

Review Article
Volume-1 Issue-1, 2024
Giant Duodenal Lipoma. A Case Report and Narrative Review of Published Cases and their Treatment Strategy
-
Received Date: July 02, 2025
-
Accepted Date: July 21, 2025
-
Published Date: July 28, 2025
Journal Information
Abstract
Background: Duodenal lipoma is a rare benign tumour. Only 4% of all gastrointestinal lipomas are found in the duodenum causing a wide range of vague abdominal symptoms, intussusception or bleeding. Diagnosis is easily made during endoscopic ultrasound or computed tomography. There are no clear treatment guidelines or recommendations available.
Results: We present a case of a 79-year-old male with anorexia, nausea and unintentional weight loss due to a duodenal lipoma. The duodenal lipoma was resected via laparotomy and duodenotomy with primary closure of the duodenum. A literature review was performed for all English reported cases treated surgically or endoscopically from 2001 until 2024 using PubMed (N= 75). Clinical presentation and lesion characteristics are important in choosing a treatment strategy. Literature suggests treating all symptomatic duodenal lipomas, whereas watchful waiting can be a valid option in asymptomatic patients. Multiple surgical and endoscopic treatment options are available.
Conclusion: Minimally invasive techniques should be considered first since duodenal lipoma is a benign disease. Patient characteristics and spatial features (location, size, number) are determining in the selection of the right treatment modality. Treatment needs to be tailored to each patient.
Key words
Lipoma, Duodenum, Digestive System Surgical Procedures, Endoscopy
List of Abbreviations
CT: Computed Tomography; D2: Second part of the duodenum; EUS: Endoscopic Ultra Sonography; HU: Houssndsfield Unit; MRI: Magnetic Resonance Imaging; ESD: Endoscopic Submucosal Dissection; EFTR: Endoscopic Full Thickness Resection; LECS: Laparoscopic Endoscopic Collaborative Surgery; PSD: Pancreas Sparing Duodenectomy
| Reference | Gender | Age (y) | Symptoms | Histology | Morphology | Size (mm) | Location | Treatment | |
| 1 | Chung-Fang Tung et al. (2001) | M | 73 | Tarry stools, Anemia (Hb 7,8g/dL) | Lipoma, Superficial ulceration | Single,Pedunculated | 45 | D2 | Endoscopic electrosurgical SNARE polypectomy |
| 2 | L. Lundell et al. (2002) | M | 44 | Obstructive jaundice, gastric outlet obstruction | Lipoma | Giant multiple lipoma | - | D2 D3 D4 Jejunum | Surgery: Laparotomy, Pancreas-sparing duodenectomy |
| 3 | Suketo Sou et al. (2003) | Fhybr | 81 | Massive melena, Anemia (Hb 6,2g/dL) | Lipoma, ulceration at tip | Single, Pedunculated | 50 | D3 | Endoscopic electrosurgical SNARE polypectomy |
| 4 | Marie-Cécile Blanchet et al. (2003) | F | 69 | Nausea, vomiting, abdominal pain, weight loss | Lipoma | Single, lobulated polypoid | 50 | D2 | Endoscopic electrosurgical SNARE polypectomy |
| 5 | Saleh N Abu Daff et al. (2008) | F | 53 | Vomiting, abdominal discomfort | Lipoma | - | - | - | Surgery: Laparoscopic enucleation, duodenotomy |
| 6 | Wen-Hsin Huang et al. (2008) | M | 46 | Upper abdominal fullness after eating | Lipoma | Single | 20 | D1 | Endoscopic endoloop-assisted unroofing technique |
| 7 | F | 75 | Postprandial discomfort | Lipoma | Single, polypoid | 20 | D2 | Endoscopic endoloop-assisted unroofing technique | |
| 8 | DRC Spalding et al. (2007) | F | 71 | Gastric outlet obstruction | Lipoma | Single | - | D3-D4 | Surgery: Laparotomy, Pancreas-sparing distal duodenectomy |
| 9 | Billy W. Long et al. (2008) | - | - | Upper gastrointestinal haemorrhage | Lipoma | Single | 40 | D3 | Endoscopic polypectomy |
| 10 | Harish K. Mohamed et al. (2008) | F | 70 | Upper gastrointestinal haemorrhage | Lipoma | Single | 55 | D2 | Endoscopic polypectomy |
| 11 | Atsuhiko Murata et al. (2008) | M | 67 | Recurrent tarry stools, anemia | Lipoma | Single, pedunculated | 40 | D2 | Endoscopic polypectomy with detachable SNARE |
| 12 | Haley Clifford et al. (2009) | M | 70 | Melena | Lipoma | Single, pedunculated | - | - | Endoscopic endoloop and SNARE polypectomy |
