

Research
Volume-1 Issue-2, 2025
Clinical Study of the Predictive Value of Serum HBV RNA Plus Hbcrag for the Progression of Liver Fibrosis in Patients with HBV DNA-Negative Chronic Hepatitis B
-
Received Date: August 05, 2025
-
Accepted Date: August 24, 2025
-
Published Date: August 31, 2025
Journal Information
Switch to Full Text Menu
Abstract
Objective: Serum hepatitis B virus RNA (HBV RNA) and hepatitis B core-related antigen (HBcrAg) reflect hepatic covalently closed circular DNA (cccDNA) levels and correlate with liver fibrosis severity. However, single serum markers are susceptible to various confounding factors and lack standardized detection methods, resulting in inconsistent research findings. This study aimed to elucidate the correlation between serum HBV RNA, HBcrAg, and liver fibrosis in HBV DNA-negative chronic hepatitis B patients, determine the predictive value of their combined dynamic changes for fibrosis progression, and assess the efficacy of dual-antibody therapy (antiviral plus antifibrotic) using these markers.
Methods: Sera from 372 patients meeting the inclusion criteria were analyzed. Liver fibrosis stages (mild, moderate, severe) were determined using the FIB-4 index and 2019 Chinese Guidelines for the Prevention and Treatment of Chronic Hepatitis B. Patients were further categorized into two treatment groups: a dual-antibody group (antiviral plus antifibrotic) and a monoclonal antibody (mAb) group (antiviral only). Baseline data and serum HBV RNA (qRT-PCR) and HBcrAg (ELISA) levels were recorded at baseline, 12 weeks, and 24 weeks. Liver stiffness measurement (LSM) values were also obtained.
Results: Baseline liver function tests differed significantly between fibrosis stages (p <0.05). Pearson and Spearman correlation analyses revealed a positive association between serum HBV RNA and LSM values in both HBeAg-positive (r=0.388, p=0.028) and HBeAg-negative patients (r=0.228, p=0.042). A positive correlation between serum HBcrAg and LSM was observed only in HBeAg-positive patients (r=0.289, p=0.087). Multiple linear regression analysis showed no association between serum HBV RNA and age, ALT, AST, GGT, TBIL, DBIL, or HBsAg; however, HBsAg correlated linearly with serum HBcrAg. ROC curve analysis demonstrated that serum HBV RNA and HBcrAg were more effective in predicting severe fibrosis, particularly in HBeAg-positive patients (combined AUC=0.869), exceeding the predictive value of individual markers. After 24 weeks, no significant differences were observed in serum HBV RNA, HBcrAg, or LSM values between the two treatment groups across fibrosis stages.
Conclusion: Serum HBV RNA showed a positive correlation with liver fibrosis, while serum HBcrAg demonstrated a partial positive correlation, primarily in HBeAg-positive patients. The combined use of serum HBV RNA and HBcrAg exhibited superior diagnostic efficacy for severe liver fibrosis compared to single markers. Twenty-four weeks of follow-up revealed no significant treatment effect difference between the dual-antibody and mAb groups.
