

Review Article
Volume-1 Issue-1, 2025
Epidemiological,Clinical,Etiological and Therapeutics Aspects of Angioedema in Dakar, Senegal
-
Received Date: May 02, 2025
-
Accepted Date: May 20, 2025
-
Published Date: May 27, 2025
Journal Information
Abstract
Angioedema (AE) is an uncommon condition which can be life-threatening in case of laryngeal involvement or during anaphylactic shock. The studies concerning Ae are rare in sub-Saharan Africa. Ours aims were to determine the epidemiological-clinical characteristics and etiological factors of AE and to describe the management modalities in Dakar.
We conducted a descriptive and analytical study range from March 1st to August 31st 2017 in two dermatology departments (Institut d’Hygiene Sociale, Aristide Le Dantec Hospital) and one cardiology department (Aristide Le Dantec Hospital).
We included all patients presented with AE and who consented to participate in the study. During the study period, 37 patients were included, which standing for a 0.28% hospital Frequency. The mean age of our patients was 38.51 years old woth a sex ratio of 0.6 . The idiopatic histaminergic Ae was the predominant type with a frequency of 86.48% (n = 32). The allergic cause was present in 32.43% (n= 12). We have incriminated pseudo-allergy in 18.92% (n = 7). We found 5 cases of AE associated with medication in 13.51% of cases. The Angiotensin-converting enzyme (ACE) inhibitors were found in 4 cases and ARAII antagonist in 1 case The Angiotensin-converting enxyme (ACE) inhibitors were found in 4 cases and ARAII antagonist in 1 case . Different factors were identified food in 35% (n=3), medicinies in 29.73% (n=11) and physical exericise in 5.4% (n=2). The lips (43.24%, n = 16) were the predominant localization. Urticaria was present in 37.84% of cases (n=14), all of Whom had histaminergic AE. We found a statisrically significant relationship between urticaria and histaminergic AE (p = 0.03). Prick tests were positive in 13 cases with clinical concordance in 8 cases. The determination of IgE specific trophallergens allowed us to highlight a food allergy in 2 patients.
For histaminergic AE cases, treatment was based on anti-H1 exclusively in 29.73% (n = 11) or associated with oral corticosteroids in 35.13% (n = 13). For cases of bradykinic mediated AE, there was a change in medications along with a clinical follow up
Key words
Angioedema; Angiotensin Converting Enzyme Inhibitors; ARA II; Dakar
|
Complaints |
Number of patients |
Frequency (%) |
|
Cutaneous oedema |
27 |
72,97 |
|
Mucosal oedema |
19 |
51,35 |
|
Urticaria |
2 |
5,41 |
|
Itching |
2 |
5,41 |
|
|
10 |
27,03 |
|
Functional sign |
Number of patients |
Frequency (%) |
|
Itching |
11 |
29,73 |
|
Dyspnoea |
5 |
13,51 |
|
Dysphonia |
5 |
13,51 |
|
Tension-like pain |
3 |
8,1 |
|
Dysphagia |
1 |
2,7 |
|
Abdominal pain |
1 |
2,7 |
|
No sign |
11 |
29,73 |
|
Total |
37 |
100 |
|
Localisation |
Number of cases |
Frequency (%) |
|
|
Upper part of the body |
Lips |
16 |
43,24 |
|
Tongue |
4 |
10,81 |
|
|
Larynx |
1 |
2,7 |
|
|
Face |
13 |
35,14 |
|
|
Hands |
5 |
13,51 |
|
|
Eyelids |
4 |
10,81 |
|
|
Cheeks |
1 |
2,7 |
|
|
Ear lobule |
1 |
2,7 |
|
|
Lower part of the body |
Penis |
2 |
5,41 |
|
Foot |
6 |
16,22 |
|
 |
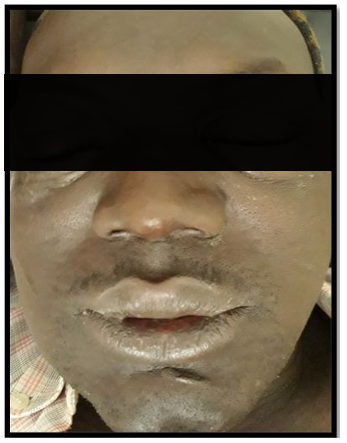
| Figure 1: Oedema was the same colour as the skin |
 |
| Figure 2 Oedema was the same colour as the skin with variable |
 |
| Figure 3 Oedema was the same colour as the skin with some multiple location |
 |
| Figure 4Oedema was the same colour in the patients |
 |
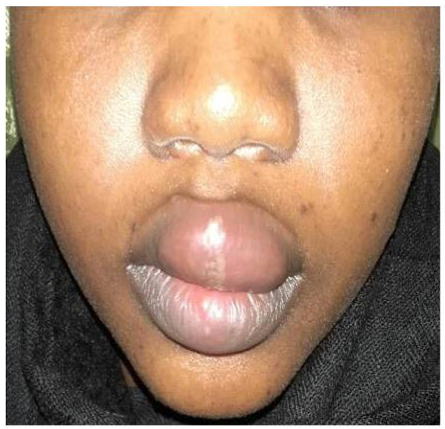
| Figure 5 Mucosal involvement was found |
Introduction