| 13 | Cheng-Wang Chang et al. (2010) | F | 59 | Melena, abdominal distention, palpitation, anemia (Hb 8,2g/dL) | Lipoma, ulcer at tip | Single, pedunculated | 40 | D2 | Surgery: laparotomy, duodenotomy |
| 14 | Helga M. Ouwerkerk et al. (2010) | F | 52 | Melena, abdominal distention, vomitus | Lipoma | Single | 17 | D1 | Surgery: laparotomy, Duodenotomy |
| 15 | R. Kadaba et al. (2011) | F | 60 | Fatigue, tiredness, generally unwell, anaemia (Hb 6,5g/dL) | Lipoma | Single | 60 | D1 | Surgery: duodenotomy, transduodenal resection in the submucosal plane, not further specified |
| 16 | Dianbo Cao et al. (2011) | F | 68 | Melena, weight loss | Lipoma, ectopic duodenal glands | Single, polypoid | 40 | D2 | Surgery: laparotomy, technique not specified |
| 17 | Jelena Djokie Kovac et al. (2012) | M | 65 | Vomiting, epigastric pain, postprandial fullness | Lipomas | Multiple, polypoid | 10, 25 | D1, D2 | Surgery: laparotomy, technique not specified |
| 18 | Tae Hee Lee et al. (2013) | F | 57 | Intermittent upper abdominal pain | Lipoma | Single, polypoid | - | - | Endoscopic electrocautery SNARE |
| 19 | Amit Kumar Parmar et al. (2013) | F | 43 | Postprandial abdominal fullness, nausea, vomiting | Lipoma | Single | 60 | D1 | Surgery: Laparoscopic excision, longitudinal duodenotomy |
| 20 | Promise N Wichendu et al. (2013) | M | 40 | Projectile vomiting, epigastric fullness, constipation, abdominal discomfort | Lipoma | Single, pedunculated | 110 | D2 | Surgery: Exploratory laparotomy, duodenotomy |
| 21 | Henrik Thorlacius et al. (2013) | M | 66 | Fatigue, acute upper gastrointestinal bleeding (Hb 9,2 g/dL), melena | Lipoma, ulcerations | Single, polypoid | 35 | D2 | Endoscopic endoloop and SNARE |
| 22 | Ismail Yaman et al. (2014) | F | 59 | Upper abdominal fullness, heartburn, anemia (Hb 9,7g/dL) | Lipoma | Single, polypoid | 40 | D2 | Endoscopic SNARE polypectomy |
| 23 | Fatih Aslan et al. (2014) | M | 77 | Nausea, vomiting, dyspepsia | Lipoma | Single | 90 | Duodenum, extending to antrum | Endoscopic submucosal dissection (ESD) |
| 24 | Downs-Canner et al. (2015) | - | - | - | Lipoma | - | - | Duodenum | Robotic surgery (Transduodenal excision / Segmental duodenal resection) |
| 25 | - | - | - | Lipoma | - | - | Duodenum | Robotic surgery (Transduodenal excision / Segmental duodenal resection) | |
| 26 | Nizar Talaat et al. (2016) | M | 79 | Darkening urine, itching, scleral icterus | Lipoma | Single | - | Gastro-duodenal | NO resection: Endoscopic placement of 10x60mm fully covered metal stent |
| 27 | Dinesh Zirpe et al. (2016) | M | 45 | Melena, anemia (Hb 8g/dL) | Lipoma, ulcerations | Multiple, polypoid | 40 | D3/D4, proximal jejunum | Surgery: Laparotomy, duodenectomy (2cm distal to ampulla) and proximal jejunum, side-to-side duodenojejunostomy |
| 28 | Chuncheng Wu et al. (2017) | F | 64 | Postprandial abdominal discomfort, intermittent melena, symptomatic anemia (Hb 9,0g/dL) | Lipoma | Single | 100 | D2 | Endoscopic submucosal dissection (ESD) |
| 29 | Alberto Mariani et al. (2017) | M | 70 | Jaundice | Lipoma | Single | 15 | D2 | NO resection. |
| 30 | Maowei Pei et al. (2017) | F | 67 | Abdominal pain, vomiting, constipation, epigastric fullness | Lipoma | Multiple | 13 - 110 | D2/D3/D4, proximal jejunum | Surgery: Exploratory laparotomy, duodenectomy (4cm distal to ampulla, proximal jejunum, end-to-end duodenojejunal hand-sewn anastomosis) |
| 31 | Taro Iwatsubo et al. (2017) | M | 70-79 | - | Tubular adenoma, lipoma beneath | Single | 30 | D2 | Hybrid: Laparoscopic endoscopic cooperative surgery (LECS), first endoscopic submucosal dissection, en bloc resection, laparoscopic suturing of mucosal defect from outside the duodenum |
| 32 | Viviana Parra et al. (2018) | M | 63 | Chronic abdominal pain, intermittent postprandial vomiting | Lipoma | Single | - | D2 | Endoscopic Modified SNARE polypectomy |
| 33 | Ankush Golhar et al. (2018) | F | 70 | Upper gastrointestinal bleed | Lipoma | Single | 110 | D3 | Surgery: Laparotomy, Segmental duodenectomy, duodenojejunostomy |