Key words
Chronic Hepatitis B, Serum HBV RNA, Serum Hbcrag, Predictive Value
| s | Mild group | Moderate group | Heavy group | P |
| Gender (Male / Female) | (180/111) | (37/18) | (14/9) | 0.621 |
| Age (year) | 55 (47,64) | 60 (51,66) | 56.9±12,2 | 0.104 |
| ALT (U /L) | 19.6 (14.5,26.2) | 19.7 (15.3,34.3) | 23.2 (19.3,30.6) | 0.074 |
| AST (U /L) | 23.6 (20.8,27.5) | 28.8 (23.8,34.1) | 32.7 (25.3,44.1) | <0.001 |
| GGT (U /L) | 16.8 (12.2,24.1) | 25.1 (18.6,48.2) | 39.9 (22.8,68.1) | <0.001 |
| TBIL (µm ol/L) | 14.8 (12.1,18.2) | 16.3 (13.3,19.7) | 18.2 (16.2,25.2) | 0.001 |
| DBIL (µm ol/L) | 4.2(3.4,5.0) | 4.9 (4.1,6.3) | 5.9 (4.8,8.9) | <0.001 |
| Negative Group, HBVRNA | Negative Group, HBcrAg | Positive Group, HBVRNA | Positive Group, HBcrAg | |
| R | 0.228 | -0.002 | 0.388 | 0.289 |
| P | 0.042 | 0.984 | 0.028 | 0.087 |
| Base Line | 12 Weeks | 24 Weeks | ||
| HBV RNA | 72.22 (28.34, 2974.50) | 117 (24.13, 1558.28) | 141 (12.09, 28.84) | |
| p | 0.91 | 0.897 | ||
| HBcrAg | 0.31 (0.27, 0.44) | 0.36 (0.30, 0.40) | 0.29 (0.25, 0.35) | |
| p | 0.443 | 0.027 | ||
| LSM price | 6.6 (5.5, 10.325) | 7.6 (5.775, 10.00) | 8.3(5.95, 12.55) | |
| p | 0.449 | 0.778 | ||
 |
| Figure 1: HBV RNA regression coefficient estimation results and regression equation of variance analysis table |
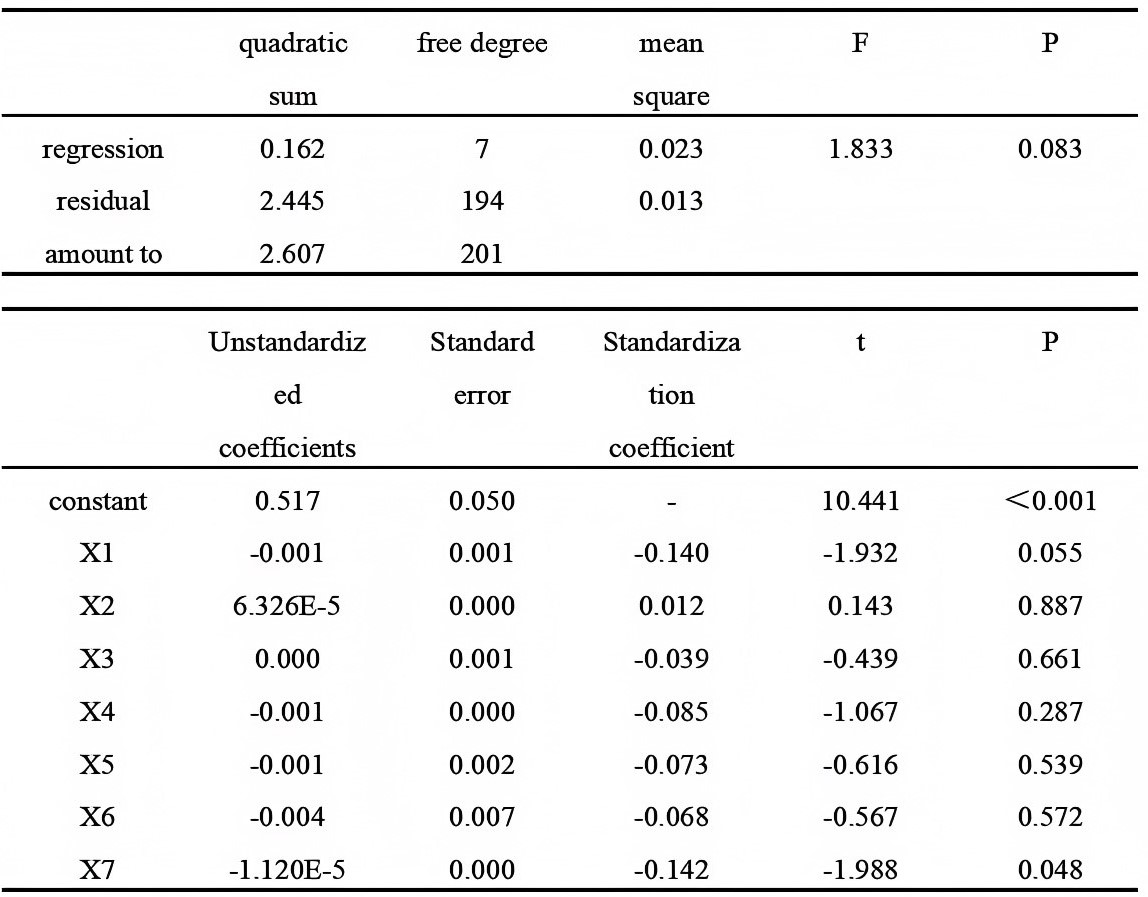 |
| Figure 2: HBcrAg regression coefficient estimation results and regression equation of variance analysis table |
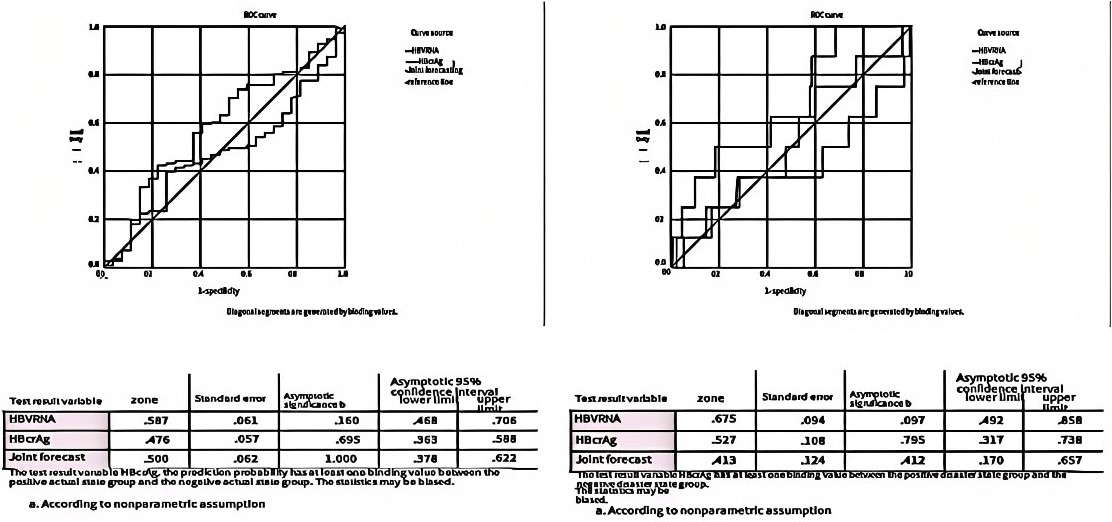 |
| Figure 3: e antigen-negative mild liver fibrosis (left) and e antigen-positive mild liver fibrosis (right) |
 |
| Figure 4: e antigen negative moderate liver fibrosis (left) and e antigen neutral mild liver fibrosis (right) |
 |
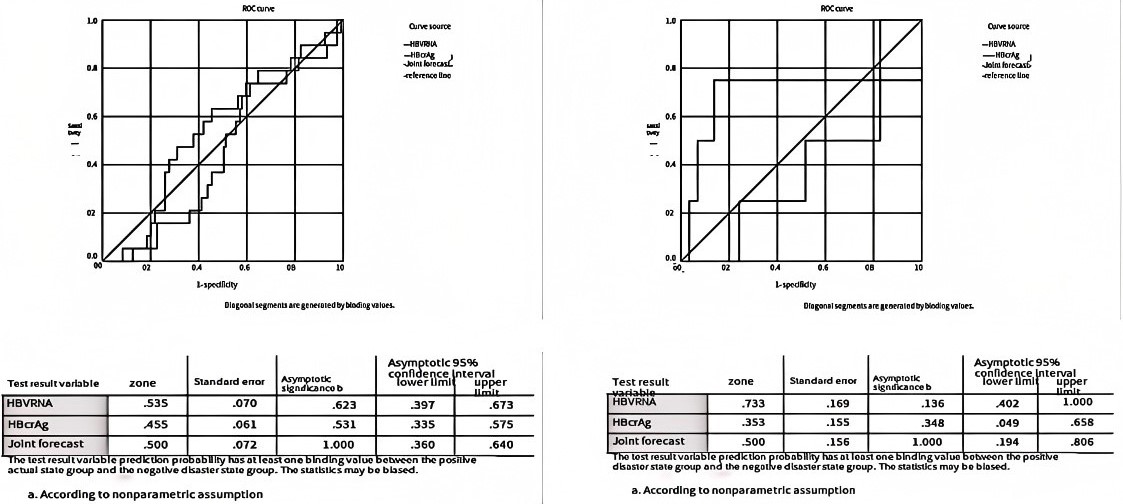
| Figure 5: e antigen negative severe liver fibrosis (left) and e antigen heavy mild liver fibrosis (right) |
Introduction
Chronic hepatitis B (CHB) is a chronic liver inflammatory disease caused by the persistent infection of hepatitis B virus, which can lead to the occurrence of liver cirrhosis and even liver cancer. According to statistics, the prevalence rate of HBsAg in China is now about 6% [1], About 30 million patients with chronic hepatitis B. Due to the unique genomic and replication form of HBV, current drugs are difficult to completely remove intrahepatic covalently closed circular DNA (cccDNA), which is the main reason for the progression of liver fibrosis after antiviral therapy in CHB patients [2]. Therefore, it is important to clarify the cccDNA level in the liver to clarify clinical issues such as the progression of hepatitis liver fibrosis and the efficacy of antifibrotic drugs. However, the detection of cccDNA in the liver depends on the invasive examination of liver puncture, which is difficult to be popularized and applied in clinical practice. It is urgent to find serological markers that can accurately reflect the level and activity of cccDNA in the liver to indirectly reflect the progression of liver fibrosis.