Angioedema is a clinical syndrome characterised by sudden lo calised swelling of the subcutaneous (hypodermal) and/or sub-- ma is coloured like the skin. It sets in within minutes or hours. It is transient and disappears without sequelae. It is not pruritic but can be painful [1,2]. In 2014, Crcardi et al [6] defined the following seven categories of AEs: idiopathic histaminergic, id iopathic non-histaminergic, acquired ACEI-related (+ sartans, gliptins, mTORinh, racecadotril, etc.), acquired C1-inhibitor deficiency (haemopathies, autoimmune diseases), inherited C1-in-hibitor deficiency, inherited with FXII (or plasmunogen, etc.) gene mutation, and inherited with unknown mutation. Studies of angioedema are scarce in sub-Saharan Africa [7]. Early man agement of an attack is crucial to improve prognosis. Indeed, only 25% of patients with a severe AE attack receive appropriate emergency treatment [4]. As a result, the patient's prognosis can be life-threatening, particularly in cases of laryngeal localisation. The main objective was to improve the management of AE in patients consulting a hospetal in Dakar. The specific objective were to determine the epidemiological and clinical characteristics of AE and to describe the management approches used in hospitals.
Patients and Methods
Type and period of study: We performed a multicentre study of descriptive, longitudinal and analytical purposes with prospec tive data collection over 6 months range from 01 March 2017 to 31 August 2017.
Study framework: This study was conducted in Dakar in the dermatology departments of the Institut d'Hygiène Sociale and the dermatology and cardiology departments of the Aristide le Dantec National Teaching Hospital Centre.
case definitionWe defined angioedema as any localised, soft, skin-coloured swelling of the subcutaneous and/or submucosal tissues that disappears within 1-4 days without sequelae.
We defined angioedema of "undetermined cause" as any idiopathic histaminergic or non-histaminergic angioedema.
The inclusion criteria consisted of: Any patient of any age, gender, who consulted during the study period for angioedema and who gave their consent to participate in the study.
Data collection method: We used a pre-established questionnaire.
The following variables were collected: Socio-demographic, clinical and biological. Respiratory prick tests were performed in patients with suspected atopy and native food and drug prick tests were performed if reported by the patient. Trophallergen specific IgE test was performed if food allergy was suspected A weighted C1-inh and C4 fraction of complement assay was performed if necessary. A functional C1inh assay could not be performed.
Ethical considerationsPatients were free to participate or not, and also had the possibility to request withdrawal from the study at any time. Confidentiality (personal information collected will not be relesed) was also required. Oral consented was rewuired to participated in the study The prick tests were performed free of charge.
Data input and processingData accuracy and quality were monitored throughout the survey. Data entry was conducted using Epi-infoTM7 software
Data were processed by a statistician using standard Microsoft Excel procedures using Epi-info 7 software.
Chi-square and Fisher tests were used according to their applicability conditions with a signifcance level of p< 0.05.
Results
During a 6-month period, we identified 37 patients who presented with AE. The hospital incidence was 0.28%. Twenty-three cases were female(62.16%)with a sex ratio (M/F) of 0.6 The mean age of our patients was 38.51 years (6 years to 80 years). The median age was 41 years.
Different complaints were founded and are illustrated in Table 1. Eight patients, standing for 21.62% of the cases, consulted for two or more reasons.
The delay of consultation was variable, sixteen patients consulted within 24 hours of the onset of symptoms while sixteen others consulted 72 hours later.