| 34 | Mohammadreza Shervinrad et al. (2019) | M | 75 | Vomiting, anorexia, unintentional weight loss, Anemia (Hb 10,0 g/dL) | Lipoma | Multi-lobed | 60, 70, 115 | D1-D2 | Surgery: Partial duodenal resection, access not further specified |
| 35 | Hung Chieh Lan et al. (2018) | F | 65 | Occult gastrointestinal bleeding, anemia | Lipoma | Single, pedunculated | 27 | D1 | Endoscopic SNARE polypectomy |
| 36 | Douglas Tjandra et al. (2019) | F | 68 | Melena, upper abdominal pain, intussusception with lipoma D1 as leading point | Lipoma | Single, pedunculated | 105 | D1 | Surgery: Laparoscopy, duodenotomy and primary repair |
| 37 | Yasunori Yoshimoto et al. (2019) | F | 47 | Abdominal pain, medical history of open bowel resection for intestinal obstruction caused by intussusception of multiple intestinal lipoma | Lipoma | Multiple | 20 | Duodenum, jejunum until distal ileum | Hybrid: Diagnostic laparoscopy, converted to open laparotomy, resection of each palpated intestinal lipoma. Duodenal lipoma was resected by endoscopic submucosal dissection (ESD). |
| 38 | Seo Yeon Gwak et al. (2020, Epub 2019) | F | 85 | Hematemesis, nausea, vomiting | Lipoma, ulcerations | Single | 20 | D1 | Endoscopic resection using SNARE |
| 39 | Karthik Gnanapandithan et al. (2020) | F | 55 | Postprandial epigastric fullness | Lipoma | Single, broad based | 50 | D1 | Endoscopic endoloop ligation, SNARE |
| 40 | Hisamichi Yoshii et al. (2020) | M | 72 | Melena, anemia (Hb 6,0g/dL) | Lipoma, mucosal ulceration | Single, sessile | 40 | D2 | Surgery: Laparoscopy, pancreassparing partial duodenectomy, Roux-en-Y reconstruction |
| - | Yuichiro Ozeki et al. (2020) | M | 60 | - | Hyperplasia Brunner’s Glands | Single | 35 | D2 | Endoscopic electrosurgical SNARE, with hemoclip anchoring at head of lipoma |
| 41 | F | 50 | - | Lipoma | Single | 30 | D3 | Endoscopic electrosurgical SNARE, with hembrotoclip anchoring at head of lipoma | |
| 42 | Marouane Baiss et al. (2021) | M | 58 | Melena, anemie (Hb 7,8g/dL) | Lipoma | Single | 100 | D1 | Surgery: Laparotomy, longitudinal duodenotomy |
| 43 | Logan D. Glosser et al. (2021) | F | 53 | Constipation, anoreia | Lipoma | Single | - | D3 | Robot assisted laparoscopic excision via transverse duodenotomy |
| - | Bin Yang et al. (2021) 23 patients | 12 M11 F | 8 symptomatic patients | Depending on relation to muscularis propria layer.Endoscopic submucosal dissection: ESDEndoscopic full thickness resection: EFTR | |||||
| 44 | M | 41 | Melena | Lipoma | - | 22 | D1 | ESD | |
| 45 | M | 61 | Epigastric pain | Lipoma | - | 23 | D2 | ESD | |
| 46 | F | 69 | Epigastric pain | Lipoma | - | 22 | D2 | ESD | |
| 47 | M | 62 | Patient desires resection | Lipoma | - | 22 | D2 | ESD | |
| 48 | M | 28 | Patient desires resection | Lipoma | - | 25 | D2 | EFTR | |
| 49 | M | 62 | Patient desires resection | Lipoma | - | 21 | D2 | ESD | |
| 50 | F | 70 | Patient desires resection | Lipoma | - | 30 | D2 | ESD | |
| 51 | M | 70 | Epigastric pain | Lipoma | - | 23 | D2 | ESD | |
| 52 | M | 72 | Melena | Lipoma | - | 60 | D2 | ESD | |
| 53 | F | 49 | Patient desires resection | Lipoma | - | 75 | D1 | EFTR | |
| 54 | F | 49 | Epigastric pain | Lipoma | - | 20 | D2 | ESD | |
| 55 | F | 42 | Patient desires resection | Lipoma | - | 40 | D2 | ESD | |
| 56 | F | 44 | Patient desires resection | Lipoma | - | 23 | D2 | ESD | |
| 57 | M | 67 | Patient desires resection | Lipoma | - | 24 | D2 | ESD | |
| 58 | M | 55 | Patient desires resection | Lipoma | - | 25 | D2 | ESD | |
| 59 | F | 65 | Patient desires resection | Lipoma | - | 30 | D2 | ESD | |
| 60 | F | 58 | Epigastric pain | Lipoma | - | 28 | D1 | EFTR | |
| 61 | F | 52 | Patient desires resection | Lipoma | - | 23 | D2 | ESD | |
| 62 | F | 73 | Patient desires resection | Lipoma | - | 25 | D1 | ESD | |
| 63 | M | 64 | Patient desires resection | Lipoma | - | 21 | D2 | ESD | |
| 64 | M | 73 | Patient desires resection | Lipoma | - | 24 | D1 | ESD | |
| 65 | F | 47 | Epigastric pain | Lipoma | - | 22 | D2 | ESD | |
| 66 | F | 42 | Patient desires resection | Lipoma | - | 26 | D2 | EFTR | |
