

Review Article
Volume-1 Issue-1, 2025
Carbon Dioxide Laser Ablation of Epidermal Cysts as Well as Milia Cysts: A Novel Approach to Treatment
Received Date: January 05, 2025
Accepted Date: January 23, 2025
Published Date: January 30, 2025
Journal Information
Abstract
The excision of any lesion, benign or malignant has the inevitable sequelae of scarring. Epidermal inclusion cysts such as sebaceous cysts or epidermal cysts, and milia are frequently occurring lesions that are most commonly excised surgically. Epidermal cysts are benign lesions of the skin and reasons for removing them can be functional (depending on site and size), cosmetic or due to multiple infections. Surgical excision is the conventional method of removal, however, when it comes to large epidermal cysts in aesthetically sensitive areas such as the face and neck, an aesthetically pleasing result can often be difficult to achieve as it may lead to a poor scar or poor contouring.
Introduction: Traditionally, either a wide excision is performed or a more limited incision with the goal to remove the cyst in its entirety, including both anterior and posterior walls. The aim is to avoid the possibility of recurrence and infection. The former technique will lead to a potentially long scar, but ultimately, both can lead to poor scarring and potential poor contouring. There are a number of surgical techniques described in the literature [1], all which aim to minimise the length and visibility of the scar. These techniques were characterised as minimal excision techniques. Wu H et.al were the first to mention CO2 laser in the treatment of sebaceous cysts, but this was for access rather than definitive treatment [2].
We therefore put forward this novel way of treating sebaceous cysts and milia, by use of Carbon Dioxide laser as a definitive treatment by ablation, which has not been described. We present a case series of four patients, all of which were treated with CO2 laser in one setting and present the resultant promising cosmetic outcomes. Though neither the pathology of the cysts nor the modality of the CO2 laser are unique, the treatment approach.
Key words
Squatting Facet, Trochlear extension, Talus, North-eastern, Nigerians
 |
| Figure 1: Technique example shown below, on a patient with multiple cysts on right forearm
Figure 1A-F A. Figure of a patient's right forearm depicting multiple cysts. B. The skin overlying the cyst is ablated with the Carbon dioxide laser using a pulsed mode. In this case the laser parameters were 125mJ, at 20Hz using a 2mm spot. C. The anterior cyst wall is ablated and the cyst contents expressed. D. For illustrative purposes, the rest of the cyst wall is controlled using a needle, and the rest of the cyst is ablated away. With experience, the cyst can be ablated along with the back wall without other instrumentation. E. The remaining cyst is ablated away F. A final light ablation is undertaken of the posterior wound bed in case of residual cyst wall remnants to mitigate recurrence. The wound can be dressed as it is, or alternative the wound edges approximated with Steristrips. |
 |
| Figure 2(a-c) Figure 2A: Confluent cystic lesions left cheek prior to treatment Figure 2B: Posterior wall of lesion treated with CO2 laser after contents have been expressed Figure 2C: Lesion 2 months post CO2 laser treatment. Mild erythema visible. |
 |
| Figure 3 |
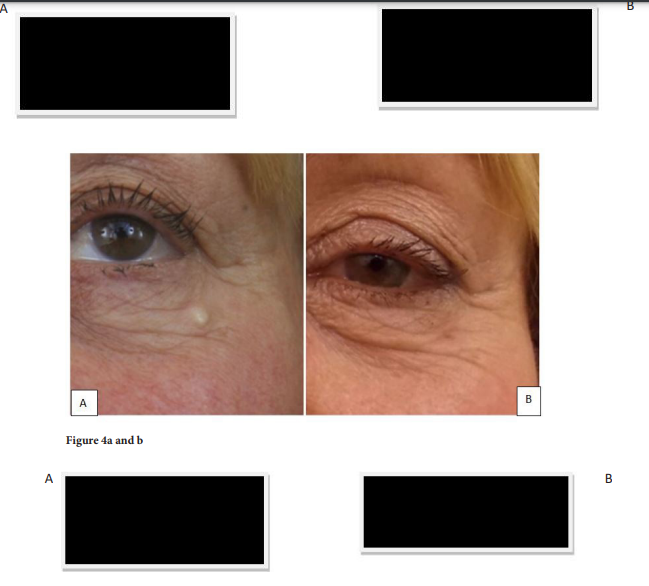 |
| Figure 4 |
 |
| Figure 5 |
 |
| Figure 6: Effect of azide treatment and pre-treatment on protein content in the green (a) and (b) red stage of H. pluvialis. Values are means of three-replications ±standard deviation. Different letters show the significant difference with p< 0.05 in one-way ANOVA and Duncan's tests |
Introduction
The excision of any lesion, benign or malignant has the inevitable sequelae of scarring. Epidermal inclusion cysts such as sebaceous cysts or epidermal cysts, and milia are frequently occurring lesions that are most commonly excised surgically. Epidermal cysts are benign lesions of the skin and reasons for removing them can be functional (depending on site and size), cosmetic or due to multiple infections. Surgical excision is the conventional method of removal, however, when it comes to large epidermal cysts in aesthetically sensitive areas such as the face and neck, an aesthetically pleasing result can often be difficult to achieve as it may lead to a poor scar or poor contouring. Traditionally, either a wide excision is performed or a more limited incision with the goal to remove the cyst in its entirety, including both anterior and posterior walls. The aim is to avoid the possibility of recurrence and infection. The former technique will lead to a potentially long scar, but ultimately, both can lead to poor scarring and potential poor contouring. There are a number of surgical techniques described in the literature [1], all which aim to minimise the length and visibility of the scar. These techniques were characterised as minimal excision techniques. Wu H et.al were the first to mention CO2 laser in the treatment of sebaceous cysts, but this was for access rather than definitive treatment [2].