More than half of the patients (n= 22 cases, corresponding to 59.45%) consulted a dermatologist directly after the onset of symptoms, the other consulted other health facilities. They were examined either by a general practitioner in 7 cases, or by a cardiologist in 5 cases and a dentist in 1 case. The previous treatments used to treat an attack were first or secound generation antihistamines in 17 cases or 45.95%, general corticosteroids in 10 cases or 27.03%, paracetamol in 1 case or 2.7%, amoxicillin in 1 case or 2.7% and NSAIDs in 1 case or 2.7%. Some patients received several treatments concomitantly.
Different co-morbidities were pointed out in 23 cases, representing 62.15%. they consisted of personal atopy in 19 cases, standing for 51.35%, including asthma (n=4), allergic rhinitis (n=10), atopic dermatitis (n=2) and allergic conjunctivitis (n=3). Family atopy was found in 9 cases (24.32%). Diabetes was found in three patients (8.11%). Among these patients, two were treated with metformin while one was on a hypoglucidic diet. None of the patients had received gliptin, oral contraceptives or NSAIDs before the episode of angioedema. High blood pressure was noted in 6 patients (16.22%), 2 of whom were treated with perindopril, one with ramipril and furosemide, and the last with ramipril alone. We found that one patient had a probably systemic lupus, which was not followed up and not treated.
We did not find any family history of AE in our patients. Various triggering factors were identified in our patients: food in 13 cases (35.13%), combination of many factors in 2 patients. In 16 patients (43.24%), no triggering factor was f
Itching, with non-specidied characteristics, was found in 11 patiens. (29.73%) The distribution of patients according to the different functional signs is shown in Table 2. Pain intensity was assessed at 2 considering the Visual Analogue Scale.
Cardiovascular collapse was noted in 1 patient. Seven patients (18.92%) reported dyspnoea and/or dysphonia. The dyspnoea was mild and well tolerated by all patients.
superficial urticaria was found in 14 patients (37.84%). The oedema was the same colour as the skin, with variable and sometimes multiple locations, as in 14 patients (37.84%) (Figures 1,2,3 and 4). Mucosal involvement was also found (Figure 5). Table 3 shows the different locations according to their frequency.
Epicutaneous tests were carried out in 14 patients, corresponding to 37.84%, in whom we suspected an atopic condition. There were respiratory prick tests (to pneumallergens) which were positive in 13 patients. These results were consistent with the clinical data (existence of asthma, rhinitis or allergic conjunctivitis) in 8 cases, representing 21.62%.
The Trophallergen specific IgE assays were performed in 3 patients with suspected food allergy. It was positive in 2 patients, one for crab and the other for soy. The time between food intake and AE occurence could not be determined
A weighted C1-inh and C4 fraction of complement assay was performed in two patients and was unremarkable in both cases. In the case of the patient with systemic lupus, the C1-inhibitor assay could not be performed, and this could be angioedema due to acquired c1-inh deficiency
Among all included patients, there were 5 patients who presented an AE following a drug intake: ARAII (n=1) and angiotensin converting enzyme inhibitors (n=4). For the ARAII, the molecule responsible was losartan with a delay of 48h after intake.For angiotensine converting enzyme inhibitors, ramipril was the cause in 2 cases and perindopril in the other 2 cases, with an onset time of between 48 hours and 1 month after intake.
For the 32 other patients, it was a histaminergic AE, the etiology of which was specified in 19 cases, standing for 51.35%, but was only confirmed in 6 cases (16.21%). The diagnosis was made on the basis of allergological tests (prick tests, trophallergen assay) and the Therapeutics response to antihistamines . The etiology was not found in 13 cases (35.13%).
Treatment was prescribed in 26 patients (70.27%) for the management of AE. It was based on second-generation antihistamines alone per os in 11 cases for 7 to 10 days. Antihistamines were combined with short-term oral corticosteroids (betamethasone) in 13 cases or 35.13%.
In all cases of histaminergic AE, avoidance of the responsible agent was recommended. In the 5 cases of bradykinic AE, clinical monitoring and discontinuation of the suspected treatment were recommended. Tranexamic acid was prescribed in one patient. The clinical course was favourable in 30 patients, while the remaining 07 patients underwent recurrent AE attacks within one month of disease progression. In our study, there was a statistically significant relationship between the type of AE and urticaria (p = 0.0m). All cases of urticaria were in patients with histaminergic AE.
Discussion
To our knowledge, this is the firs study regarding angioedema conditions in Senegalese hospitals. During our study period, the prevalence of AE was estimated at 0.28%. This shows that it was a rare condition in black patients, in accordance with the liter ature. Indeed, this rarity had also been highlighted in cohorts of patients treated with ACE inhibitors by Nigerian authors [8]. This rarity seems to be in contradiction with studies conducted in the United States which reported a high frequency in Afri can-Americans. Nevertheless, African-Americans have been shown to have a higher proportion of SNPs (Single Nucleotide Polymorphism) in the AMPm (bradykinin-degrading) kininase gene compared to Caucasians [9].