| 67 | Beom Jin Shin et al. (2021) | F | 78 | Asymptomatic | Lipoma and Brunner Gland hyperplasia in 1 polypoid lesion | Single, Pedunculated polyp with erosions | 35 | D2 | Endoscopic SNARE polypectomy |
| 68 | Shimura Takaya et al (2021) | F | 53 | Recurrent pancreatitis | Lipoma | Single, Pedunculated with stalk originating from para-ampulla of Vater | 60 | D2 | Hybrid: Endoscopic submucosal dissection, laparoscopic removal of specimen from jejunum |
| 69 | Branko Brankovic et al. (2022) | M | 45 | Upper gastro intestinal bleeding, Melena, Anemia (Hb 8,5g/dL) | Lipoma | Single | 35 | - | Surgery: Laparotomy, duodenotomy and excision |
| 70 | Mohammed I. Mousa et al. (2023) | F | 49 | Abdominal pain, melena | Lipoma | Single, pedunculated | 23 | D1 | Endoscopic SNARE resection |
| 71 | Ryan Alghanemi et al. (2023) | M | 67 | Weight loss, night sweats, constipation, postprandial fullness | Lipoma | Single | 74 | D1 | Robotic assisted duodenotomy, excision |
| 72 | Kazuya Miyaguchi et al. (2023) | F | 50 | Upper abdominal pain, melena, symptomatic anemia (Hb 6,6g/dL) | Composite tumor: lipoma combined with gastric-type NUMP | Single, pedunculated, erosions | 30 | D2 | Endoscopic resection |
| 73 | Isabel Tarrio et al. (2023) | M | 82 | Jaundice | Lipoma | Single, pedunculated | 20-30 | - | Endoscopic SNARE resection |
| 74 | Carl Cosgrave et al. (2023) | M | 73 | Syncope and melena with need for transfusion | Lipoma | Single, pedunculated | 65 | D2 | Endoscopic SNARE resection |
| 75 | Manish Sahni et al. (2024) | M | 15 | Jaundice, intermittent upper gastrointestinal bleeding | Lipoma | Sessile | 70 | D2, Ampulla | Surgery: Laparotomy, duodenotomy with excision and plastic repair sphincter of Oddi (pancreas preserving) |
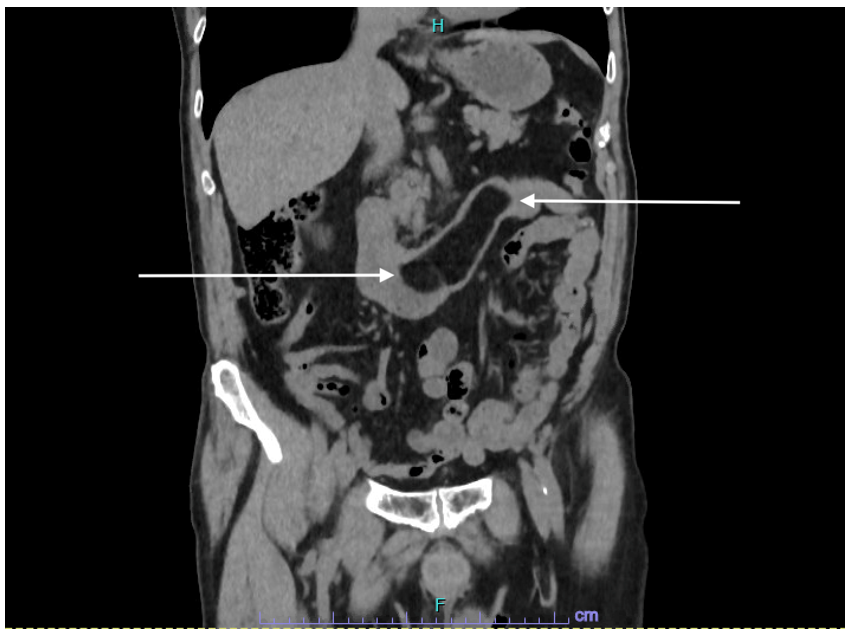 |
| Figure 1: Computed tomography of the abdomen - coronal section. The mass at the level of the duodenum measures -120 to -90 HU representing a duodenal lipoma, indicated with arrows |
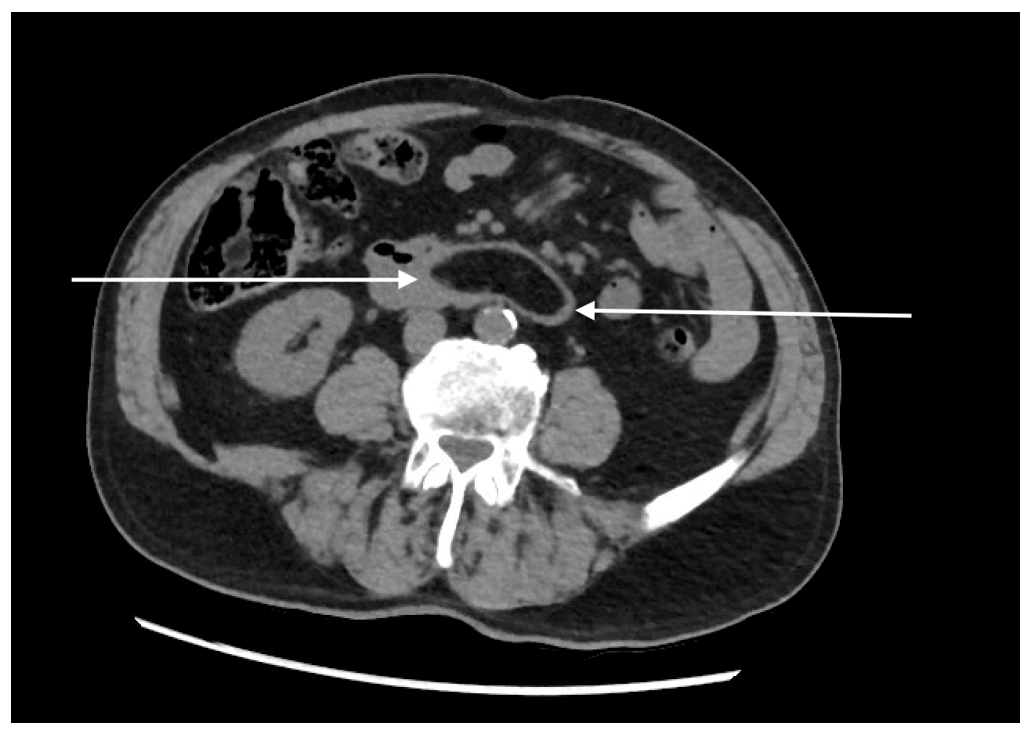 |
| Figure 2: Computed tomography of the abdomen - transverse section. Duodenal lipoma is indicated with arrows |
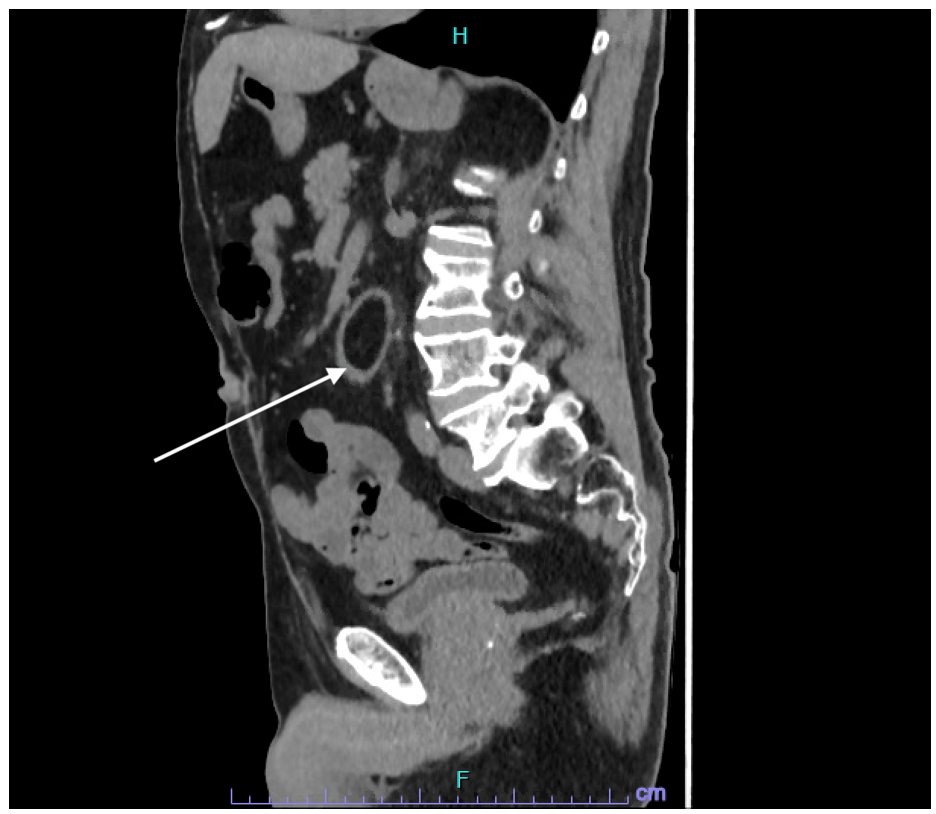 |
| Figure 3: Computed tomography of the abdomen- sagittal section. Duodenal lipoma is indicated with an arrow |
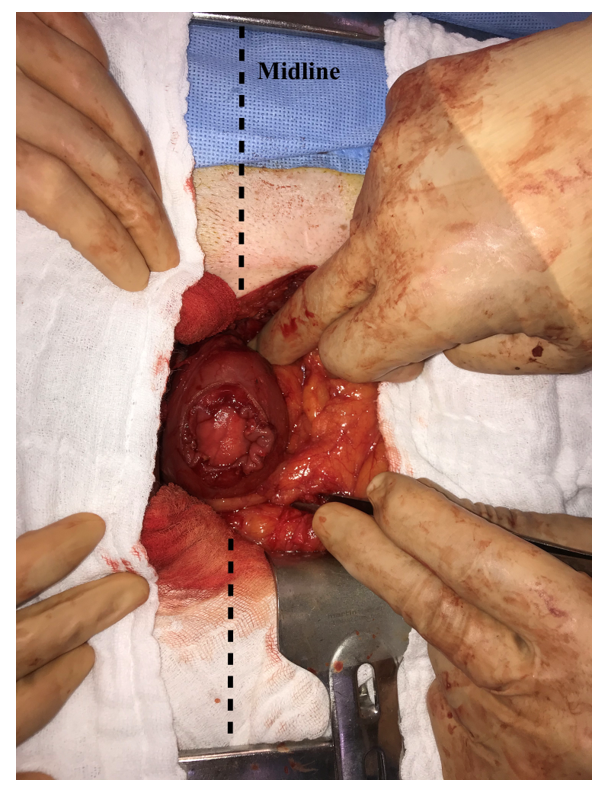 |
| Figure 4: Operative photo: Redo upper abdomen midline laparotomy. A longitudinal incision of the anterior aspect of the second part of the duodenum revealing a submucosal, yellowish mass originating from the posterior wall |
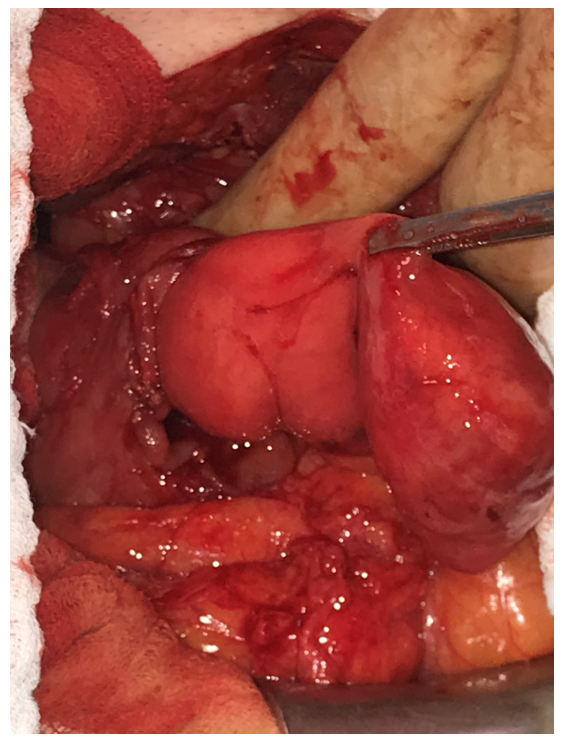 |
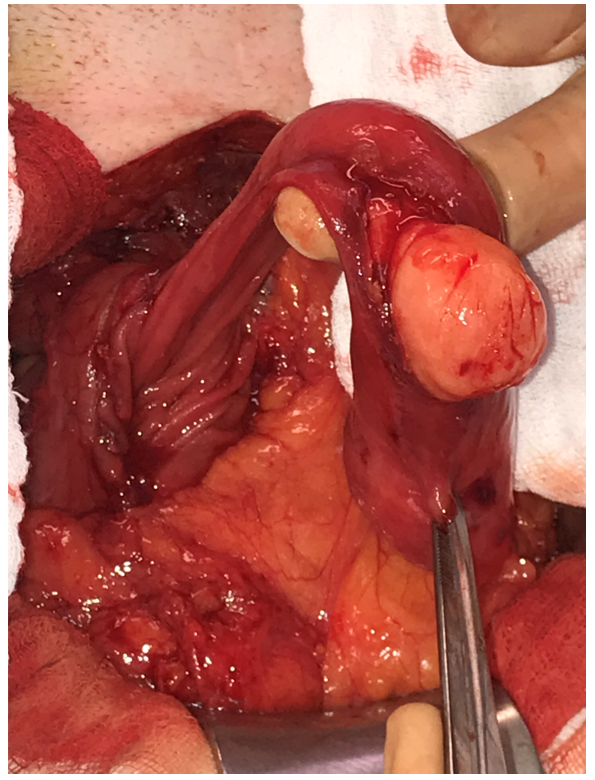
| Figure 5: Operative photo. Duodenal lipoma presenting itself as a large pedunculated mass, which was luxated easily through the longitudinal duodenotomy |
 |
| Figure 6: Operative photo. The overlying normal mucosa was incised, revealing a well-defined submucosal lipoma |
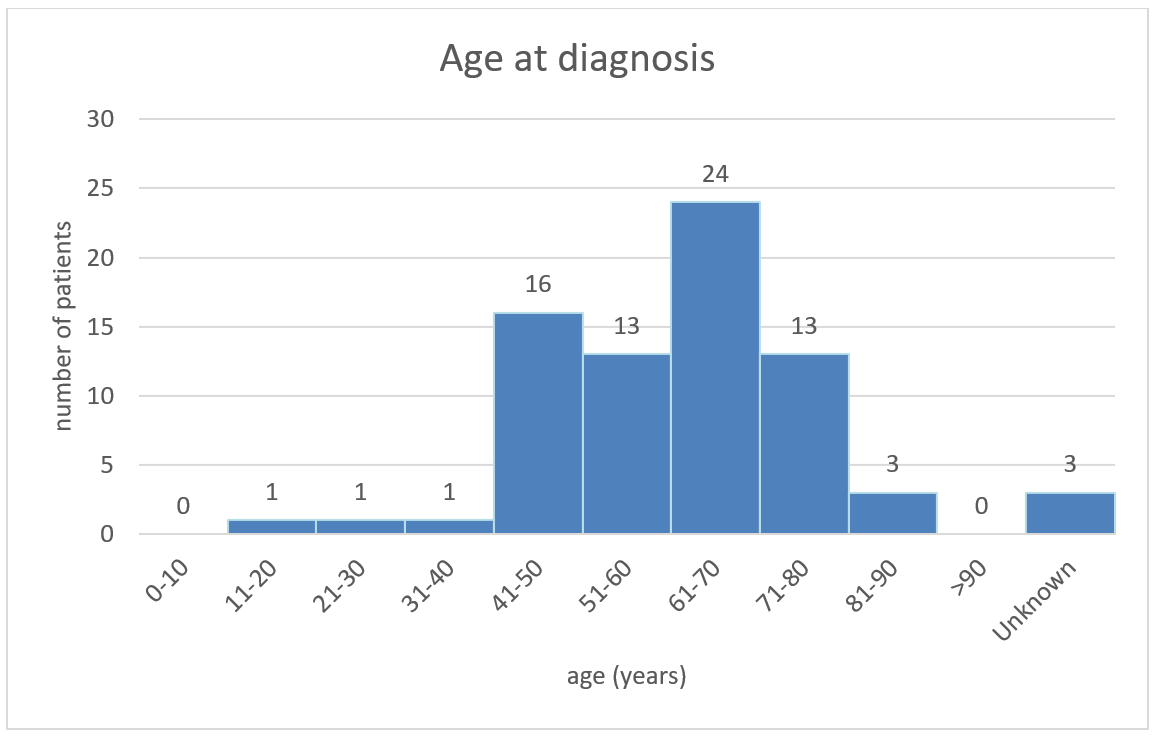 |
| Figure 7: Plot showing the number of patients diagnosed with duodenal lipoma in each age category per 10 years, with a total number of patients n=75, including 3 patients of unknown age and no reported cases older than 85 years |
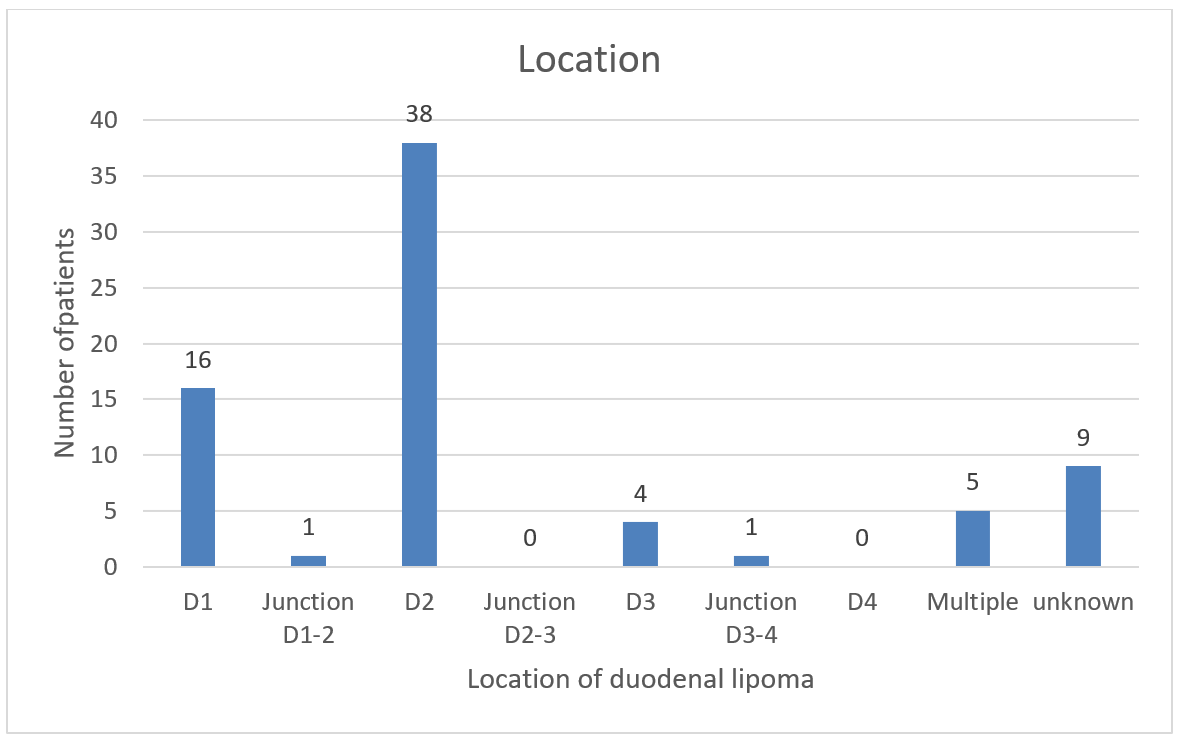 |
| Figure 8: Anatomical location of all reported duodenal lipoma. D1: first segment of duodenum, D2: second part of duodenum, D3: third part of duodenum, D4: fourth part of duodenum |
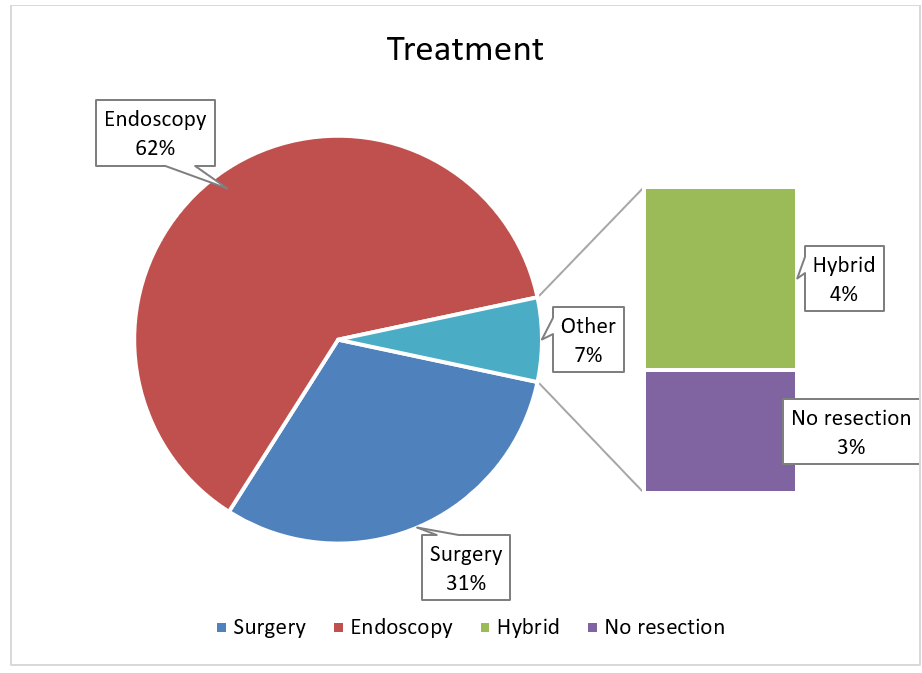 |
| Figure 9: Diagram showing all different treatment modalities in English published cases from 2001 until may 2024 |
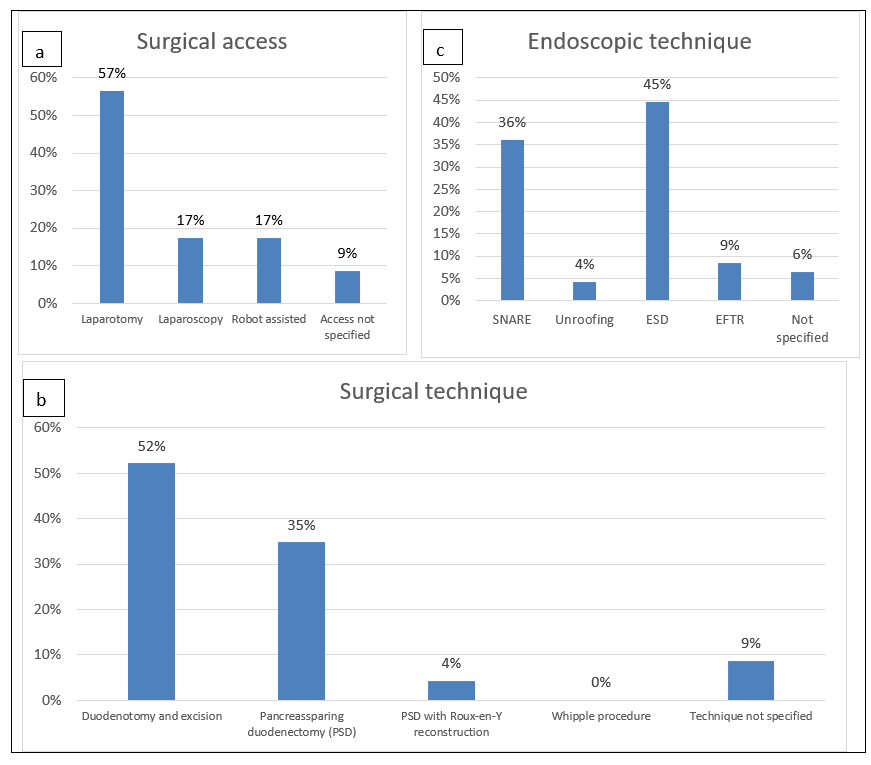 |
| Figure 10: Treatment options for duodenal lipoma. a: Surgical access, b: Surgical techniques, c: Endoscopic options for resection. PSD: pancreas sparing duodenectomy, ESD: Endoscopic submucosal dissection, EFTR: Endoscopic full thickness resection |
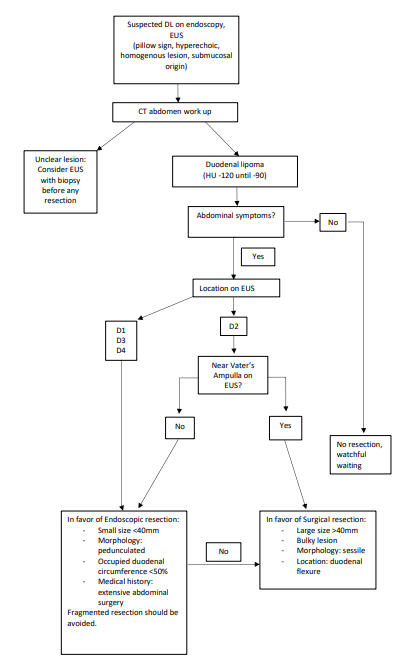 |
| Figure 11: Flow chart with proposed practical guidelines for the management of duodenal lipoma in daily practice. DL: Duodenal lipoma; EUS: Endoscopic ultra-sonography; D1: first part of duodenum; D2: second part of duodenum; D3: third part of duodenum; D4: fourth part of duodenum |