We therefore put forward this novel way of treating sebaceous cysts and milia, by use of Carbon Dioxide laser as a definitive treatment by ablation, which has not been described. We present a case series of four patients, all of which were treated with CO2 laser in one setting and present the resultant promising cosmetic outcomes. Though neither the pathology of the cysts nor the modality of the CO2 laser are unique, the treatment approach.
Methods
We present our treatment of patients and prospective evaluation of the results. All lesions were biopsied to assess suitability for laser treatment. The laser used was a Cynosure Performa Carbon Dioxide laser with a 1mm surgical hand piece at 30 watts, pulse duration of 2ms in pulsed mode and with off time of 35ms.
We elaborate further on the extended use of the CO2 laser to treat similar lesions through complete ablation of the overlying skin, anterior and posterior cyst wall or allowing a conglomeration of cysts and cyst contents to shed after ablation of the posterior wall. One lesion was more amenable to CO2 laser ablation of the anterior wall and removal of the cyst wall not dissimilar to the technique previously described [2,3].
Our description of the use of CO2 laser has shown excellent cosmetic results and no recurrence in a number of patients as illustrated.
Results
Case 1A 63-year-old gentleman was referred to our outpatients’ clinic with multiple lesions on his left cheek (figure 2a). These were biopsied and confirmed to be benign milia, confirmed histologically by small white benign superficial keratinous cysts resembling epidermal cysts with a wall of stratified epithelium of a few cell layers. The patient was treated with a Cynosure Performa Carbon Dioxide laser with a 1mm surgical hand piece at 30 watts, pulse duration of 2ms in pulsed mode and with off time of 35ms. Initially, the anterior wall of the lesion was treated, with subsequent expression of cystic contents. After washout with 0.9% Saline solution, the posterior wall was ablated and cyst contents expressed or allowed to shed (figure 2b).
The patient was reviewed at 6 months post treatment having had an exceptionally good result after carbon dioxide laser treatment to multiple large cysts of his left cheek. The residual erythema had resolved when reviewed at a further 6 months. The patient had no evidence of recurrence after 5 years.
Case 2A 57-year-old gentleman presented to our clinic with another milia cystic lesion on his left inner canthus. This again was confirmed histologically to be benign milia, with white benign superficial keratinous cysts resembling epidermal cysts with a wall of stratified epithelium of a few cell layers. This was treated with a CO2 laser, with identical setting as in case 1. Figure 3a shows the lesion prior to treatment and figure 3b immediately after. A simple ointment is applied post treatment to keep the wound hydrated.
Case 3Figure 4a shows a third milia lesion histologically confirmed as per lesions in case 1 and 2. This presented on the left lateral lower eyelid on a female patient and is shown before treatment and figure 4b shows the same lesion after CO2 laser treatment. Similar settings to the CO2 laser were used as in the aforementioned patients.
Case 4Figure 5a shows a male patient with a similar lesion as the aforementioned patients, again histologically confirmed. It presented on the left cheek prior to CO2 laser treatment, and figure 5b shows the left cheek lesion 2 months after CO2 laser. Again, laser settings similar to the previous cases.
Discussion
Epidermal inclusion cysts are some of the most commonly occurring benign epithelial tumours. They are firm-tofluctuant, slow-growing, dome-shaped lesions that frequently appear on the trunk, neck, face, scrotum, or behind the ears [4]. These lesions are commonly treated by surgical excision, inevitably resulting in a scar. Anatomically, the apex of an epidermal cyst is attached to the dermis of the skin. However, the remaining portion of the cyst underneath the skin loosely attaches to the subcutaneous tissue and is freely mobile over it [3]. In addition, sebum, which is the content of the cyst, is composed mainly of the lipids squalene (sq), wax ester (we), triglyceride, free fatty acid, and cholesterol, which are secreted mostly from the sebaceous glands and by keratinocytes [5]. Recently, on this anatomical basis, minimally invasive methods have been suggested to avoid scarring [2,3,4,6], including the use of CO2 laser. The carbon dioxide laser emits infrared light at 10,600 nm which is absorbed by tissue water. In a continuous mode the laser will non-selectively vaporize tissue. In keeping with our use of the CO2 laser, Song et.al [3] proposed a new minimally invasive method that completely removes a cyst through a small hole made by a CO2 laser, however, the cyst itself was removed surgically.
