

Review Article
Volume-1 Issue-1, 2025
Knowledge, Attitude and Practices of Parents Regarding Home Management of Nephrotic Syndrome
-
Received Date: June 05, 2025
-
Accepted Date: June 23, 2025
-
Published Date: June 30, 2025
Journal Information
Abstract
Introduction: Nephrotic syndrome is a pathological entity characterized by massive proteinuria, hypoalbuminemia, hypercholesterolemia and generalized oedema. It is one of the common diseases in children. The epidemiology and incidence of NS vary, depending on the country and the ethnic origin of the children.
Materials and Methods: This aim of this cross sectional comparative study was to assess knowledge, attitude and practices of parents regarding home management of nephrotic syndrome and was carried out in the Department of Paediatric Nephrology, Cumilla Medical College Hospital, Cumilla conducted from April 2019 to October 2019. Study population were parents having children with nephrotic syndrome age ranging from 1-12 years. A total of 160 parent having children with nephrotic syndrome were included in this study. Knowledge, attitude and practices of parents regarding the home management in control (n=80) and case (n=80) were recorded.
Results: Mean age was almost similar in both groups (6.49 ± 2.67 years vs 6.43 ± 3.06 years). Male to female ratio were respectively 1.7:1 and 1.9:1 in both groups. Mean score of knowledge about signs and symptoms was 6.41 ± 1.68 in cases which was significantly (p< 0.001) higher than controls (2.88 ± 0.96). Mean score of practices of home management were 6.35 ± 2.20 in cases and 2.45 ± 1.09 in controls, there was significant difference between cases and controls (p< 0.001) Attitude regarding home management of nephrotic syndrome was found significantly (p< 0.001) higher in case than that of control (7.80 ± 1.10 vs 2.81 ± 0.85). There was significant positive correlation of knowledge of home management of nephrotic syndrome with practice (r=0.979 and p=< 0.001) of home management of nephrotic syndrome. The more the knowledge the more the home management practice.
Conclusion: Practices of home management of nephrotic syndrome are related to knowledge and attitude.
Key words
Knowledge; Attitude; Nephrotic Syndrome;
|
Case (n=80) |
Control (n=80) |
p-value |
Age (Years) |
|
|
|
≤5 |
36 (45.0) |
42 (52.5) |
0.524 |
6 - 10 |
35 (43.8) |
28 (35.0) |
|
>10 |
9 (11.3) |
10 (12.5) |
|
Mean±SD |
6.49 ± 2.67 |
6.43 ± 3.06 |
b0.892 |
Gender |
|
|
|
Male |
50 (62.5) |
53 (66.3) |
a0.620 |
Female |
30 (37.5) |
27 (33.8) |
|
Table 1:Baseline characteristics of the study subjects (n=160)
Table 1 shows demographic profile of the study subjects. Mean age was almost similar in both groups. Most of the patients were below or equal to 10 years in both groups. Male was predominant in both groups.
|
Case (n=80) |
Control (n=80) |
p-value |
Knowledge about signs and symptoms |
6.41 ± 1.68 |
2.88 ± 0.96 |
<0.001 |
Knowledge about diet |
7.69 ± 1.32 |
2.78 ± 1.16 |
<0.001 |
Knowledge about weight |
7.40 ± 1.09 |
2.45 ± 1.04 |
<0.001 |
Knowledge about urine examination |
7.49 ± 1.22 |
2.63 ± 1.32 |
<0.001 |
Knowledge about medication |
7.19 ± 1.24 |
2.58 ± 1.61 |
<0.001 |
Knowledge about infection and other complications |
6.73 ± 1.48 |
2.68 ± 1.05 |
<0.001 |
Knowledge about follow up |
7.15 ± 1.18 |
2.65 ± 1.30 |
<0.001 |
Table 2: Knowledge regarding the home management of nephrotic syndrome (n=160)
Table 2 Shows all parameters of knowledge regarding the home management of nephrotic syndrome were found significantly higher in cases (subsequent relapse) than that of control (initial episode).