Introduction
A lipoma is a benign, adipose tumour that can appear throughout the whole gastrointestinal tract. Most commonly, they are found at the level of the colon (64%), ileum and jejunum (26%). Only 4% of all gastrointestinal lipomas are found in the duodenum. They present as a single and slow-growing tumour and are most often found in the second part of the duodenum or descending duodenum [1]. It is a neoplasm of mesenchymal origin. Other mesenchymal tumours include leiomyomas, leiomyoblastomas, haemangiomas, fibroids, neurofibroma-like tumours, schwannomas, gangliomas and lymphangiomas [2]. Duodenal lipoma can present itself as a sessile or a pedunculated mass, often incidentally diagnosed on endoscopy, computed tomography (CT) or during surgery.
Small lipomas (diameter < 2 cm) tend to be asymptomatic. When exceeding a diameter of 2 cm, it can cause a wide range of vague symptoms and therefore an easily missed diagnosis in daily practice. Epigastric pain, fullness, nausea, vomiting, obstruction and rarely intussusception have been described [1,3-7]. Gastrointestinal tract bleeding can occur from overlying ulcerated mucosa, causing anemia and melena or occult gastrointestinal bleeding [3,8-16]. Rare symptoms are obstructive jaundice and pancreatitis [17,18].
To our knowledge, there are no clear guidelines concerning the treatment of duodenal lipoma. Our aim was to review possible treatment strategies since we encountered a patient with a symptomatic giant duodenal lipoma ourselves. Therefore, a literature search on PubMed was performed for published cases of duodenal lipoma and their treatment strategy. All case reports published in English from 2001 until 2024 were included (table 1).
Case Report
A 79-year-old male patient presented with anorexia, nausea, unintentional weight loss of 2 kg and constipation. There is a medical history of splenectomy, rectal adenocarcinoma (pT3N0M0, Dukes b) treated with open total mesorectal excision and few years later an incisional hernia treated with open ventral hernia mesh repair. Active medication included calcium channel blockers. Upon clinical examination, there was no recurrence of the ventral hernia. Upper gastrointestinal endoscopy showed an extensive submucosal mass in the second part of the duodenum, easily passable with a scope, over a length of 10 cm, suggestive of a duodenal lipoma.
Computed tomography (CT) of the abdomen confirmed the presence of a duodenal lipoma extending from the 2nd to 4th part of the duodenum, measuring 95 mm x 30 mm (Figure 1 - 3).
Due to his surgical history, laparoscopy was not found to be a safe surgical approach. We performed a redo midline, upper abdomen, laparotomy. After extensive adhesiolysis and identification of the Treitz ligament, no mass could be palpated at this level. Proceeding with mobilization of the duodenum by performing the Kocher manoeuvre, a large mass could be palpated in the descending part of the duodenum(D2). Longitudinal duodenotomy at the level of D2 revealed a pedunculated mass originating from the posterior wall of the duodenum (Figure 4-6).
Resection was performed using a powered stapler (EchelonTM flex 60 mm), positioned at the base of the stalk of this pedunculated mass after luxating it through the duodenotomy and checking for safe distance from Vater’s ampulla. After primary transverse closure of the duodenotomy, a Blake drain was placed alongside the duodenum.
The postoperative period was uneventful. Upper gastrointestinal contrast series on the third postoperative day showed no signs of contrast leakage, normal duodenal appearance and stomach emptying. Oral intake was resumed, and the drain was removed successfully. The patient was discharged home on day 6.
Histopathological diagnosis confirmed a submucosal lipoma with no signs of malignancy. At the one-month post surgery follow-up, the patient had no residual complaints of nausea, good oral intake without any postprandial discomfort and a stable body weight.