Wang class [3] Studies have also shown that serum HBV RNA is virus-like particles formed by untranscribed or partially transcribed pgRNA coated with HBsAg. Further studies found that the No [3] Under the dual verification of cell experiments and animal experiments, the level of pgRNA increased after blocking the reverse transcriactivity of HBV DNA polymerase, which indicates that NAs, only blocking rcDNA generation but not affecting pgRNA synthesis, means that this part of pgRNA level is not affected by NAs and can be used for clinical detection. GIERSCH [2] Studies have found that serum HBV RNA in untreated HBeAg-positive HBV-infected mice was associated with intrahepatic cccDNA levels (r =0.89, P <0.001). Professor Chen's team showed that the serum HBV RNA level was linearly correlated with the degree of significant liver fibrosis in both HBeAg positive and negative patients, and it was able to predict significant liver fibrosis progression more accurately than the two prediction formulas including APRI and FIB-4 [4].
Hepatitis B virus core-associated antigen (hepatitis B core related antigen, HBcrAg) is a composite marker containing HBcAg, HBeAg, and p22 proteins [5], Related to the cccDNA transcriptional activity in hepatocytes, and it is valuable in distinguishing the disease stage, predicting the reversal of liver fibrosis, and predicting the risk of HCC [6]. Sun Chao et al [7] The CHB patients were collectedLiver biopsy tissue and serum samples, measuring histopathology and HBcrAg levels, indicated a correlation between serum HBcrAg level and liver fibrosis grade and inflammation stage in CHB patients. And Junko Tanaka et al [8] Among the 529 e-negative patients with FIB-43.6, hepatitis B surface antigen (HBsAg), HBV DNA, hepatitis B core antigen associated with (HBcrAg), but genotype was not associated with previous status, and HBsAg≥3.0log IU / mL and HBcrAg≥3.7log IU / mL were independently associated with progression of cirrhosis. Liu Ruyu et al [9] A total of 246 patients with untreated chronic hepatitis B infection, all undergoing liver biopsy at baseline, showed serum HBcrAg to correctly identify patients with significant fibrosis with an area under the subject operating characteristic curve of 0.81 (95% CI,0.75-0.88). The APRI, FIB-4 index, and ALBI score identified significant liver fibrosis, with the area under the ROC curve being 0.74 (95% CI,0.66-0.81), 0.73 (95% CI,0.65-0.80), and 0.63 (95% CI,0.55-0.72), respectively. Compared with these three indicators, the accuracy of obvious fibrosis based on HBcrAg was higher than the FIB-4 index (p = 0.0479) and ALBI score (p = 0.0030). Zhang Xiujuan et al [10]. A prospective multicenter study of 403 CHB patients with variables related to Ishak fibrosis score and fibrosis regression regression, showed that 88.37% of patients receiving entecavir at week 72 had undetectable HBV DNA, but their serum HBcrAg was still detectable, and a greater reduction in HBcrAg concentration after treatment was associated with regression and histological improvement of liver fibrosis.
The objective of this study was to determine the clinical value of serum HBV RNA combined with HBcrAg in evaluating the degree of HBV DNA-negative hepatitis B liver fibrosis. Determine the efficacy of serum HBV RNA combined with HBcrAg to test the effect of double antiantibody treatment.
Materials and Methods
Study Subjects and Group Plan
According to the inclusion and exclusion criteria of this study, 284 patients with hepatitis B and liver fibrosis were selected in our department from December 2022 to May 2023. In the laboratory, the remaining blood samples after admission or outpatient blood examination were collected in the EDTA anticoagulant tube (purple tube), and the serum was collected in the -80℃ refrigerator. This study was reviewed by the hospital ethics committee and approved for the clinical study. All patients volunteered to participate in the study and signed informed consent before enrollment. According to the non-invasive liver fibrosis classification standard, each group was divided into three groups: mild, severe and severe liver fibrosis group, and according to the treatment plan, it was divided into two subgroups: mAb group and double mab group. Both the 2019 and 2022 editions of the guidelines for the prevention and treatment of chronic hepatitis B state that for patients using NAs drugs, their blood routine, liver biochemical indicators, HBV DNA quantification, HBV serological markers, and liver stiffness values should be tested once every 3 to 6 months. Therefore, 12 weeks and 24 weeks were selected as the basis for evaluating the endpoint of anti-fibrotic effect.
Diagnostic Criteria and Classification Criteria
The non-invasive diagnostic criteria for chronic hepatitis B liver fibrosis proposed in the 2019 guidelines for the prevention and treatment of chronic hepatitis B shall prevail, as follows: FIB-43.25 diagnosed liver fibrosis and liver inflammation grade Metavir score F3, and FIB-4 <1.45 excluded Metavir score F3[11]. The calculation formula of FIB-4 is: age (year) AST (IU / L) / [platelet count (109/L) ×√ALT (IU/L). According to the above principles, the classification criteria of hepatitis B liver fibrosis in this study: according to the LSM value classification: <9.85 kPa, mild liver fibrosis; 9.85-15.85kPa, moderate liver fibrosis; 15.85-17.4kPa, severe liver fibrosis [12]. When measuring the LSM of a patient's liver, we will comprehensively assess the accuracy of LSM based on the results of liver color Doppler ultrasound (excluding fatty liver) and liver function results, minimizing errors as much as possible. For specific reference, please refer to the expert consensus on the diagnosis of liver fibrosis by transient elastography in 2018.
Inclusion Criteria and Exclusion Criteria
Inclusion Criteria for Hepatitis B and Liver Fibrosis
Diagnosis of patients with chronic hepatitis B liver fibrosis who met the above criteria; Antiviral treatment has been performed and serum HBV DNA <10 IU / mL;Sign the informed consent for this study and follow follow-up for 24 weeks.
Exclusion Criteria for Hepatitis B and Liver Fibrosis
Serious primary diseases of the heart, brain, kidney and other organs;Infected with HCV, HIV and HDV virus;Patients with chronic hepatitis B being treated with interferon;Patients with severe systemic diseases and mental disorders;Female patients during lactation and pregnancy;Patients with neoplastic diseases and other hepatitis causes, such as drug-induced liver injury, immune hepatitis, fatty liver, etc.
