

Review Article
Volume-1 Issue-1, 2025
Two Artery Embolizations for Severe Hematuria After Transrectal Ultrasonography Guided Prostate Biopsy: A Case Report
-
Received Date: March 03, 2025
-
Accepted Date: March 21, 2025
-
Published Date: March 28, 2025
Journal Information
Abstract
Bleeding complications after transrectal ultrasonography (TRUS)-guided prostate biopsy are common, but life- threatening severe hematuria is extremely rare. We present a case of severe hematuria after TRUS-guided prostatic biopsy. The patient had a TRUS-guided prostatic biopsy at another hospital. Severe gross hematuria occurred on the third day after biopsy and was transferred to our hospital for treatment. We performed interventional angiography on the patient after transfusion therapy failed. The first angiography showed extravasation of contrast media at bilateral bulbous urethral arteries, and the bleeding site was immediately embolized with gelatin sponge granules. On the 4th day after the embolization, the patient had a sudden hypovolemic shock. The patient was immediately treated with antishock therapy, and a second interventional angiography was performed with contrast extravasation in the bilateral prostatic arteries. We immediately used gelatin sponge granule to embolize bilateral prostatic artery and right inferior bladder artery. Hematuria completely disappeared after the second embolization. At 3 months of following-up, no bleeding related events occurred. We also describe the literature surrounding the complication and treatment measures. To our knowledge, this was the first report of prostatic arterial embolization in the treatment of life-threatening hematuria following TRUS-guided prostatic biopsy.
Key words
Prostate Biopsy; Hematuria; Interventional Embolization; Hemorrhagic Shock; Case Report
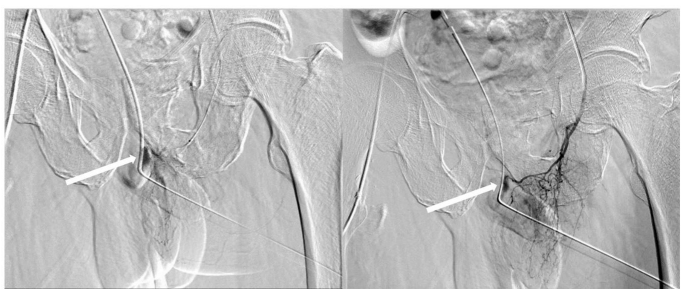 |
| Figure 1: Bilateral bulbar urethral arteries showed contrast extravasation |
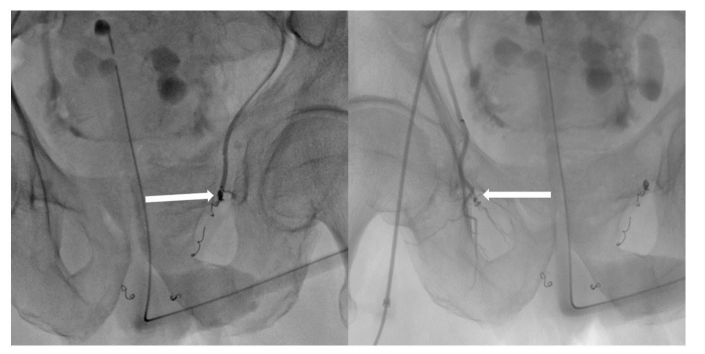 |
| Figure 2:Bilateral prostatic arterial contrast extravasation |
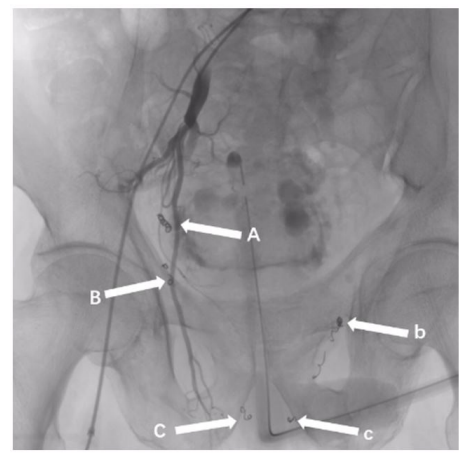 |
| Figure 3:A: Right inferior bladder artery embolism, B and b: Bilateral prostatic arterial embolism, C and c: Bilateral bulbar urethral artery embolism |
Introduction
TRUS-guided prostate biopsy is a common procedure in urology and is well tolerated by most patients [1]. However, its bleeding complications include hemospermia, hematuria, and rectal bleeding [2]. Most of the bleeding is mild and self-limited, and less than 1% of patients with severe hematuria requires hospitalization [3].