Materials and Methods
There are no clear guidelines concerning the treatment of duodenal lipoma to our knowledge. Our aim was to review possible treatment strategies since we encountered a patient with a symptomatic giant duodenal lipoma for the first time.
A literature review was performed using the search term “duodenal lipoma” in PubMed. This search generated 157 articles published from 2001 until May 2024, of which 51 case reports of duodenal lipoma published in English and 2 retrospective studies. The retrospective study by Yang et al. was included since all patient characteristics and treatment details were available per individual patient. Xiang et al. did not provide individual information and thus was not included in our review. Case reports of gastric and jejunal lipoma were excluded.
Results
We included 51 case reports and one retrospective study representing 75 patients diagnosed with duodenal lipoma over a time span of 24 years (table 1). There were five cases of multiple lipomas; 44 patients were diagnosed with a single lipoma, of which one was multilobulated, two case reports and the retrospective study by Yang et al. did not mention specific spatial information (26 patients). The size varied between 10 mm and 115 mm. Twenty-three patients were treated surgically of which 4 robot-assisted procedures. Three cases described a combined surgical and endoscopic approach [19-21]. Forty-seven patients were treated endoscopically. In two patients the lipoma was not resected. One case report by Mariani et al. reporting a duodenal lipoma obstructing a biliary stent which was not resected and in the case reported by Talaat et al. stenting of the common bile duct for obstructive jaundice was preferred over resection of the duodenal lipoma [17,18].
One retrospective study was published in 2021 by Yang et al. comparing endoscopic submucosal dissection (ESD) and endoscopic full thickness resection (EFTR) depending on how the lesion was relating to the muscularis propria layer on endoscopic ultrasound.
The literature search showed only one systematic review by Pei et al. discussing all published cases of duodenal lipoma from 1948 until 2016 in addition to their own encountered patient with duodenal lipoma [22]. There are no clinical trials or meta-analysis published.
Discussion
From 2001 until 2024, the majority of reported cases (24 patients, 32%) including all patients of a retrospective study by Yang et al. were diagnosed with duodenal lipoma in their 7th decade of life. We found no diagnosis before the age of 15 or above the age of 85 (table 1, figure 7). Thirty-eight female (51%) and thirty-four male (45%) patients were diagnosed, 2 case reports (3 patients, 4%) did not mention patient gender or age. The majority of lipoma were found in the second part of the duodenum (figure 8).
Symptoms
Duodenal lipoma can cause vague abdominal symptoms such as epigastric fullness and postprandial discomfort. Unintentional weight loss, gastric outlet obstruction with nausea and (projectile) vomiting are also reported. Intussusception is described with the lipoma acting as the leading point causing duodeno-duodenal intussusception [7].
Symptoms of upper gastrointestinal bleeding (hematemesis, melena, anemia, fatigue) can be associated because of ulceration of the overlying mucosa, often seen upon endoscopy. Some rare symptoms, such as obstructive jaundice and (recurrent)pancreatitis, have been described in 3 case reports [17,18,20].
Large lipomas tend to cause symptoms more often, whereas small lipomas are frequently found by coincidence on CT scan, during endoscopy or intraoperatively. The literature review by Pei et al. stated that 80% of symptomatic lipomas have a diameter of >2 cm [22]. Other authors mention that lipomas <1 cm are usually asymptomatic and lipomas of> 4 cm are more likely to cause obstruction, intussusception or bleeding [2]. The cut-off diameter for large or giant lipoma differs depending on the author.
Diagnosis
Duodenal lipomas are often found by accident during endoscopy and endoscopic ultrasonography (EUS). They have a characteristic appearance because of their fat content and their submucosal location in the enteric wall. During endoscopy a lipoma can appear as a round yellowish elevated lesion. A positive ‘Pillow sign’, consisting of a visible indentation when palpating the lesion with closed forceps, is described as a typical endoscopic feature for a lipoma [23]. Characteristic presentation during EUS consists of an intense, homogeneous, hyperechoic lesion originating from the submucosa [23,24]. Endoscopy with EUS is the most accurate imaging modality for morphological features (sessile, pedunculated) and defining the exact location of the lipoma establishing its distance to the ampulla of Vater. These features are determining in selecting the right treatment option.
Differential diagnosis consists of other hyperechoic lesions, e.g. renal cell carcinoma metastasis, ampullary carcinoma, hamartomatous duodenal polyp and gangliocytic paraganglioma[25]. Other duodenal lesions to keep in mind are gastrointestinal stromal tumours, carcinoids, solitary Peutz-Jeghers polyp and adenoma [23]. Yang et al. describes a possible risk of malignancy especially when the duodenal lipoma exceeds 5cm, referring to the UK guidelines for management of soft tissue sarcoma’s [26,27]. Reviewing these guidelines ourselves we found no specific statements on visceral or duodenal lipoma in particular. Gaspar et al. and the systematic review by Pei et al. report no malignant transformation [22,23].
Computed tomography (CT) has grown in popularity for diagnostic purposes in the last decade. Lipomas are easily and reliably identified on CT because of their appearance as a smooth margined mass combined with a characteristic low uniform (fat density) attenuation with a low Hounsfield Unit (HU) count from -70 to -120 HU [28-30].
Combining information from EUS and CT, the diagnosis of duodenal lipoma can easily be confirmed because of its characteristic features on both imaging modalities. When the diagnosis remains uncertain, EUS with biopsy is an option to differentiate from possible malignant lesions.
In addition, lipomas have specific characteristics on magnetic resonance imaging (MRI). They show a high signal intensity on a T1-weighted image and an iso-signal intensity on T2-weighted images [30,31].
Treatment
Duodenal lipomas come in different sizes and shapes, as do their treatment options. The majority of patients was treated endoscopically (62%), 31% was treated surgically and 4% underwent a hybrid treatment strategy combining both (figure 9). Important features to consider are size, location in the duodenum (relation to the ampulla of Vater) and patient-specific characteristics. The most determining factor is clinical presentation. Lipoma is a lesion of benign nature. In the retrospective study by Yang et al, the authors are concerned about possible malignancy whereas the systematic review by Pei et al. state that malignant change of duodenal lipoma is unheard of and they consider these lesions as benign [22,26]. We found no reports of malignancy or malignant deterioration of duodenal lipoma from 2001 until present.
Given its benign nature, treatment is recommended when patients are symptomatic. A pedunculated duodenal lipoma lends itself to endoscopic management when not too bulky. Large and sessile lipomas are often better managed with surgical intervention.
The majority of patients (47 patients; 62%) were treated endoscopically (figure 10). This high number can partially be explained by the included retrospective study which only reviewed endoscopic treated patients in their hospital. In this study a remarkedly large number of asymptomatic patients were treated claiming resection of the lipoma was the patients’ wish (8 patients). Several endoscopic techniques are described: SNARE polypectomy (17 patients), unroofing technique (2 patients), endoscopic submucosal dissection (ESD, 21 patients) and endoscopic full thickness resection (EFTR, 4 patients). For three patients the endoscopic technique was not specified. In 36% of all endoscopic treated patients, the SNARE technique using a two-channel scope was used. One channel is used for the introduction of an electrocautery snare, and the other channel for grasping forceps pulling the lipoma through the loop of the [4,8,12,15,16,32-42]. The unroofing technique used in 2 patients (4% of all endoscopic treated patients) consisted of cutting the upper half of the lipoma and extruding the remaining adipose tissue from this open surface. It is considered a simple technique with minimal risk of perforation. The main disadvantage is the fragmented resection [24,43]. Yang et al. compares the use of ESD to endoscopic full resection (EFTR), choosing EFTR when the lesion was near the muscularis propria layer. In those patients the nearby muscularis propria and serosa were also resected, closing the defect in the duodenal wall with purse-string sutures using endoloops and clips. This technique is accompanied with the need for pneumoperitoneum desufflation during and after procedure and a gastro-intestinal tube was left behind at level of the resection site. Hospital stay in this study was rather long for both techniques from 5 days until 16 days hospital stay which is longer than the hospital stay of our patient treated with open surgical excision [26].
The most used endoscopic technique, accounting for 21 patients (45% of all endoscopic treated patients) is the endoscopic submucosal dissection (ESD) frequently mentioned as the preferred approach for resection. With increasing lipoma diameter, the endoscopic intervention becomes increasingly challenging with a higher risk of perforation and more fragmentated tissue for histo-pathological examination. Another large disadvantage is the long intervention time reported up to 4 hours in this literature search. Therefore, this technique is not suitable for every patient nor every lesion [19,26,44,45].
Two case reports did not resect the duodenal lipoma causing obstructive jaundice. One lipoma was lifted out of a present biliary stent with the tip of the endoscope without resection[18]. In the second case, endoscopic bare metal stenting was preferred to treat the jaundice without resection of the responsible lipoma [17].
Surgical management was described in 23 patients (31%). Surgical access options are laparotomy (13 patients) or minimally invasive via laparoscopy (4 patients) or robot-assisted surgery as described in 4 patients (figure 10). The access was not specified in two patients.
