discontinuity resulted in resident physicians being more aggressive with blood pressure management. A study of nurse practitioners found that longer-term relationships diverted the provider and patient toward al- ternate social or family issues and away from the “medical” aspects of care, suggesting that an emphasis on relation- ship building could be deleterious to the patient’s physical health. Anecdotal findings in the current study, however, revealed that nurse practitioner documentation focused on multiple medical issues at most visits (eg, vaginitis, mammograms, Pap smears), whereas physician documentation focused on blood pressure management. A larger sample and a study that specifically addresses follow-up care, medication intensification, prescription usage, and the nuances of chronic disease management would provide a better understanding of the relationship among these variables. The fact that 26% of the original subjects did not return for a second visit in 6 months and the majority of those patients were seen by a resident physician underscores the importance of evaluating the interpersonal processes that affect trust and patient willingness to return for care. This study also evaluated differences in guideline adherence and hypertension outcomes by provider type. Differences were noted in certain aspects of the care provided. Patients seen by nurse practitioners were significantly more likely to return for at least 1 follow-up visit and receive lifestyle teaching in all areas, while physicians were more likely to make medication adjustments and achieved greater reductions in diastolic blood pressure readings. The diastolic blood pressure reduction difference contradicts earlier research comparing nurse practitioners and physicians [18]. However, these findings are consistent with other research that has shown that nurse practitioners and physicians achieve similar health outcomes but use different processes of care [12].
Nurse practitioner education places significant emphasis on the interpersonal aspects of care. As a result, nurse practitioners are more likely to spend time teaching and counseling patients regarding lifestyle changes prior to intensifying pharmacologic treatments as compared with physicians. In contrast, resident physicians report low rates of cardiovascular disease counseling [19] and low confidence in lifestyle counseling interventions in primary care. Although behaviors can be increased and confidence gained through targeted interventions, resident physicians report numerous barriers to behavioral counseling, including time limitations, perceived ineffectiveness, and a lack of training [19]. More than half of the patients seen by both types of providers did not attain blood pressure goal suggests that a collaborative model of care may be an effective option for achieving better control and a higher overall level of quality of care. One study compared the quality of hypertension outcomes for groups treated by physicians versus groups treated by a physician-nurse (non–nurse practitioner nurses) team. The physician-nurse team demonstrated lower mean systolic and diastolic pressures and a higher score for blood pressure medication knowledge. Unfortunately, the paper did not define the dynamics of the nurse-physician team, leaving unclear the effect of the nurse’s role or whether members of the team had contact with the patient together or individually. Other research has found that patients’ lack of understanding of the disease process, concerns over side effects of medications, and lack of shared decision making are associated with lack of adherence to antihypertensive regimens. A team approach that combines the interpersonal emphasis of the nurse practitioner with the technical emphasis of the physician could be a viable solution to these non-adherence challenges.
Findings from the current study need to be interpreted in light of the study limitations. The number of returning patients was small and reflects a potential selection bias. Additionally, although the patients had severe income limitations, they had access to both health care and medications. It may be that these 2 factors are more important than guide- line adherence in achieving blood pressure. Additionally, the current study shares the limitations common to quality audits and chart reviews. Nurse completion of the HQI was time- and effort-intensive. The time-intensive nature of comprehensive quality indicator tools is a well- known dilemma in the area of process improvement [11]. Developing standardized instruments and data collection processes to ensure the reliability and ease of use of quality measures is an important step in improving the quality of care provided to patients with hypertension. Additionally, chart reviews are limited by the level of documentation recorded. Such reviews cannot determine if the deficit noted is due to level of provider skill or reflective of time and documentation constraints. A comparison of providers across a variety of documentation systems would provide insight into the usefulness of the HQI to assess the quality of care provided.
Conclusion
The overall adherence of physicians to hypertension treatment guidelines was very low. This study highlights how a gap in clinical governance contributes to low adherence to clinical guidelines. Establishing regular clinical audit, issuing regulations to enforce the use of updated guidelines, along with introducing training programs in hospitals and continuous assessment to the practicing physicians is suggested as crucial interventions. Considerable efforts to build clinical governance in Ethiopia are required.