Study Methods
Main reagents, Consumables and Instruments
The HBV RNA was extracted from the serum using the magnetic bead method according to the manufacturer's instructions (Beijing Rejing Bio) and followed the operating instructions in the kit. Other test reagents and main instruments: isopropyl alcohol, absolute ethanol, 1.5-mL RNase-Free centrifuge tube, PCR reaction tube, pipette gun head (200µL), Shake mixer, magnetic bead separator, pipete of various specifications, fluorescence quantitative PCR instrument (bio rad cfx96), automatic nucleic acid extraction instrument (Magmix 48). Serum HBcrAg was detected by double-antibody enzyme-linked immunosorbent assay according to the manufacturer's instructions. Main instruments and software: microplate reader (Thermo Scientific Multiskan GO), ELISA Calc software.
Statistical Methods
Group analysis of measurement data was performed using SPSS25.0 software, Comparison between the two different groups, Compliance with a normal distribution and homogeneity of variance using a two-independent samples t-test, Non-normal distribution, or uneven variance using the Mann-Whitney U test; Multiple-group comparison of the data, In line with normal distribution and homogeneity of variance, Non-normal distribution, or uneven variance using the Kruskal-Wallis test; Using the Kolmogorov-Smirnov test or the Shapiro Wilk test for the normality of the data, Non-normal distributed data were transformed by the natural log method; Pearson (Person) correlation analysis, Spearman correlation analysis was used to determine the relationship between indicators; Comparison of count data between groups using χ2U-test was used to compare grade data; multiple linear regression was used to analyze serum HBV RNA and serum HBcrAg influencing factors and receiver operating characteristic curve (ROC curve) to evaluate the correlation value of serum HBV RNA and HBcrAg and hepatitis B fibrosis; the final presentation of data was expressed by mean ± standard deviation (x ± s) or median (upper and lower quartile).
Results
Statistics of the Clinical Data
A total of 372 cases meeting the enrollment criteria were included, including 292 mild, 56 moderate and 24 severe liver fibrosis, and 284 patients participated in the study. During the subsequent follow-up, 73 patients participated in the follow-up and 131 patients participated in the follow-up of 24 weeks of treatment. The general clinical data at baseline were included. Table 1 showed no significant statistical differences (P> 0.05) in age, sex group (ALT), aspartate amino transferase (AST), γ -glutamyltransferase (GGT), total bilirubin (TBIL) and direct bilirubin (DBIL) (P <0.05), consistent with the condition.
Correlation Analysis Between Two Indexes and Liver Fibrosis Under Different E-Antigen States
During the course of the study, we found significant differences in HBV RNA and e-antigen negative and e-antigen positive (P <0.05), and no significant statistical differences in HBcrAg and e-antigen negative (P> 0.05). So, we divided the data into e antigen negative and e antigen negative two groups, respectively in the e antigen negative and e antigen negative correlation with liver fibrosis, through the liver hardness value (LSM value) reaction liver fibrosis severity, detailed in Table 2.
From the above table, person Correlation analysis showed that, In the case of a positive e-antigen profile, HBcrAg Is a positive correlation with LSM values (r=0.289, p =0.087<0.1), Spearman Correlation analysis showed that, In the e-antigen-negative case, HBcrAg No correlation with the LSM value (r=-0.002, p=0.984>0.1), In the case of a positive e-antigen profile, HBV RNA Is a positive correlation with LSM values (r=0.388, p =0.028<0.1), In the e-antigen-negative case, HBV RNA Is a positive correlation with LSM values (r=0.228, p=0.042<0.1), In conclusion, Whether the e-antigen is negative or positive, HBV RNA Are both associated with liver fibrosis, And showed a positive correlation, This is basically consistent with the research conclusions of Professor Chen Liang's team; Only in the e-antigen-positive cases was HBcrAg positively associated with liver fibrosis, Whereas in the e-negative case, HBcrAg Has no correlation with liver fibrosis.
Correlation Analysis Between Serum Hbv Rna and Serum Hbcrag and Other Factors
It has been shown that serum HBV RNA is affected by multiple factors, including the periods of chronic HBV infection [13], HBeAg status, glutamotransferase (ALT) level, HBV genotype [14]. In order to further clarify the correlation between other factors and the two indicators, multiple linear regression was used to analyze the factors affecting serum HBV RNA and serum HBcrAg, as shown in Figure 1 and 2. Where the independent variable Y indicates serum HBV RNA or serum HBcrAg, and the dependent variable X, in turn, indicates age, ALT, AST, GGT, TBIL, DBIL, and HBsAg factors.
As can be seen from Figure 1, independent variables X1, X2, X3, X4, X5, X6 and X7 do not have statistical significance at the test level of α=0.05. As can be seen from Figure 2, independent variables X1, X2, X3, X4, X5, X6 were not significant at α=0.05 test level, while independent variable X7, that is, Hepatitis B surface antigen (HBsAg), was statistically significant at α=0.05 test level, indicating that HBsAg may be a related factor affecting serum HBsAg. Meanwhile, combined with Table 3.2, it is shown that HBeAg status is an influential factor for serum HBV RNA.
The Predictive Value of Serum HBV RNA and Hbcrag For Dynamic Prediction of Liver Fibrosis
To further discuss the predictive value of serum HBV RNA and serum HBcrAg to predict liver fibrosis and combine the difference between the two indexes and HBeAg status, the ROC curve was used to classify e antigen status, as shown in Figure 3-5.
Under the ROC curve of the mild, moderate and severe liver fibrosis was 0.500,0.500, and 0.675, respectively, and the ROC curve of the mild, moderate and severe liver fibrosis was 0.587,0.500, and 0.869, respectively. Among them, the average area under the curve of mild and moderate liver fibrosis under e-antigen negative was around 0.5, Represents meaningless; The average area under the curve of mild liver fibrosis and moderate liver fibrosis under e antigen was around 0.5, It means meaningless, In which, the area under the curve of severe liver fibrosis was 0.869, Serum HBV RNA alone predicted the area under the ROC curve of 0.857, The combined prediction of both patients can improve the diagnostic efficiency; Further analysis of the optimal cut-off value, To ved that when the HBV RNA critical value is greater than 5011.73, It has a sensitivity of 1, The specificity was 0.75, When the HBcrAg critical value is greater than 0.5664, With a sensitivity of 0.333, The specificity is 1.
Difference Between the Two Indexes of The Double Antibody Group and Mab Group Under the Same Liver Fibrosis Grade
In order to further evaluate the treatment effect of dual-antibody group and mAb group, we evaluated the difference of HBV RNA and HBcrAg under the same liver fibrosis grade at different periods, so that the treatment effect of indirect response was at different periods.