Different useful surgical techniques are duodenotomy with excision/enucleation of the lipoma and primary closure (12 patients), a pancreas sparing duodenectomy (PSD) with end-to-end or side-to-side duodenojejunostomy (8 patients), PSD with the need for Roux-en-Y reconstruction (1 patient) and Whipple procedure (no reported cases) all summarized in figure 10 [1,5-7,10,11,13,14,31,46–58]. The resection technique was not further specified in two patients [31,55]. Three patients underwent a hybrid approach combining endoscopy and surgical techniques. One patient had multiple intestinal lipomas resected via laparotomy with resection of each palpated (jejunal) lipoma combined with ESD for the one duodenal lipoma[19]. One patient was treated with ESD but needed laparoscopic removal of the specimen [20]. And one patient underwent a hybrid laparoscopic endoscopic collaborative surgery (LECS) procedure in which ESD was performed with en bloc resection of the lipoma followed by laparoscopic suturing of a mucosal defect [21].
Based on reviewed literature we propose a practical flow-chart useful in daily practice when encountering a patient with duodenal lipoma (figure 11). When large and bulky, surgical excision is a more appropriate course of action. No clear cut-off diameter is established in the literature from which surgery is preferred over endoscopic resection. Several authors describe large lipoma as being too difficult for endoscopic resection, especially when located in D2 and near Vaters’ ampulla. The systematic review by Mao Wei Pei et al. (2017) mentions large and sessile lesions as difficult to manage endoscopically because of the increasing risk of perforation and bleeding with increasing lesion size, but a size cut off favoring surgical treatment was not discussed. Kato Motohiko et al.(2019) published a retrospective study identifying lesion size >40mm, lesion location in duodenal flexure and occupied circumference >50% as characteristics associated with technical difficulties during ESD. [59] Therefore 40mm could be a possible size cut-off from which surgery should be considered over endoscopic treatment. Criteria in favor of surgery are location near Vater’s ampulla, sessile and large lipoma and no clear diagnosis of benign nature since endoscopic resection often results in fragmented and sometimes incomplete resection. Future research is needed to establishing a clear size cut-off from which surgery is preferred over endoscopic management. This could result in more evidence-based guidelines supporting gastroenterologist and surgeons in daily practice.
Laparoscopic and robotic approaches are technically feasible and have been described in several cases. Patient history and location of the lipoma in the duodenum are important factors in determining if your patient can be considered for minimally invasive surgery.
In our case, laparotomy was preferred given the patients’ surgical history and extensive adhesions were to be expected. Additionally, the duodenal lipoma was located at the posterior wall of the descending duodenum, a location difficult to access laparoscopically.
Several good treatment options and techniques have been described for symptomatic duodenal lipoma. In summary, there is endoscopy (SNARE, unroofing technique, ESD, EFTR), laparoscopy and laparotomy (duodenotomy with excision/enucleation, PSD with or without Roux-en-Y reconstruction), robotic assisted procedures and hybrid approach.
There is a need for larger studies with long term follow up of patients to assess outcomes of all the different treatment modalities. This will contribute to more evidence-based guidelines concerning the management of duodenal lipoma to better support and guide gastroenterologists and abdominal surgeons when encountering this rare pathology in their daily practice.
Conclusion
Duodenal lipoma is a difficult and rare diagnosis. Therefore, it is important to keep this benign tumour in mind when investigating a patient with vague abdominal, nonspecific complaints.
A CT scan and MRI can confirm the diagnosis based on the imaging characteristics of a lipoma but are less accurate in exact localization. Endoscopic ultrasound is more accurate in determining the precise location of the duodenal lipoma in relation to Vaters’ ampulla and evaluating its morphology and spatial features (sessile, pedunculated).
Dealing with a benign disease, always consider the least invasive technique seen fit for each patient. Watchful waiting is considered a safe option for asymptomatic duodenal lipoma. When symptomatic, excision is recommended endoscopically or surgically depending on the characteristics of the patient and the lesion.
The best treatment option is the technique most suited for your specific patient taken medical history and characteristics of the lipoma into account. Spatial characteristics of the lipoma such as size, morphology and location, are important factors in determining the appropriate treatment access and technique.
There are no treatment guidelines available. Individual assessment is needed but clear evidence-based guidelines are mandatory in further improving the care for patients diagnosed with duodenal lipoma. Therefor larger studies are needed, assessing long-term outcomes of all different treatment strategies, contributing to evidence-based guidelines.
Acknowledgements
Not applicable
Declarations
No funding was received for this article. The authors report there are no competing interests to declare. The patient gave consent for publication.
All data generated or analysed during this study are included in this published article and its supplementary information files.
Author Contributions
Potums L. acted as writer of the original draft of the article, performing the literature search and review included.
Huysentruyt F., D’hooge P. and Delvaux P. were major contributors throughout the writing and re-writing process of the manuscript, proofreading and help in re-writing the discussion section.
All the authors have read and approved the final manuscript.
Appendix – Additional information
References
- Pei M, Hu M, Chen W, Qin C (2017) Multiple Duodenal Lipomas as a Rare Cause of Upper Gastrointestinal Obstruction: Case Report and Literature Review. Gastroenterol Res. 10: 149–52.
- Latos W, Kawczyk-Krupka A, Strzelczyk N, Sieroń A, Cieślar G (2019) Benign and non-neoplastic tumours of the duodenum. Gastroenterol Rev. 14: 233-41.
- Long BW, Goodwin E, Halford P, Almas J (2008) Diagnosis and endoscopic resection of a bleeding duodenal lipoma. J Miss State Med Assoc. 49: 3–6.
- Blanchet MC, Arnal E, Paparel P, Grima F, Voiglio EJ, Caillot JL (2003) Obstructive duodenal lipoma successfully treated by endoscopic polypectomy. Gastrointest Endosc. 58: 938–9.
- Parmar AK, Bibyan M, Khandelwal R, Reddy PK (2013) Laparoscopic Management of a Large Duodenal Lipoma Presented as Gastric Outlet Obstruction. J Soc Laparoendosc Surg. 17: 459–62.
- Wichendu PN, Dodiyi-Manuel A. Gastric outlet obstruction from duodenal lipoma in an adult. Niger J Surg. 19: 79–81.
- Shervinrad M, Salem RR, Zhang X (2019) Giant Duodenal Lipoma: a Rare Cause of Vomiting, Anorexia, Unintentional Weight Loss, and Duodenal Intussusception. J Gastrointest Cancer. 50: 693–4.
- Sou S, Nomura H, Takaki Y, Nagahama T, Matsubara F, Matsui T, et al. (2006) Hemorrhagic duodenal lipoma managed by endoscopic resection. J Gastroenterol Hepatol. 21: 479–81.
- Mohammed HK, Suresh CC, Alexander KG, Neena M (2008) Bleeding duodenal lipoma treated with endoscopic polypectomy. Trop Gastroenterol. 29: 167–8.
- Ouwerkerk HM, Raber MH, Freling G, Klaase JM (2010) Duodenal Lipoma as a Rare Cause of Upper Gastrointestinal Bleeding. Gastroenterol Res. 3: 290–2.
- Kadaba R, Bowers KA, Wijesuriya N, Preston SL, Bray GB, Kocher HM (2011) An Unusual Cause of Gastrointestinal Bleeding: Duodenal Lipoma. Case Rep Gastroenterol. 5: 183–8.
- Thorlacius H, Weiber H, Ljungberg O, Nielsen J, Toth E (2013) Endoscopic diagnosis and treatment of a giant duodenal lipoma presenting with gastrointestinal bleeding. Endoscopy. 45: E385–6.
- Zirpe D, Wani M, Tiwari P, Ramaswamy PK, Kumar RP (2016) Duodenal Lipomatosis as a Curious Cause of Upper Gastrointestinal Bleed: A Report with Review of Literature. J Clin Diagn Res. 10: PE0-5.
- Yoshii H, Izumi H, Tajiri T, Mukai M, Nomura E, Makuuchi H (2020) Surgical Resection for Hemorrhagic Duodenal Lipoma: A Case Report. Tokai J Exp Clin Med. 45: 75–80.
- Tung CF, Chow WK, Peng YC, Chen GH, Yang DY, Kwan PC (2001) Bleeding duodenal lipoma successfully treated with endoscopic polypectomy. Gastrointest Endosc. 54: 116–7.
- Clifford H, Lui M, Lee R, Thomson A (2009) A finger in the duodenum. Med J Aust. 191: 691.
- Talaat N, Malenie R, Raina A (2016) An Unusual Case of Obstructive Jaundice Owing to an Extrabiliary Mass. Gastroenterology. 151: e8–9.
- Mariani A, Archibugi L, Petrone MC, Arcidiacono PG (2017) An unusual cause of biliary metal stent obstruction. Dig Liver Dis. 49: 1283.
- Yoshimoto Y, Yoshida T, Fujikawa T, Shirai Y, Yamamoto T (2019) Novel surgical approach without bowel resection for multiple gastrointestinal lipomatosis: A case report. Int J Surg Case Rep. 59: 54–7.