We reported a case of severe hematuria with hemorrhagic shock following TRUS-guided prostate biopsy.
Case report
A 72-year-old male, with dysuria for 2 months and excessive prostate-specific antigen (PSA:20 ng/ml), presented with massive gross hematuria on the third day after TRUS-guided prostate biopsy at another hospital. Physical examination at the time of transfer to our hospital: heart rate 78 bpm, blood pressure 105/70 mmHg, fully-filled bladder was palpable on the pubis, laboratory examination: normal blood coagulation function, hemoglobin (HGB): 70 g/L. An 18F three-chamber catheter was indwelling and the bladder was irrigated continuously. Dark red blood clots and bright red urine were observed. The bladder was compressed by the balloon to stop the bleeding and the blood transfusion was performed and reexamined HGB:67 g/L. Conventional hemostasis measures were ineffective, and angiography was performed under local anesthesia. During the operation, a large amount of contrast agent was found at bilateral bulbous urethral arteries. Gelatin sponge granules were used to embolize bilateral bulbous urethral arteries (Figure 1). After the operation, the gross hematuria of the patient was significantly reduced, and a small amount of reddish liquid was found to flow out after bladder irrigation and reexamined HGB:89 g/L. On the 4th day after the operation, the patient suddenly turned pale and sweaty at night, and a large number of gross hematuria occurred again. Examined urgently HGB: 60 g/L. Heart rate 135 bpm, blood pressure 74/45 mmHg. Interventional angiography was performed at the same time of antishock treatment, and severe contrast agent exudation was found in bilateral prostatic arteries. Considering the possibility of bleeding points, the patient was embolized with gelatin sponge granules for bilateral prostatic arteries (Figure 2) and right inferior bladder arteries (Figure 3). After surgery, the patient’s gross hematuria disappeared. Reexamined HGB:97 g/L. Heart rate 78 bpm, blood pressure 105/88 mmHg. One month after being safely discharged from hospital, prostate enucleation has been performed for the patient in our hospital. Postoperative pathological examination indicated benign prostatic hyperplasia. After 3 months of follow-up, no symptoms of hematuria or bleeding occurred and no dysuria was found.
Discussion
The occurrence of life-threatening hematuria after TRUS- guided prostate biopsy is rare, but if the puncture needle is not parallel to the urethra as much as possible during the puncture process, the urethra and the periurethral artery may still be damaged, thereby causing serious gross hematuria. Combined with the angiographic results of this patient, we inferred that bilateral bulbous urethral arteries and bilateral prostatic arteries may have been damaged during the puncture operation of this patient, resulting in severe hematuria. Treatments of hematuria after prostate puncture include [4], standardized use of hemostatic drugs, continuous bladder irrigation, three-chamber catheter compression, blood transfusion and endoscope-hemostasis. In this case, we did not choose endoscopic hemostasis after conventional treatment failed, because the diagnosis of prostate cancer was not completely excluded during the patient’s hospitalization. And studies have shown that endoscopic-hemostasis is not beneficial for long-term survival of prostate cancer patients [5]. At the same time, interventional embolization hemostasis was safe and fast for emergency bleeding than it, so we chose interventional embolization hemostasis.