Traditionally, either a wide excision is performed or a more limited incision with the goal to remove the cyst in its entirety, including both anterior and posterior walls. The aim is to avoid the possibility of recurrence and infection. The former technique will lead to a potentially long scar, but ultimately, both can lead to poor scarring and potential poor contouring. As mentioned by Nakamura et.al in their paper [1], there are a number of ways to surgically remove a sebaceous cyst: Danna [7] has described a technique that uses a diathermy needle to cauterize a portion of the overlying skin and the wall of the cyst; Patten [8], O’Keeffe [9], and Richards [10] mention the use of trephine, and Vivakananthan [11] advocates a minimal incision. Subsequently, Nakamura et.al described a further, simple technique, using an incisional procedure.
The minimal excision technique discussed by Moore et.al [12], Avakoff [13] and as mentioned above by Nakamura et.al. were similar to the punch technique, which can achieve minimal scarring but carries a risk of recurrence. For large cysts or cysts located in areas of thick skin, the cyst wall is more friable or not easy to express, making complete cyst removal with a better cosmetic appearance more difficult. [2]
Therefore, in putting forward this novel way of treating epidermal cysts and milia by use of Carbon Dioxide laser as a definitive treatment by ablation, we submit a technique that is novel and not previously described. We present a case series of four patients and one used as a step-by-step example describing the technique, all of which were treated with CO2 laser in one setting and present the resultant promising cosmetic outcomes.
Conclusion
The sole use of CO2 laser for complete ablation of both epidermal (pilar) cysts as well as milia has not been previously described as a technique that can be used routinely. We describe the use of CO2 laser in a versatile manner to treat a range of cysts to demonstrate that this procedure is straightforward, avoids surgery, and can produce excellent clinical results. We have had no recurrences as yet, having used the technique for many years. However, a bigger study and ideally randomised trial would be required to look at recurrence rates further. Although challenging, other outcomes to formally assess in future studies include: a) comparison of scarring and aesthetic outcomes between surgery and laser and b) cost of treatment.
Compliance with Ethical StandardsThe authors declare that they have no conflicts of interest.
References
- Nakamura M (2001) Treating a Sebaceous Cyst: An Incisional Technique. Aesthetic Plastic Surgery 25: 52-6.
- Wu H, Wang S, Wu L, S Zheng (2009) A New Procedure for Treating a Sebaceous Cyst: Removal of the Cyst Content with a Laser Punch and the Cyst Wall with a Minimal Postponed Excision. Aesthetic Plast Surg 33: 597-9.
- Song SW, Burm JS, Yang WY, Sang YK (2014) Minimally Invasive Excision of Epidermal Cysts through a small Hole Made by a CO2 Laser. Arch Plast Surg 41: 85-9.
- Zuber TJ (2002) Minimal excision technique for epidermoid (sebaceous) cysts. Am Fam Physician 65:1409-12.
- Feng CJ, Ma H (2015) Treatment of epidermal cysts with erbium: YAG laser fenestration: an alternative to surgical intervention. Ann Plast Surg 2: S89-92.
- Danna JA (1946) The treatment of sebaceous cysts by electrosurgical marsupialisation. Ann Surg 123: 952.
- Patton HS (1963) An alternative method for removing sebaceous cysts. Surg Gynecol Obstet 117: 645.
- O’Keeffe PJ (1972) Trephining sebaceous cysts. Br J Plast Surg 25: 411.
- Richards MA (1985) Trephining large sebaceous cysts. Br J Plast Surg 38: 583.
- Vivakananthan C (1972) Minimal incision for removing sebaceous cysts. Br J Plast Surg 25: 60.
- RB Moore, EB Fagan, Stephen H, DC Skolnik, G O'Sullivan (2007) Clinical inquiries. What’s the best treatment for sebaceous cysts. J Fam Pract 56: 315-6.
- Avakoff JC (1989) Microincision for Removing sebaceous cysts. Plast Reconstr Surg 84: 173-4.
Artcle Information
Review Article
Received Date: January 05, 2025
Accepted Date: January 23, 2025
Published Date: January 30, 2025
Journal of Dermatology and Clinical Cosmetics
Volume 1 | Issue 1
Citation
S Sofos, K Shokrollahi (2025) Carbon Dioxide Laser Ablation of Epidermal Cysts as well as Milia Cysts: A Novel Approach to Treatment. J Derm and Clin Cosm 1(1):101
Copyright
©2025 S Sofos. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jdcc.2025.1.101