- Shimura T, Okubo T, Okuda Y, Iwasaki H, Katano T, Kato A, et al. (2022) Endoscopic submucosal dissection followed by laparoscopic collection of a giant duodenal lipoma causing repeated pancreatitis. Endoscopy. 54: E346–7.
- Iwatsubo T, Takeuchi Y, Yamasaki Y (2017) Duodenal adenoma overlying a lipoma treated with laparoscopic endoscopic collaborative surgery. Dig Endosc. 29: 812–3.
- Pei MW, Hu MR, Chen WB, Qin C (2017) Diagnosis and Treatment of Duodenal Lipoma: A Systematic Review and a Case Report. J Clin Diagn Res. 11: PE01–5.
- Gaspar JP, Stelow EB, Wang AY (2016) Approach to the endoscopic resection of duodenal lesions. World J Gastroenterol. 22: 600–17.
- Lee TH, Kim WJ (2013) A duodenal lipoma with a long stalk. Korean J Intern Med. 28: 383.
- Figueiredo PC, Pinto-Marquez P, Mendonca E, Oliveira P, Brito M, Serra D (2013) Duodenal subepithelial hyperechoic lesions of the third layer: Not always a lipoma. World J Gastrointest Endosc. 5: 514–8.
- Yang B, Jiang F, Lu P, Han H (2021) Minimally invasive management of large duodenal lipoma: endoscopic submucosal dissection. J Int Med Res. 49: 01–11.
- Dangoor A, Seddon B, Gerrand C, Grimer R, Whelan J, Judson I (2016) UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res. 6: 20.
- Jayaraman MV, Mayo-Smith WW, Movson JS, Dupuy DE, Wallach MT (2001) CT of the Duodenum: An Overlooked Segment Gets Its Due. Radio Graphics. 21: S147–60.
- Kakitsubata Y, Kakitsubata S, Nagatomo H, Mitsuo H, Yamada H, Watanabe K (1993) CT Manifestations of lipomas of the small intestine and colon. Clin Imaging. 17: 179–82.
- Genchellac H, Demir MK, Ozdemir H, Unlu E, Temizoz O (2008) Computed Tomographic and Magnetic Resonance Imaging Findings of Asymptomatic Intra-Abdominal Gastrointestinal System Lipomas: J Comput Assist Tomogr. 32: 841–7.
- Kovač JD, Dunjić MK, Bjelović M, Banko B, Lilić G, Milenković R, et al. (2012) Magnetic resonance imaging features of multiple duodenal lipomas: a rare cause of intestinal obstruction. Jpn J Radiol. 30: 676–9.
- Hung CL, Tseng-Shing C (2018) A rare cause of occult gastrointestinal bleeding. Dig Liver Dis. 50: 620.
- Parra V, Preciado J, Huertas M, Acero F, Aponte D, Sabbagh L (2017) Low-cost technique for resection of a large duodenal lipoma with the aid of a modified polypectomy snare. Endoscopy. 50: s-0043-120265.
- Yaman I, Derici H, Paksoy S (2014) Symptomatic duodenal lipoma with endoscopic snare polypectomy. Turk J Surg. 30: 103–5.
- Murata A, Osoegawa T, Ijyu M, Kanayama K, Tanaka M, Nakamura K (2008) Pedunculated duodenal lipoma treated with endoscopic polypectomy with a detechable snare. Fukuoka Igaku Zasshi. 99: 131–5.
- Gwak SY, Lee MK, Lee YK (2020) A Case of a Bleeding Duodenal Lipoma Successfully Controlled by Endoscopic Resection. Clin Endosc. 53: 236–40.
- Gnanapandithan K, Aslanian HR, Jamidar PA, Muniraj T (2020) Endoscopic Resection of a Giant Duodenal Lipoma. ACG Case Rep J. 7: e00327.
- Ozeki Y, Hirasawa K, Sato C (2020) Useful endoscopic resection technique for large pedunculated lesions in the duodenum using thread‐traction method with a double‐channel endoscope. Dig Endosc. 32: e22–3.
- Shim BJ, Park SK, Park HU, Park TY (2022) Enteritis cystica profunda with lipoma in the second portion of the duodenum: a case report. J Yeungnam Med Sci. 39: 72–6.
- Mousa MI, Al Ghamdi SS, Alsolmi AA, Fakhri AF (2023) Duodenal Lipoma As Upper Gastrointestinal Bleeding Presentation: Case Report and Review of the Literature. Cureus. 15: e33996.
- Tarrio I, Andrade AJ, Moreira M, Lopez L (2023) Duodenal lipoma - An unusual finding, location and presentation. Rev Esp Enferm Dig.
- Cosgrave C, Abbas S, Alexander S (2023) Large bleeding duodenal lipoma. Gastrointest Endosc. S0016-5107: 03195–4.
- Huang WH, Peng CY, Yu CJ, Chou JW, Feng CL (2008) Endoloop-assisted unroofing for the treatment of symptomatic duodenal lipomas. Gastrointest Endosc. 68: 1234–6.
- Aslan F, Akpinar Z, Cekic C, Alper E (2015) En bloc resection of a 9cm giant gastro-duodenal lipoma by endoscopic submucosal dissection. Dig Liver Dis. 47: 88–9.
- Wu C, Yang JF, Tan Q, Zhang Q, Hu B (2017) En bloc resection of a large symptomatic duodenal lipoma by endoscopic submucosal dissection. Video GIE. 2: 182–4.
- Lundell L, Hyltander A, Liedman B (2002) Pancreas-sparing Duodenectomy: Technique and Indications. Eur J Surg. 168: 74–7.
- Sahni M, Daga R, Jangir N, Singh S, Sharma R (2024) Management of a Rare Challenging Case of Duodenal Ampullary Lipoma. Indian J Surg Oncol. 15: S322–4.
- brankovic B, Stanojevkc G, Nestorovic M, Dencic T, Milutinovic N (2022) Unusual cause of upper gastrointestinal bleeding. Report of the case of hemorrhagic duodenal lipoma with review of the literature. Ann Ital Chir. 11: S2239253X22038014.
- Alghanemi R, Tekin Z (2023) Duodenal lipoma: robotic-assisted approach. J Surg Case Rep. 5: 1–2.
- Glosser LD, Lombardi CV, Knauss HM, Hopper W, Alalwan A, Stanek S (2021) Treatment of duodenal lipoma with robotic-assisted transverse duodenotomy: A case report of novel approach. Int J Surg Case Rep. 86: 106366.
- Baiss M, Rahali A, Hicham EM, Mdaghri J, Lahlou K, Mssrouri R, et al. (2021) Giant duodenal lipoma: an unusual cause of gastrointestinal bleeding ‘case report’. Pan Afr Med J. 38.
- Tjandra D, Knowles B, Simkin P, Kranz S, Metz A (2019) Duodenal Lipoma Causing Intussusception and Gastric Outlet Obstruction. ACG Case Rep J. 6: e00157.
- Golhar A, Mangla V, Mehrotra S, Lalwani S, Mehta N, Nundy S (2018) Limited distal duodenal resection: Surgical approach and outcomes. A case series. Ann Med Surg. 30: 36–41.
- Downs-Canner S, Van Der Vliet WJ, Thoolen SJJ, Boone BA, Zureikat AH, Hogg ME, et al. (2015) Robotic Surgery for Benign Duodenal Tumors. J Gastrointest Surg. 19: 306–12.
- Cao D, Sun X, Du J, Sun Y (2011) Duodenal Lipoma Associated with Ectopic Duodenal Glands. Clin Pract. 1: e128.
- Chang CW, Chu CH, Shih SC, Chen MJ, Yang TL, Chang WH (2010) Duodenal polypoid lipoma with bleeding. Am J Surg. 200: e49–50.
- Spalding D, Isla A, Thompson J, Williamson R (2007) Pancreas-Sparing Distal Duodenectomy for Infrapapillary Neoplasms. Ann R Coll Surg Engl. 89: 130–5.
- Abu Daff SN, Abu Daff NS (2008) Laparoscopic enucleation of a duodenal lipoma, with review of the literature. Saudi Med J. 29: 455–7.
- Kato M, Sasaki M, Mizutani M, Tsutsumi K, Kiguchi Y, Akimoto T, et al. (2019) Predictors of technical difficulty with duodenal ESD. Endosc Int Open. 07: E1755–60.
Article Information
Review Article
Received Date: July 02, 2025
Accepted Date: July 21, 2025
Published Date: July 28, 2025
Giant Duodenal Lipoma. A Case Report and Narrative Review of Published Cases and their Treatment Strategy
Volume 1 | Issue 1
Citation
Lieselot Potums, Frederik Huysentruyt, Pieter D’hooge, Peter Delvaux (2025) Giant Duodenal Lipoma. A Case Report and Narrative Review of Published Cases and their Treatment Strategy. Eur J Gastroenterol Digestive Dis 1: 104
Copyright
©2025 Lieselot Potum. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jgdd.2025.1.104