The results showed that there was no significant difference in baseline serum HBV RNA and serum HBcrAg between the "monoclonal antibody group" and the "double-clonal antibody group" in the same hepatic fibrosis condition (P > 0.05). During subsequent follow-up of 12 and 24 weeks, serum HBV RNA and serum HBcrAg showed no significant difference between the "monoclonal antibody group" and the "double-clonal antibody group" (P > 0.05), preliminarily indicating that there was no significant change in liver fiber degree between the two groups after the application of anti-fibrotic drug intervention. In order to further verify the possibility of conclusion, we conducted the following analysis.
Analysis of Serum HBV RNA and Serum HBcrAg Levels
At weeks 12 and 24, we compared the changes of serum HBV RNA and serum HBcrAg dynamics, and conducted pairwise analysis between groups using Kruskal-Wallis test and Mann-WhitneyU test. In order to further test the dynamic level changes of the two indexes, the dynamic level changes of liver hardness value (LSM value) were compared horizontally. Kruskal-Wallis test and Mann-WhitneyU test were used to analyze the difference between groups.detailed in Table 3.
From the above results, there was no significant difference in serum HBV RNA and serum HBcrAg (P> 0.05) (P> 0.05), indicating that there was no significant difference in alleviating liver fibrosis in the "double antibody group" and the "single antibody group" at 24 weeks of follow-up treatment.
Discussion
Correlation Between Chronic Hepatitis B HBV-DNA and Liver Function Index and Liver Fibrosis
This study used the combination of LSM and FIB-4 to diagnose and grade liver fibrosis, with FibroTouch used to measure liver stiffness (LSM value). In this study, the majority of the HBeAg-negative chronic hepatitis B patients had liver fibrosis, while the HBeAg-positive patients were a minority, which is consistent with the actual clinical situation. Studies have shown that the diagnostic efficacy of using FibroTouch alone was 0.844[15]. A multicenter prospective study also showed that the accuracy of LSM in detecting significant liver fibrosis and cirrhosis in chronic hepatitis B patients is reliable [16]. In this study, other possible factors affecting the LSM value such as viral hepatitis and fatty liver were excluded. In summary, it is feasible to evaluate the stage of hepatitis B fibrosis by using FibroTouch only to measure liver hardness.
This study observed that the liver biochemical indicators were different at different levels of liver fibrosis. The enrolled patients in this study were all HBV DNA-negative chronic hepatitis B patients, so the relationship between HBV DNA load and liver fibrosis is also worth analyzing and discussing. Zhang Yan et al. [17] showed that serum HBV DNA load is strongly correlated with laminin (LN), and weakly correlated with hyaluronic acid (HA), type III procollagen (PCIII), and type IV collagen IV-C (IV-C), but the conclusions of the above studies are controversial. However, the results of the next study showed that the biochemical indexes of liver fibers were negatively correlated with albumin and platelets, and positively correlated with ALT, AST, TBIL and TBA [17], Previous studies also conducted liver pathology analysis in patients with chronic hepatitis B and found that serum type IV collagen, type III procollagen, hyaluronidase had a good correlation with liver type IV collagen, suggesting that serum liver fibrosis indexes are good indicators for the diagnosis of liver fibrosis and the degree of liver fibrosis [18] .which is consistent with the results observed in this experiment, that the degree of liver fibrosis is positively correlated with the patient's liver function indicators.
Factors Affecting Serum HBV RNA and Hbcrag
In clinical work, we found that although the antiviral efficacy of nucleoside (acid) (NA) drugs is significant, and the serum HBV DNA of CHB patients remains negative after treatment, some patients still have persistent liver inflammation and progress in liver fibrosis. The majority of chronic hepatitis B patients are HBV DNA-negative after treatment, so to exclude the influence of HBV DNA load on serum HBV RNA and serum HBcrAg, all enrolled patients were HBV DNA-negative (with a quantitative detection result of <10 IU/mL).
Peng Ymeng et al. [19] showed that HBeAg was an influential factor in the serum HBV RNA level of patients with chronic hepatitis B, and qHBsAg and HBeAg were influential factors in the lower detection limit of serum HBV RNA in patients with chronic hepatitis B. However, the experiment had problems such as small sample size and low viral load, so the experimental conclusions need to be verified.Another study [20] found that HBsAg and ALT were independent factors affecting the detection rate of HBV RNA, and HBsAg was significantly positively correlated with HBV RNA. Overall, serum HBV RNA was strongly correlated with HBcrAg (r=0.760, p < 0.001), while it was moderately correlated with HBV DNA and HBsAg, with correlation coefficients of 0.663 and 0.670, respectively. However, in chronic hepatitis B patients, HBV RNA was significantly correlated with HBCRAG. Only serum HBcrAg has a stable correlation with serum HBV RNA formation [21]. Another study showed that HBV DNA and HBeAg were independent risk factors for pg RNA positivity [22].
In summary, serum HBV RNA is related to HBeAg status, partially related to HBV DNA, HBsAg, and ALT levels, and the correlation is not strong, which may be related to disease stage and antiviral regimen. In this experiment, all enrolled patients were HBV DNA-negative (quantitative detection result <10 IU/mL), and ultimately 47.33% (231/488) were not detected, at the lower limit of the experiment (300 copies/mL). Due to the lack of some clinical data in this experiment, the effects of disease stage and antiviral regimen on serum HBV RNA could not be discussed. The final analysis showed that HBeAg status was a factor affecting serum HBV RNA, and there was no significant correlation with HBsAg and ALT (p> 0.05), which was basically consistent with the above research conclusions. We also explored the influencing factors of serum HBcrAg.
The results of Barbara Testo et al. [23] showed that serum HBcrAg was significantly higher in e antigen-positive patients than in e antigen-negative patients, and serum HBcrAg was correlated with serum HBV-DNA, liver tHBV-DNA, pgRNA and cccDNA levels in e antigen-positive patients.According to the conclusion of previous studies on the effect of cccDNA activity on liver fibrosis [2], combined with the findings in this study that serum HBcrAg was positively correlated with liver fibrosis indicators in patients with positive e antigen, but no correlation was found between serum HBcrAg and liver fibrosis indicators in patients with negative e antigen, which may be related to differences in test methods. Therefore, there was no significant difference in serum HBcrAg between the e antigen-positive group and the e antigen-negative group in general (p > 0.05). Therefore, this experiment could not conclude that the e antigen status was also an influencing factor of serum HBcrAg based on the existing results.
To further determine the correlation between serum HBcrAg and other factors, this experiment performed multiple linear regression analysis and found that overall, serum HBcrAg had a moderate correlation with HBsAg, and no correlation with ALT, AST, GGT, TBIL, and DBIL, suggesting that HBsAg is a factor affecting serum HBcrAg. Barbara Testo et al. further analyzed the correlation between serum HBcrAg and intrahepatic viral markers, and found that in HBeAg-positive patients, serum HBcrAg was correlated with HBsAg, but in HBeAg-negative chronic hepatitis B patients, serum HBcrAg was not related to HBsAg. Previous literature [24-29] also explained this point. This also explains why in this experiment, serum HBcrAg had a moderate correlation with HBsAg overall.