According to Hacard et al [2] and Faisant et al [10], the incidence of AE in the general population has been estimated at 0.05%. In fact, the actual number of cases might be higher as some patients did not consult a doctor because of the spontaneous remission of AE. According to James et al [11], the frequency of AE is difficult to determine due to the paucity of clinical syudies on this conditions
A female predominance was noted in our series with a sex ratio od 0.6. This high female prevalence has been reported by Kulthanan et al [12] with a sex ratio of 0.28 and by Zingale et al [9] with a sex ratio of 0.64. It can be explained by the fact that women were more likely to consult for AE due to the added hor monal factor [13]
Our patients were relatively young, with a mean age of 38.51 years. The age group of 40-50 years was the most representative This result was similar to that found by Kulthanan et al [12] in Thailand (39.4 years). However, in theseries reported by Faisant et al [10] the mean age was higher at 50 years
For the consultation time, we found that it was less than 24 hours in 43.24% of cases (n=16). This could be ralated to the patient's embarrassment and anciaety during a first episode. On the other head for the same number of cases (n=16), the delay was more than 72 hours. We believe that this may be the group of patients who underwent previous self-remitted episodes of AE. We did not find a statiscally significant relationship between the time to consultation and the notion of "first epsiod". In seventeen patients (45.95%), this was the first first episode of angioedema.
The absence of a family history of AE in our patients seems consistent with the small sample size and the rarity of hereditary AE. Indeed, according to Du-Thanh et al, the prevalence of hereditary AE was estimated to be between 1/10,000 and 1/50,000 without ethnic predominance [14]. In South Africa, over a period of 6 years, only 60 cases of hereditary angioedema were reported [7].
Itching was the predoninant sign in our series. This may be explained by histamine release as histaminergic AE was the most common in our study.
In our study, 7 patients reported dyspnoea and/or dysphonia, which had regressed since the onset of the crisis. In fact, these signs could indicate laryngeal damage that could be life-threat ening [1,12]. We asked these patients to seek urgent medical at tention if such signs reappeared
Urticaria is considered a clinical feature of histaminergic AE and is usually absent in bradykinic-mediated AE [2,15-17]. However, this assumption has been recently overturned and it has been demonstrated that urticaria may be present in bradykinic-medi ated AE secondary to oestrogen [18].
The leading was allergy (32.43%), followed by pseudo-allergy (18.92%). In the literature, Boccon-Gibod et al [3] state that non-allergic AE is by far the most frequent. Therefore, our result needs to be confirmed by other studies with large sample size. The cause was not identified in 13 cases of histaminergic AE (40.63%). This is in agreement with the literature. Indeed, Kanani et al [19] found that the cause of histaminergic AE was unknown in 50%. However, we note that in our study, this result is explained by the lack of paraclinical explorations in these pa tients due to the high cost of the examination. For this reason, we preferred to assign the term "indeterminate cause" to these 13 cases of histaminergic AE.
After a 1-month follow-up, the evolution was favourable in 30 patients (81%). The other 7 cases underwent recurrent,AE at tacks at one months of the disease evolution. This was due to the absence of avoidance of the causative agent in 2 cases or to the failure to identify the causative agent in 5 cases. Indeed, the eviction measures seemed difficults to apply in certain situations. In the case of histaminergic AE, the majority of cases show a favourable evolutation after eviction of the causative agent agent and the use of anti-H1 drugs [2]. It should be noted that in the case of bradykinic-mediated AE, despite the Availability and affordability of tranxenamic acid, it was rarely prescribed by practitioners. This scarcity of prescription of this molecule could be due to a
Discussion
To our knowledge, this is the first study regarding angioedema conducted in Senegalese hospitals. During our study period, the prevalence of AE was estimated at 0.28%. This shows that it was a rare condition in black patients, in accordance with the liter ature. Indeed, this rarity had also been highlighted in cohorts of patients treated with ACE inhibitors by Nigerian authors [8]. This rarity seems to be in contradicition with studies conducted in the United States which reported a high frequency in Afri can-Americans. Nevertheless, African-Americans have been shown to have a higher proportion of SNPs (Single Nucleotide Polymorphism) in the AMPm (bradykinin-degrading) kininase gene compared to Caucasians [9].