During the first embolization process, active bleeding was found in bilateral bulbous urethral arteries, and gelatin sponge granules were used to embolize bilateral bulbous urethral arteries. Although the bleeding was temporarily stopped after surgery, severe hematuria occurred again 4 days later, possibly because the superior branch artery was not embolized. The bulbous urethral artery in adults mainly supplies the urethral cavernosum, which usually originates from the internal pudendal artery. For the first time, we embolized only bilateral bulbar urethral arteries and did not embolize the internal pudendal artery. Comparing to the second embolism, we embolized bilateral prostatic arteries and right inferior bladder arteries because the prostatic artery usually arose from the inferior bladder artery [6], and no events related bleeding occurred after surgery. At the same time, nocturnal penile erection might be the direct cause of secondary bleeding [7]. However, more studies are needed to confirm whether embolization of internal pudendal artery would cause erectile dysfunction or other complications, whether other patients can achieve better hemostatic effect after embolization of bilateral bulbous urethral artery, and whether drugs should be used to reduce penile erectile after embolization of penile supplying artery.
In conclusion, when conservative treatments for postoperative bleeding after TRUS-guided prostate biopsy are ineffective, embolization hemostasis is a feasible plan. We can try to embolize the upper branch vessels to achieve better hemostasis effect if we can make it safe.
Acknowledgements
This work was supported by our institution and team. We would like to thank all authors for their help in article content.
Funding
This work was supported by the Guizhou Science and Technology Agency Fund, under Grant: [2019]5405. The sponsor provided financial support for this research.
Availability of data and materials
The datasets used and/or analyzed during the present study are available from the corresponding author upon reasonable request.
Authors’ contributions
Jing-wen Ren analyzed the patient data and wrote the preliminary draft, Guang-heng Luo, Ye Tian , Tao Li provided expertise and edited the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors report no conflicts of interest.
References
- Haifeng Huang, Wei Wang, Tingsheng Lin (2016) Comparison of the complications of traditional 12 cores transrectal prostate biopsy with image fusion guided transperineal prostate biopsy[J]. BMC Urol 16: 1-6.
- Quinlan MR, Bolton D, Casey RG (2018) The management of rectal bleeding following transrectal prostate biopsy: A review of the current literature[J]. Can Urol Assoc J 12: E146-E153.
- Loeb S, Vellekoop A, Ahmed HU (2013) Systematic Review of Complications of Prostate Biopsy[J]. European Urology 64: 876-92
- Pinkhasov GI, Lin YK, Palmerola R (2012) Complications following prostate needle biopsy requiring hospital admission or emergency department visits - experience from 1000 consecutive cases[J]. BJU Int 110: 369-74.
- Choi SY, Ryu J, You D (2018) Oncological effect of palliative transurethral resection of the prostate in patients with advanced prostate cancer: a propensity score matching study[J]. J Cancer Res Clin Oncol 144: 751-8.
- Picel AC, Hsieh TC, Shapiro RM (2019) Prostatic Artery Embolization for Benign Prostatic Hyperplasia: Patient Evaluation, Anatomy, and Technique for Successful Treatment[J]. Radiographics 39: 1526-48.
- ZHONG Li-ming, WEI Xin, HU Hong, YOU Jian, ZHANG Zong- ping, et al. (2014) Clinical value of vascular embolization for genitourinary system hemorrhage. Med J of West China 26: 1480-2.
Artcle Information
Review Article
Received Date: March 03, 2025
Accepted Date: March 21, 2025
Published Date: March 28, 2025
Journal of Pediatric Care and Neonatology
Volume 1 | Issue 1
Citation
Jing-wen Ren (2025) Two Artery Embolizations for Severe Hematuria After Transrectal Ultrasonography Guided Prostate Biopsy: A Case Report. J Hepatol Nephrol Endocrinol Sci 1: 101
Copyright
©2025 Guang-heng Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jhne.2025.1.101