

Review Article
Volume-1 Issue-1, 2025
Modified Duke’s Criteria Fulfilled Staphylococcal Infective Endocarditis in A Newborn with Structurally Normal Heart
-
Received Date: April 03, 2025
-
Accepted Date: April 19, 2025
-
Published Date: April 26, 2025
Journal Information
Abstract
Background: Occurrence of infective endocarditis is infrequent in pediatric population especially neonates and is associated with high morbidity and mortality if not managed timely.
Case: A term extramural female baby born with a setting of Rh incompatibility required umbilical venous access for exchange level hyperbilirubinemia.Two days following which baby developed features of sepsis, shock and respiratory failure and pneumothorax requiring mechanical ventilation and chest drain insertion. Baby also had gangrene of big toe tip. Sepsis screen was positive, Echocardiography revealed structurally normal heart with vegetations over tricuspid valve. Serial blood culture grown growth of methicillin sensitive staphylococcus aureus.
Management: Baby diagnosed as having infective endocarditis according to modified Duke criteria. She was managed with ventilator care and supportive measures, empirically started on Meropenem vancomycin and later clindamycin added according to culture and sensitivity report. Antibiotics given for a total of 4 weeks. Follow up ECHO was normal. Baby discharged with stable vitals and on breastfeeds.
Conclusion: Early diagnosis and appropriate treatment can result in positive outcome in this rare disease.
Key words
Newborn; Infective Endocarditis; Staphylococcus aureas
Culture specimen |
Organism grown |
Pencillin |
Ampicillin |
Cloxacillin |
Gentamicin |
Amox/clav |
Clindamycin |
Ceftriaxone |
Tetracycline |
Trimethoprim |
Ciprofloxacin |
Linezolid |
Rifampicin |
Vancomycin |
Blood 1 |
MSSA |
R |
R |
S |
S |
S |
S |
S |
S |
S |
R |
S |
S |
S |
Blood 2 |
MSSA |
R |
R |
S |
S |
S |
S |
S |
S |
S |
R |
S |
S |
S |
ET secretions |
MSSA |
R |
R |
S |
S |
S |
S |
S |
S |
S |
R |
S |
S |
S |
 |
| Figure 1: Digital gangrene on left big toe |
 |
| Figure 2:Right side ICD in situ, left sided consolidation with ? pneumatocele (arrow) |
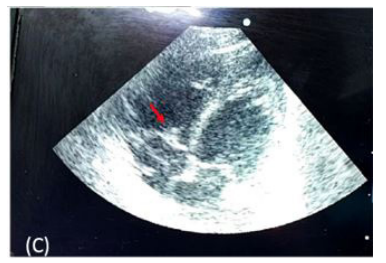 |
| Figure 3:Vegetation on anterior tricuspid leaflet (arrow) on echocardiography |
Introduction
Infective endocarditis (IE) in a neonate is a relatively rare occurrence with high mortality and morbidity if not treated appropriately. IE is infrequent in pediatric population with structurally normal heart but is been more and more diagnosed even in the absence of congenital heart disease [1]. Newborn IE constitutes 7- 8 % of all pediatric IE and the recent increase in incidence has been attributed to the rampant use of invasive central lines in the management of various medical conditions [1]. We present an extramural baby with a structurally normal heart, who developed IE secondary to use of an umbilical line and developed complications including pneumonia, shock and digital gangrene. A high index of suspicion and early targeted antibiotics resulted in the successful treatment of the condition.
Case
A term, 38 weeks, extramural female baby born by elective cesarean section to a B-negative gravida two mother, with a birth weight of 2600g, at a district level hospital. Baby cried soon after birth and was started on breastfeeds. Baby’s blood group was B-positive and DCT was positive, received phototherapy and developed exchange level hyperbilirubinemia (total bilirubin 20mg/dl) on day of life 3. Umbilical catheterization was done for double volume exchange transfusion subsequently the bilirubin levels came down to 15mg/dl. On day 6 of life, baby developed fever, abdominal distension, redness around umbilicus and purulent discharge for which umbilical lines were removed and also developed respiratory distress requiring continuous positive airway pressure (CPAP) support. Respiratory distress worsened on day 9 of life and baby was put on invasive ventilation, also developed right pneumothorax for which ICDT was inserted and was referred to our hospital on manual IPPR. At admission baby was on manual IPPR ,had right sided intercostal drainage (ICD) , started on mechanical ventilation (SIMV with PIP 16mmHg, PEEP 5mmHg, Rate 35perminute and FiO2 40%) and had features of shock, with HR-180 per minute ,poor peripheral pulses and low blood pressure (BP 42/28(MAP 32)mmHg), for which she was started on inotropic support of Dopamine 10 microgram/kg/min Dobutamine 20 microgram/kg/min and Adrenaline 0.3 microgram /kg/min. Baby had one episode of clonic seizure also for which loading dose of Phenobarbitone was given.