Double-Antibody Efficacy Analysis
As the clinical research on the prevention and treatment of chronic hepatitis B-related liver fibrosis with traditional Chinese medicine deepens, many Chinese patent medicines such as Anluohua Xin'an, Fuyang Huayin Tablets, and Fuzheng Huayu Capsules have been included in the 2019 Guidelines for the Integrated Diagnosis and Treatment of Liver Fibrosis [30], which proves the definite efficacy of traditional Chinese medicine in anti-hepatitis B liver fibrosis.
Liu Yiqi et al. [31] enrolled 780 chronic hepatitis B patients and found that after 78 weeks of treatment, in patients with baseline F≥3, the fibrosis regression rate in the ETV+ALHX (Anluohua Xin'an) group was significantly higher than in the ETV group: 124/211 (58.8%) vs. 45/98 (45.9%), p=0.035. The proportion of patients with a decrease in liver stiffness measurement (LSM) was higher in the ETV+ALHX group: 156/211 (73.9%) vs. 62/98 (63%), p=0.056. Logistic regression analysis showed that ETV combined with Anluohua Xin'an was related to fibrosis regression. Another study also had similar conclusions [32], indicating that after 72 weeks of treatment, the fibrosis reversal rate in the Fuyang Huayin Tablets combined with entecavir group was significantly higher than that in the entecavir group alone. Therefore, if the follow-up time of this experiment can be extended, dynamic changes in serum HBV RNA and serum HBcrAg may occur, and the predictive value for the disease will also be reflected accordingly.There are also studies that have separately researched the efficacy of anti-fibrotic Chinese patent medicines[33], finding that after 48 weeks of treatment, the pathological reversal rate in the Anluohua Xin'an or Fuyang Huayin Tablets treatment group was higher than that in the placebo group. Lou Yan et al. [34] used network meta-analysis to suggest that the effect of the combined use of 5 Chinese patent medicines (Dahuang Ganjinwang, Fuyang Huayin Tablets, Ganjie Wan, Fuzheng Huayu Capsules, Anluohua Xin'an) with entecavir was better than the use of entecavir alone in terms of liver stiffness measurement (LSM).
From the above research conclusions, it can be seen that after a period of treatment, anti-liver fibrosis traditional Chinese medicine can effectively improve liver fibrosis. However, the 2019 Guidelines for the Integrated Diagnosis and Treatment of Liver Fibrosis do not specify the treatment cycle in detail, only mentioning it in Opinion 13: [35] liver fibrosis requires long-term treatment, and then only gives the clinical criteria for stopping the use of anti-fibrotic drugs. The guidelines also suggest that the course of treatment can be individualized according to the treatment goal and the patient's specific condition. Xue Jianhua et al. [36] found that after 24 weeks of treatment, the CAP value in the treatment group was better than the control group, with a statistically significant difference (p <0.05), but the enrolled patients were all untreated, virus-replicating chronic hepatitis B patients, also reflecting the individual differences in anti-liver fibrosis.
The results of this experiment showed that after 24-week follow-up, there was no significant difference in liver stiffness value (LSM value) (p>0.05) and liver fibrosis indicators (serum HBcrAg and HBcrAg) (p>0.05) between the groups. However, at baseline, the correlation between the serum fibrosis parameters and liver stiffness value (LSM value) was relatively good. In summary, the failure of the double antiviral treatment in this experiment may be related to the short follow-up time.
The Combined Predictive Value of Serum HBV RNA And Hbcrag for Liver Fibrosis
There have been many reports on the predictive value of serum HBV RNA and serum HBcrAg for liver fibrosis. Huang, CL et al. [4] found that HBV RNA had better diagnostic efficacy in diagnosing significant liver fibrosis than APRI and FIB-4. In HBeAg-negative patients, the diagnostic efficacy of HBV RNA was also better than APRI and FIB-4. Further analysis found that both HBeAg-negative and positive were linearly correlated with liver fibrosis. Bian Dandan et al. [37] confirmed through liver biopsy that a decrease of serum HBV RNA greater than 0.63 log10 copies /ml at the 6th month could predict fibrosis regression at the 60th month. Therefore, it is concluded that HBV RNA measurement is a useful indicator for monitoring the changes of liver fibrosis in HBeAg-positive patients with chronic hepatitis B, but the above experiment only discussed the predictive efficacy of serum HBV RNA in the case of e antigen positive for significant liver fibrosis. Another study [38] showed that serum HBV RNA had predictive value in e antigen-negative patients, but the experiment did not compare the predictive efficiency of liver fibrosis at all levels one by one, and only summarized the whole, and did not further analyze the influence of DNA load and other factors on serum HBV RNA, so the conclusion needs to be further verified. This study confirmed good diagnostic efficacy of serum HBV RNA in patients with significant hepatitis B fibrosis (LSM > 15.85Kpa), and better in patients with e antig-positive chronic hepatitis B (area under ROC curve 0.857, sensitivity 1, specificity 0.75), while poor diagnostic efficacy in patients with non-significant hepatitis B fibrosis.
The predictive value of serum HBcrAg for liver fibrosis has also been reported. Zhang Xiujuan et al. [10] found that in HBeAg-positive chronic hepatitis B patients, the serum HBcrAg level was negatively correlated with the stage of liver fibrosis, while in HBeAg-negative chronic hepatitis B patients, it was positively correlated with the stage of liver fibrosis. Zhang Zhanqing et al found that [39] HBcrAg had a good performance in predicting the level of liver fibrosis in HBeAg negative patients.
Fan Weiguang et al. [40] also proved that the AUC of serum HBcrAg for predicting S3 patients was 0.647, but did not discuss the HBeAg status. However, this experiment found that in HBeAg-positive patients, serum HBcrAg was positively correlated with liver fibrosis indicators, but in HBeAg-negative patients, serum HBcrAg was not correlated with liver fibrosis indicators, which is inconsistent with the research conclusions of Zhang Xiujuan et al. But the above studies were established in untreated chronic hepatitis B patients. According to Barbara Testo's research conclusion [23], in HBeAg-negative chronic hepatitis B patients, higher serum HBcrAg would lead to higher fibrosis and inflammatory activity, so the correlation between serum HBcrAg and liver fibrosis stage in HBeAg-negative patients’ needs to be compared after keeping the serum HBV-DNA, intrahepatic tHBV-DNA, and inflammatory scores consistent. The study also found that the predictive efficacy of serum HBcrAg for severe liver fibrosis in HBeAg-positive patients was lower than that for moderate liver fibrosis, but the overall predictive efficacy was stronger than that in HBeAg-negative patients, which may be related to the smaller number of HBeAg-positive chronic hepatitis B patients enrolled.