Acknowledgments
We would like to acknowledge the study participants for their participation in the study
Availability of data and materials
The datasets used and/or analyzed during the current study will be available from the corresponding author on reasonable request
Authors’ contribution
F.A. Designed and implemented the research, GM and YL conducted the data analysis and drafted the manuscript, supervised the field implementation of the research and reviewed the manuscript. YL Proof read the final manuscript. All authors approved the final version of the manuscript prior to submission.
Ethics approval and consent to participate
Ethical clearance was granted from S.t Paul’s Hospital Millennium Medical College (SPHMMC) Institution Ethical Review Board to proceed with the field work. Written consent was obtained from each participant.
Competing interests
The authors declared that they had no competing interests.
References
- Jarari N, Rao N, Peela JR (2016) A review on prescribing patterns of antihypertensive drugs, Jarari et al. Clinical Hypertension 22: 7.
- Abdissa SG, Feleke Y, Awol M (2014) Prevalence of hypertension and pre-hypertension in Addis Ababa, Ethiopia: A survey done in recognition of World Hypertension Day, Original article, 2014 page 1-9.
- World Health Organization (2014) Ethiopia: NCD Synergies.
- Alemayehu CM (2013) Clinical Medicine Research 2: 94-100.
- Weber MA (2014) Clinical Practice Guideline for the management hypertension, a statement by the ASH and ISH 32: 1.
- ESH/ESC (2013) Guideline for the management of arterial hypertension.
- Berhe DF, Abera HM (2017) BMJ Open 2017: 7: e015743.
- Derbew FB, Katja T, Haaijer-Ruskamp FM, Afework M, Mengistu TY (2017) BMJ Open.
- Naru FU, Malik M, Hussain A (2016) Prescriber adherence to standard treatment guideline for the management of hypertension, Int J Res Appl Natural Social Sci 4: 49-58
- Asafa R. Adedeji John Tumbo (2016) Adherence of doctors to a clinical guideline for hypertension in Bojanala district, NorthWest Province, South Africa: 1-9.
- Karbach U, Schubert I, Hagemeister J, Ernstmann N, Pfaff H (2011) Physicians knowledge of and compliance with guidelines: An exploratory study in cardiovascular diseases. Dtsch Arztebl Int 108: 61–9.
- The ESC Textbook of Cardiovascular Medicine 2008: 287-308.
- Harrison’s Cardivascular medicine 2010: 422-44.
- Rickard Ekesbo, PatrikMidlöv, Sofia Gerward, Kristin Persson, Christina Nerbrand and Lennart Johansson Lack of adherence to hypertension treatment guidelines among GPs in southern Sweden-A case report-based survey BMC Family Practice 2012: 13: 34.
- Berhe DF, Taxis K, Haaijer-Ruskamp FM (2017) Hypertension treatment practices and its determinants among ambulatory patients: retrospective cohort study in Ethiopia. BMJ Open 7: e015743.
- Kenneth E Olive JNC 8, Sep 8,2015.
- Rickard Ekesbo, Patrik Midlöv, Sofia Gerward, Kristin Persson, Christina Nerbrand (2012) BMC Family Practice 13: 34
- HG Mengesha (2018) Comparative effectiveness of antihypertensive drugs prescribed in Ethiopian healthcare practice: A pilot prospective, randomized, open label study
- Tsui Kelly, Dodson, Terry A (2012) Jacobson, MD Atlanta Cardiovascular Disease Prevention Counseling in Residency: Resident and Attending Physician Attitudes and Practices Judith, Georgia and Dallas, Texas
Artcle Information
Review Article
Received Date: February 01, 2025
Accepted Date: February 18, 2025
Published Date: February 25, 2025
Journal of Cardiovascular Research and Heart Valve Disease
Volume 1 | Issue 1
Citation
Fetene Adamu Nteneh (2025) Physicians’ Guideline Adherence Assessment in the Management of Hypertension Working in Public Teaching Hospitals in Addis Ababa, Ethiopia. J Cardiovasc Res Heart Valve Dis 1(1):101
Copyright
©2025 Fetene Adamu Anteneh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jcrh.2025.1.101