There was also gangrene of left foot big toe tip (Figure 1) for which subcutaneous low molecular weight heparin was started. Blood investigations showed leukocytosis (total leukocyte count – 15.3 x 106/L, polymorph 69%) and an elevated CRP (101mg/dl). X ray showed right ICD tube in situ with no residual pneumothorax. There was bilateral haziness suggestive of pneumonia and also a left midzone pneumatocele (Figure 2). This was later ultrasonographically detected to be left upper lobe collapse consolidation with air bronchogram. Screening bedside echocardiography was done and it revealed swinging vegetations on tricuspid valve leaflet. A structurally normal heart with patent foramen ovale and vegetations over anterior tricuspid valve of size 0.32cm was subsequently confirmed by pediatric cardiologist (Figure 3). Doppler flow imaging for of lower limb vessels was normal.
Baby was empirically started with Meropenem, Vancomycin and Amphotericin B. Two blood cultures were sent, one at admission and another after eighteen hours. Both grew methicillin sensitive staphylococcal aureus (MSSA). Antibiogram is provided in Table 1. Endotracheal tube secretions also revealed MSSA growth with similar sensitivity pattern. Eye examination and ultrasonography of brain, kidney, ureter and bladder were normal. Lumbar puncture was negative for meningitis; and urine culture was sterile. Baby gradually improved with antibiotics and supportive measures. ICD tube was removed on day 14 of life and extubated on 15th day of life to CPAP (6/25%) support and to nasal prongs oxygen on 23 days of life. Baby was made off oxygen by twentyfifth day of life. Follow up X-ray showed resolving pneumonia. Repeat blood culture sent on day 20 was sterile. CRP came down (11mg/dl on day 25 of life). Digital gangrene did not progress further and improved. Anticoagulants were given for 2 wks. Baby received PRBC, platelet transfusions for anemia and thrombocytopenia (80 x 106/L). Follow up ECHO on 26th day of life showed no vegetations, normal biventricular function and mild tricuspid regurgitation. CRP became negative Antibiotics were given for a total of six weeks and baby was discharged. In follow up baby was on full breastfeeds with stable vitals and normal growth.
Discussion
Here we present the case of a newborn with structurally normal heart, who developed severe sepsis, IE and complications like digital gangrene and pneumonia following invasive central line catheterization. IE was diagnosed by modified Duke Criteria and the child satisfied both the major criterias i.e, (i) An oscillating intracardiac mass on the valve or supporting structures on echocardiogram and, (ii) Two positive cultures from blood samples drawn more than 12 h apart [2,3]. It assures that modified Duke criteria holds equally good for diagnosis of IE in newborns.
IE in newborn was once a fatal disease often diagnosed postmortem [4]. Neonatal IE is different from pediatric and adult IE in that fewer than one third cases has associated congenital heart disease. The increasing use of central lines, parenteral nutrition and invasive procedures facilitates the entry of surface bacteria, resultant bacteremia and valve damage [1]. The right side of heart is more commonly affected, even though both valve involvement has been described in adults and rarely in neonates [5]. In our case also, the use of umbilical vein catheter might have been the culprit to cause damage to the endothelial surface, platelet and fibrin deposition further acting as a nidus for bacterial colonization.
Manifestations of IE in neonate overlaps with those of other common diagnosis like sepsis. However septic emboli and resultant osteomyelitis, pneumonia or meningitis has been described in patients with IE [1]. Our case also had digital gangrene and pneumonia. Other manifestations seen in children and adults like arthritis, arthralgia and immunological phenomenon are rare in newborns.