Summary and Outlook
In summary, this study confirmed that for patients with severe liver fibrosis, the diagnostic efficacy is better, and the combination of serum HBV RNA and serum HBcrAg for predicting HBeAg-positive has an AUROC of 0.869, which is better than the predictive value of a single indicator.
This study has some limitations. The observation that the predictive efficacy of serum HBcrAg for severe liver fibrosis in HBeAg-positive patients was lower than that for moderate liver fibrosis, while previous studies have shown that the predictive efficacy for significant liver fibrosis was better, may be related to the smaller number of HBeAg-positive chronic hepatitis B patients enrolled. In addition, the difference in the correlation between serum HBcrAg and liver fibrosis compared with previous studies may be related to the inconsistent inclusion criteria of patients, but may also be related to the difference in detection methods. A study conducted by Japanese scholars showed [41] that iTACT HBcrAg was more convenient than traditional HBcrAg detection method, with shorter sample pretreatment time and higher sensitivity. In combination with this study, all the enrolled patients were HBV DNA negative chronic hepatitis B patients, and the experimental results showed that serum HBcrAg was at a low concentration. Using this method may reduce the experimental error and improve the accuracy.
This experiment also found that 47.33% (231/488) of serum HBV RNA was not detected, which may be related to the enrolled patients, but cannot rule out the relationship with the experimental method. Professor Zhang Wenhong's research team pointed out [42] that in HBV DNA low-concentration samples (HBV DNA <100 IU/mL), the SAT (Simultaneous Amplification and Testing) detection rate was 77.27%, and the reverse transcription PCR detection rate was 59.09%, suggesting that SAT has higher sensitivity than conventional reverse transcription PCR in HBV DNA low-concentration samples. Using the above detection methods may improve the detection rate and further analyze the correlation between undetected patients' serum HBV RNA and other factors.
Due to the small number of HBeAg-positive chronic hepatitis B patients in this experiment and the lack of some clinical data during continuous follow-up, more patients meeting the inclusion criteria need to be enrolled in the future to further verify the experimental conclusions. Since this experiment did not observe dynamic changes in liver fibrosis after treatment, the follow-up time needs to be further extended to clarify the optimal cutoff values of the two serum indicators after liver fibrosis is improved, in order to provide help for clinical diagnosis and prevention.
References
- Liu J, Liang W, Jing W, et al. (2019) Countdown to 2030: eliminating hepatitis B disease, China[J]. Bull World Health Organ. 97: 230-8.
- Giersch K, Allweiss L, Volz T, et al. (2017) Serum HBV pgRNA as a clinical marker for cccDNA activity[J]. J Hepatol. 66: 460-2.
- Wang J, Shen T, Huang X, et al. (2016) Serum hepatitis B virus RNA is encapsidated pregenome RNA that may be associated with persistence of viral infection and rebound[J]. J Hepatol. 65: 700-10.
- Huang C, Li Q, Xu W, et al. (2020) Serum HBV RNA levels predict significant liver fibrosis in patients with chronic HBV infection[J].Discov Med. 29: 119-28.
- Mak L Y, Wong D K, Cheung K S, et al. (2018) Review article: hepatitis B core-related antigen (HBcrAg): an emerging marker for chronic hepatitis B virus infection[J]. Aliment Pharmacol Ther. 47: 43-54.
- Chuaypen N, Posuwan N, Payungporn S, et al. (2016) Serum hepatitis B core-related antigen as a treatment predictor of pegylated interferon in patients with HBeAg-positive chronic hepatitis B[J]. Liver Int. 36: 827-36.
- Fan R, Peng J, Xie Q, et al. (2020) Combining Hepatitis B Virus RNA and Hepatitis B Core-Related Antigen: Guidance for Safely Stopping Nucleos(t)ide Analogues in Hepatitis B e Antigen-Positive Patients with Chronic Hepatitis B[J]. J Infect Dis. 222: 611-8.
- Tada T, Kumada T, Toyoda H, et al. (2018) Hepatitis B virus core-related antigen levels predict progression to liver cirrhosis in hepatitis B carriers[J]. J Gastroenterol Hepatol. 33: 918-25.
- Liu R, Li M, Lu Y, et al. (2022) Hepatitis B core-related antigen serum levels are associated with significant liver fibrosis in treatment-naive chronic HBV infection patients[J]. J Viral Hepat. 29: 438-46.
- Chang X J, Sun C, Chen Y, et al. (2019) On-treatment monitoring of liver fibrosis with serum hepatitis B core-related antigen in chronic hepatitis B[J]. World J Gastroenterol. 25: 4764-78.
- Jia Jidong, Hou Jinlin, Wei Lai, et al. (2020) New highlights of the Guidelines for prevention and Treatment of Chronic Hepatitis B (2019 edition) [J]. Chinese Journal of Liver Diseases. 28: 3.
- Chen Gaofeng, Pingjian, Gu Hongtu, etc. (2017) Correlation analysis of liver stiffness measured by FibroTouch and FibroScan and liver histological Ishak fibrosis score in patients with chronic hepatitis B [J]. Chinese Journal of Liver Diseases. 25: 145-50.
- Luo H, Zhang X X, Cao L H, et al. (2019) Serum hepatitis B virus RNA is a predictor of HBeAg seroconversion and virological response with entecavir treatment in chronic hepatitis B patients[J]. World J Gastroenterol. 25: 719-28.
- Sun Chao, Chang Xiujuan, Li Xiaodong, et al. (2019) HBcrAg Application value in the natural course of chronic hepatitis B and in predicting the reversal of liver fibrosis [J]. Journal of Clinical Hepatobiliary Diseases. 35: 328-33.
- Shen Xiaofei. FibroTouch (2021) Clinical study of advanced liver fibrosis combined with liver serum biochemical index [master's thesis]. Dalian Medical University.
- Marcellin P, Ziol M, Bedossa P, et al. (2009) Non-invasive assessment of liver fibrosis by stiffness measurement in patients with chronic hepatitis B[J]. Liver Int. 29: 242-7.
- Zhang Yan, Xiao Xiang, Han Changquan, et al. (2021) The relationship between HBV-DNA, and liver function index and liver fibrosis in patients with chronic hepatitis B [J]. Journal of Clinical Digestive Diseases. 33: 36-40.