According to Hacard et al [2] and Faisant et al [10], the incidence of AE in the general population has been estimated at 0.05%. In fact, the actual number of cases might be higher as some patients did not consult a doctor because of the spontaneous remission of AE. According to James et al [11], the frequency of AE is difficult ti determine due ro the paucity of clinical studies on this condition.
A female prodominance was noted in our series with a sex ratio of 0.6. The high female prevalence has been repored by Kulthanan et al [12] with a sex ratio of 0.28 and by Zingale et al [9] with a sex ratio of 0.64. It can be explained by the fact that women were more likely to consult for AE due to the added hor monal factor [13].
Our patients were relatively young, with a mean age of 38.51 years. The age group of 40-50 years was the most representative This result was similar to that founded by Kulthanan et al [12] in Thailand (39.4 years). However, in the series reported by Faisant et al [10], the mean age was higher at 50 years
For the consultation time, we found that it was less than 24 hours in 43.24% of cases (n=16). This could be ralated to the patients's embarrassment and anxiety during a first episode. On the other hand, for the same number of cases (n=16), the delay was more than 72 hours. We believe that this may be the group of patients who underwent previous self-remitted episodes of AE. We did not find a statistically significent relationship between the time to consultation and the notion of "first episode". In seventeen patients (45.95%), this was the first episode of angioedema.
The absence of a family history of AE in our patience seems consistent with the small sample size and the rarity of hereditary AE. Indeed, according to Du, Thanh et al, the prevalence of hereditary AE was estimated to be between 1/10,000 and 1/50,000 without ethnic predominance [14]. In South Africa, over a period of 6 years, only 60 cases of hereditary angioedema were reported [7].
Itching was the predominant sign in our series. This may be explained by histamine release as histaminergic AE was the most common in our study
In our study, 7 patients reported dyspnoea and/or dysphonia, which had regressed since the onset of the crisis. In fact, these signs could indicate laryngeal damage that could be life-threat ening [1,12]. We asked these patients to seek urgent medical at tention if such signs reappeared.
Urticaria is considered a clinical feature of histaminergic AE and is usually absent in bradykinic-mediated AE [2,15-17]. However, this assumption has been recently overturned and it has been demonstrated that urticaria may be present in bradykinic-medi ated AE secondary to oestrogen [18].
The leading was allergy (32.43%), followed by pseudo-allergy (18.92%). In the literature, Boccon-Gibod et al [3] state that non-allergitic AE non-allergic AE id by far the most frequent. Therefore, our result needs to be confirmed by other studies with large sample sizes. The cause was not identified in 13 cases of histaminergic AE (40.63%). This is in agreement with the literature. Indeed, Kanani et al [19] found that the cause of histaminergic AE was unknown in 50%. However, we note that in our study, this result is explained by the lack of paraclinical explorations in these pa tients due to the high cost of the examination. For this reason, we preferred to assign the term "indeterminate cause" to these 13 cases of histaminergic AE.
After a 1-month follow-up, the eveloution was favourable in 30 patients (81%). The other 7 cases underwent recurrent AE attracks at one month of the disease eveloution. This was due to the absence of avoidance of the causative agent in 2 cases or to the failure to identify the causative agent in 5 cases. Indeed, the eviction measures seemed difficults to apply in certain situtions. In the case of histaminergic AE, the majority of cases show a favourable eveolution after eviction of the causative agent and the use of anti-H1 drugs [2]. It should be noted that in the case of bradykinic-mediated AE,despited AE, despite the availability and affordability of tranxenamic acid, it was rarely prescribed by practitioners. Th9is scarcity of prescription of this molecule could be due to a lack of knowledge or to the fear of side effects, particularly vascular thrombosis
Conclusion
AE is a rare disease whose management must be known by all doctors but also by different medical and surgical specialties where it can be encountered (dermatology, cardiology, gy naecology, nephrology and endocrinology). In our study, we confirmed the rarity in hospitals, the predominance of women and the occurrence in middle-aged adults. Atopy was frequently found, the most frequent cause was histaminergic angioedema but angioedema suspected of bradykinic-mediated AE related to ACEI/sartans was also found. Antihistaminic drugs were the most frequently prescribed. The overall prognosis was favourable with rare cases of recurrence.
References
- Wuthrich B (2012) Angioedema: rarely of allergic origin [An gioedèmes: rarement d’origine allergique]. Forum Med Suisse 7: 138-43.