Common pathogens responsible for neonatal IE include Staphylococcus aureus, coagulase negative staphylococcus, gram negative bacteria and candida species, guiding the empirical therapy till a culture report is available. Rarely Klebsiella, group B streptococcus, Enterococcus, Burkholderia and Pseudomonas has been reported as causative agents (2,6–8). Sensitive antibiotics at minimal inhibition concentration given for a period of 4-6 weeks and monitored by blood culture and echocardiography helps in the resolution of IE and its complications. However, significant embolic events, left sided severe stenosis or regurgitation, persistant cardiac failure and very large vegetations (>10mm) warrant surgical intervention. Our patients blood culture had grown methicillin sensitive staphylococcus aureus and was given sensitive antibiotics Vancomycin and Clindamycin for a period of 4 weeks.
Complications of IE include acute cardiac failure due to rupture of chordae tendinae or perforation of valve leaflet. Ventricular dysfunction and valvular insufficiency can cause insidious cardiac failure. Other cardiac complications include arrythmias and periannular extension of infection. Embolic episodes to cerebral ,pulmonary renal or coronary vessels can occur especially in fungal or staphylococcal IE or with large lesions >10mm size. These are more common in mitral and aortic vegetations. Extra cardiac complications include mycotic aneurysms and renal failure(9). Our baby even though diagnosed with staphylococcal IE did not develop any complications or embolic phenomenon, probably as a result of early diagnosis and appropriate management.
Conclusions
Newborn infective endocarditis is a rare entity with high morbidity and mortality. High index of suspicion should be kept in newborns with invasive lines and thrombotic episode .Confirmation of diagnosis can be done by blood cultures and bedside echocardiography. Early targeted treatment can result in resolution of symptoms without sequelae.
Learning Points
• Strict asepsis measures to be taken while doing any invasive procedures in a neonate.
• High index of suspicion of IE in a neonate with thrombotic episode.
• Early and appropriate treatment is life saving in this fatal disease.
References
- Baltimore RS, Gewitz M, Baddour LM, Beerman LB, Jackson MA, et al. (2015) Infective Endocarditis in Childhood: 2015 Update: A Scientific Statement From the American Heart Association. Circulation 132: 1487–515.
- McLennan D, Morgan G (2018) Infective Endocarditis, a Rare Complication of Late Neonatal Group B Strep Sepsis. Front Pediatr 6: 274.
- Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG, et al. (2000) Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 30: 633–8.
- Millard DD, Shulman ST (1988) The changing spectrum of neonatal endocarditis. Clin Perinatol 15: 587-608.
- Varghese TG, Revankar VR, Thomas SC (2015) A rare case report of neonatal infective endocarditis with concomitant involvement of the mitral and tricuspid valves. J Indian College of Cardiology 5: 341–4.
- Nadroo Ali Mohd, Al She Wear Abdulrahman, Al Sowailem Abdul Mohsen, Al Jubair Fahad (1997) Infective Endocarditis in a Neonate. Annals of Saudi Med 17: 347–9.
- Nasser BA, Al Qwaee A, Almesned AR, Akhfash A, Mohamad T, et al. (2019) Infective endocarditis in children with normal heart: Indication for surgical intervention. J Saudi Heart Assoc 31: 51–6.
- Yonas E, Damay V, Pranata R, Nusarintowati N (2018) Infective endocarditis due to Burkholderia cepacia in a neonate: a case report. J Med Case Rep 12: 120.
- Ferrieri P, Gewitz MH, Gerber MA, Newburger JW, Dajani AS, et al. (2002) Unique features of infective endocarditis in childhood. Pediatrics 109: 931–43.
Artcle Information
Review Article
Received Date: April 03, 2025
Accepted Date: April 19, 2025
Published Date: April 26, 2025
Journal of Cardiovascular Research and Heart Valve Disease
Volume 1 | Issue 1
Citation
Nisha Menon (2025) Modified Duke’s Criteria Fulfilled Staphylococcal Infective Endocarditis in A Newborn with Structurally Normal Heart. J Cardiovasc Res Heart Valve Dis 1: 102
Copyright
©2025 Bijaylaxmi Behera. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jcrh.2025.1.102