- Xiao Hejian Jie, Li Congrong, Li Ping, et al. (2008) Study on the liver histopathology and serum liver fibrosis index for the diagnosis of liver fibrosis [J]. Journal of Tropical Medicine. 8: 561-3.
- Peng Yameng, Yuan Hao, Zhou Yifeng, et al. (2019) Serum levels of hepatitis B virus RNA and its influencing factors in patients with chronic hepatitis B virus with low levels of hepatitis B virus DNA [J]. General Practice in China. 22: 2217-22.
- Shen Yujuan, Chen Haiyan, Tong Luyuan, et al. (2023) Serum HBV RNA levels and their influencing factors in CHB patients treated with NAs [J]. Journal of Huzhou Normal University. 45: 69-74.
- Wang M L, Liao J, Ye F, et al. (2021) Distribution and factors associated with serum HBV pregenomic RNA levels in Chinese chronic hepatitis B patients[J]. J Med Virol. 93: 3688-96.
- Yan H Z, Huang Z H, Guo X G, et al. (2022) A Study on Pregenomic RNA and Factors Related to Hepatitis B Virus Infection Based on Real World[J]. Front Public Health. 10: 856103.
- Testoni B, Lebossé F, Scholtes C, et al. (2019) Serum hepatitis B core-related antigen (HBcrAg) correlates with covalently closed circular DNA transcriptional activity in chronic hepatitis B patients[J]. J Hepatol. 70: 615-25.
- Nassal M.Hbv (2015) cccDNA: viral persistence reservoir and key obstacle for a cure of chronic hepatitis B[J].Gut. 64: 1972-84.
- Zhang X, Lu W, Zheng Y, et al. (2016) In situ analysis of intrahepatic virological events in chronic hepatitis B virus infection[J]. J Clin Invest. 126: 1079-92.
- Tu T, Budzinska M A, Shackel N A, et al. (2017) HBV DNA Integration: Molecular Mechanisms and Clinical Implications[J]. Viruses. 9: 75.
- Lebossé F, Testoni B, Fresquet J, et al. (2017) Intrahepatic innate immune response pathways are downregulated in untreated chronic hepatitis B[J]. J Hepatol. 66: 897-909.
- Volz T, Lutgehetmann M, Wachtler P, et al. (2007) Impaired intrahepatic hepatitis B virus productivity contributes to low viremia in most HBeAg-negative patients[J]. Gastroenterology. 133: 843-52.
- Wooddell C I, Yuen M F, Chan H L, et al. (2017) RNAi-based treatment of chronically infected patients and chimpanzees reveals that integrated hepatitis B virus DNA is a source of HBsAg[J]. Sci Transl Med. 9: eaan0241.
- Sister Shi Mei, Xiao Huanming, Xie Yubao, et al. (2023) Current status, challenges and thinking on the prevention and treatment of chronic hepatitis B liver fibrosis by traditional Chinese medicine [J]. Journal of Clinical Hepatobiliary Diseases. 39: 1280-6.
- Liu Y Q, Zhang C, Li J W, et al. (2023) An-Luo-Hua-Xian Pill Improves the Regression of Liver Fibrosis in Chronic Hepatitis B Patients Treated with Entecavir[J]. J Clin Transl Hepatol. 11: 304-13.
- Rong G, Chen Y, Yu Z, et al. (2022) Synergistic Effect of Biejia-Ruangan on Fibrosis Regression in Patients With Chronic Hepatitis B Treated With Entecavir: A Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial[J].J Infect Dis. 225: 1091-9.
- Xiao H M, Shi M J, Jiang J M, et al. (2022) Efficacy and safety of AnluoHuaxian pills on chronic hepatitis B with normal or minimally elevated alanine transaminase and early liver fibrosis: A randomized controlled trial[J]. J Ethnopharmacol. 293: 115210.
- Lou yan (2023) Reticular meta-analysis of five Chinese patents combined with entecavir for chronic hepatitis B liver fibrosis or cirrhosis [master's thesis]. Hubei University of Traditional Chinese Medicine.
- The Liver Disease Professional Committee of the Chinese Society of Integrated Traditional Chinese and Western Medicine (2019) Guidelines for the Diagnosis and Treatment of Integrated Traditional Chinese and Western Medicine in liver fibrosis (2019 edition) [J]. Chinese Journal of Liver Diseases. 27: 494-504.
- Xue Jianhua, Cheng Yang, Chen Jianjie, et al. (2019) Clinical observation of hepatitis B liver fibrosis with enacavir [J]. Traditional Chinese Medicine Information. 36: 57-60.
- Bian D, Zhao J, Liao H, et al. (2023) Serum HBV RNA is associated with liver fibrosis regression in HBeAg-positive chronic hepatitis B patients treated with nucleos(t)ide analogues[J]. J Viral Hepat. 30: 303-9.
- Yuan Yuhui (2021) Correlation analysis of serum HBV RNA level and hepatitis B-related liver fibrosis in HBeAg positive and negative patients [J]. Chinese Modern Doctor. 59: 1-5.
- Zhang Z Q, Shi B S, Lu W, et al. (2020) Quantitative HBcrAg and HBcAb versus HBsAg and HBV DNA in predicting liver fibrosis levels of chronic hepatitis B patients[J]. Gastroenterol Hepatol. 43: 526-36.
- Fan Weiguang, Chen Laiyin, An Weina, et al. (2022) HBcrAg, Predictive value of HBsAg on the degree of inflammation and fibrosis in liver tissue of CHB patients [J]. Marker immunoassay and clinical. 29: 101-6.
- Inoue T, Kusumoto S, Iio E, et al.Clinical efficacy of a novel, high-sensitivity HBcrAg assay in the management of chronic hepatitis B and HBV reactivation[J].J Hepatol. 75: 302-10.
- Wang Xuegang, Zhang Xinzhi, Yang Shu, et al. (2020) Correlation and consistency evaluation of the two HBV RNA methods in nucleoside (acid) analogues treated and treated chronic hepatitis B patients [J]. Liver. 25: 736-42.
Article Information
Research
Received Date: August 05, 2025
Accepted Date: August 24, 2025
Published Date: August 31, 2025
Clinical Study of the Predictive Value of Serum HBV RNA Plus Hbcrag for the Progression of Liver Fibrosis in Patients with HBV DNA-Negative Chronic Hepatitis B
Volume 1 | Issue 2
Citation
Chao Duan, Liming Liu, Jing Chen, Dai Dan, Hongmei Xia, et al. (2025) Clinical Study of the Predictive Value of Serum HBV RNA Plus Hbcrag for the Progression of Liver Fibrosis in Patients with HBV DNA-Negative Chronic Hepatitis B. Eur J Gastroenterol Digestive Dis 1: 201
Copyright
©2025 Liming Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jgdd.2025.1.201