- Hacard F, Nosbaum A, Bensaid B, Nicolas JF, Augey F, et al. (2015) Histamine angioedema and chronic urticaria [An gio-œdème histaminique et urticaire chronique]. Presse Med 44: 37-42.
- Boccon-Gibod I, Bouillet L (2014) Angioedema in urticaria [Les angiœdèmes dans l’urticaire]. Ann Dermatol Venereol 141: S586-S595.
- Floccard B, Javaud N, Crozon J, Rimmelé T (2015) Emergen cy management of bradykinic angioedema [Prise en charge en urgence des angiœdèmes bradykiniques]. Presse Med 44: 70-7.
- Roskiewicz F, Andriamanana I, Gras-Champel V, Andrejak M, Massy ZA (2007) Iatrogenic angioedema: role of angiotensin converting enzyme inhibitors and angiotensin II receptor antag onists (sartans) [Angio-oedèmes iatrogènes : rôle des inhibiteurs de l’enzyme de conversion et des antagonistes des récepteurs à landiotensine II (sartans). Nephrol Ther 3:89-95
- Cicardi M, Aberer W, Banerji A, Bas M, Bernstein JA, et al. (2014) HAWK under the patronage of EAACI (European Acad emy of Allergy and Clinical Immunology). Allergy 69: 602-16.
- Wentzel N, Panieri A, Ayazi M, Ntshalintshali SD, Pourpak Z, et al. (2019) Fresh frozen plasma for on-demand hereditary angioedema treatment in South Africa and Iran. World Allergy Organ J 12: 100049.
- Ajayi AA, Adigun AQ (2000) Angioedema and cough in Ni gerian patients receiving ACE inhibitors. Br J Clin Pharmacol 50: 81-2.
- Zingale LC, Beltrami L, Zanichelli A, Maggioni L, Pappalardo E, et al. (2006) Angioedema without urticaria : a large clinical survey. CMAJ 175: 1065-70.
- Faisant C, Boccon-Gibod I, Mansard C, Dumestre Perard C, Pralong P, et al. (2016) Idiopathic histaminergic angioedema without wheals : a case series of 31 patients. Clin Exp Immunol 185: 81-5.
- James C, Bernstein JA (2017) Current and future therapies for the treatment of histamine-induced angioedema. Expert Opin Pharmacother 18: 253-62.
- Kulthanan K, Jiamton S, Boochangkool K, Jongjarearnpras ert K (2007) Angioedema: clinical and etiological aspects.Clin Dev Immunol 2007: 1-6.
- Bouillet L, Boccon-Gibod I, Massot C (2011) Hereditary or acquired bradykinic angioedemas [Les angioedèmes bradyki niques héréditaires ou acquis]. Rev Med Interne 32: 225-31.
- Du-Thanh A, Rainson Peyron N, Guillot B (2011) bradykinin angioedema [Les angioedèmes à bradykinine]. Ann Dermatol Venereol 138: 328-35.
- Coovadia KM, Chothia MY, Baker SG, Peter JG, Potter PC (2018) Hereditary angio-oedema in the Western Cape Province, South Africa. S Afr Med J 108: 283-90.
- Petitpierre S, Bart P-A, Spertini F, Leimgruber A (2008) Multiple etiologies of angioedema [Multiples étiologies de l’an giœdème]. Rev Med Suisse 4: 1030-8.
- Boccon-Gibod I (2012) Histamine or bradykinic urticaria/ angioedema? [Urticaire/angioedème histaminique ou bradyki nique?] Rev Fr Allergol 52: 327-332.
- Giard C, Nicolie B, Drouet M, Lefebvre-Lacoeuille C, Le Sel lin J, et al. (2012) Angio-oedema induced by oestrogen contra ceptives is mediated by bradykinin and is frequently associated with urticaria. Dermatology 225: 62-9.
- Kanani A, Schellenberg R, Warrington R (2011) Urticaria and angioedema. Allergy Asthma Clin Immunol 7: S9.
Artcle Information
Review Article
Received Date: May 02, 2025
Accepted Date: May 20, 2025
Published Date: May 27, 2025
Journal of Dermatology and Clinical Cosmetics
Volume 1 | Issue 1
Citation
Ly F, Ghorbel A, Ndiaye MB, Ndiaye Diop MT, Sarr SA, et al. (2025) Epidemiological, Clinical, Etiological and Therapeutic Aspects of Angioedema in Dakar, Semegal. J Derm and Clin Cosm 1: 103
Copyright
©2025 S Sofos. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jdcc.2025.1.103