Practice |
Case (n=80) |
Control (n=80) |
p-value |
Practices of home management |
6.35 ± 2.20 |
2.45 ± 1.09 |
<0.001 |
Practices of urine examination |
7.64 ± 1.29 |
2.55 ± 1.22 |
<0.001 |
Practices of dietary modification |
7.53 ± 1.51 |
2.76 ± 1.34 |
<0.001 |
Practices of skin care |
7.31 ± 1.50 |
2.64 ± 1.42 |
<0.001 |
Practices of prevention from infection and other complication |
7.20 ± 1.07 |
2.56 ± 1.38 |
<0.001 |
Practices of medication |
6.68 ± 1.37 |
2.49 ± 1.13 |
<0.001 |
Practice daily living activity |
6.95 ± 1.34 |
2.46 ± 1.29 |
<0.001 |
Practice emotional support |
6.41 ± 1.46 |
2.50 ± 1.06 |
<0.001 |
Practices follow up |
7.09 ± 1.14 |
2.66 ± 1.15 |
<0.001 |
Table 3: Practices regarding the home management of nephrotic syndrome (n=160)
Table 3 shows all parameters of practices regarding the home management of nephrotic syndrome were found significantly higher in cases than that of control
Attitude |
Case (n=80) |
Control (n=80) |
p-value |
It is a kidney disease |
6.63 ± 2.26 |
2.63 ± 0.99 |
<0.001 |
Needs home management |
6.58 ± 2.25 |
2.55 ± 1.03 |
<0.001 |
Home management can protect |
6.55 ± 2.24 |
2.54 ± 1.01 |
<0.001 |
Getting any home management yet |
6.51 ± 2.21 |
2.50 ± 1.03 |
<0.001 |
Table 4:Attitude regarding the home management of nephritic syndrome (n=160)
Table IV shows attitude regarding home management of nephrotic syndrome was found significantly higher in case than that of control
 |
|
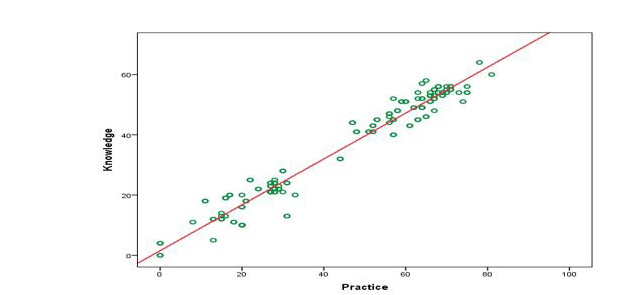
Pearson’s correlation test showed positive correlation. Here, r = 0.979 and p = < 0.001, that is the more the knowledge about home
management of nephrotic syndrome, the more is the home management practices Figure 1: Correlation between knowledge and practice |
 |
|
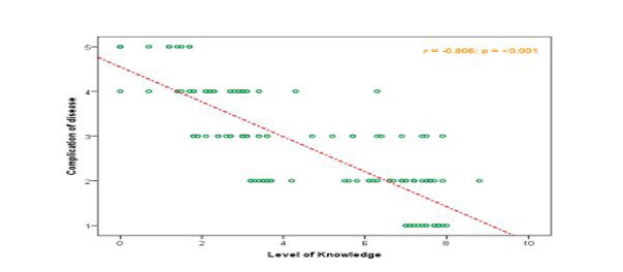
Pearson’s correlation test showed negative correlation. Here, r = -0.806 and p= < 0.001, that is more knowledge, attitude and practice
about the home management the less the complication of nephrotic syndrom Figure 2:Correlation of knowledge, attitude and practice with complication |
 |
|
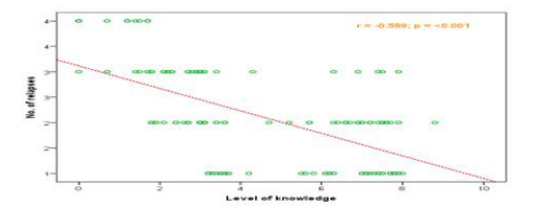
Pearson’s correlation test showed negative correlation. Here, r = -0.589 and p= < 0.001, that is more knowledge, attitude and
practice about the home management the less the number of relapse of nephrotic syndrome Figure 3:Correlation of knowledge, attitude and practice with number of relapse |
 |
|
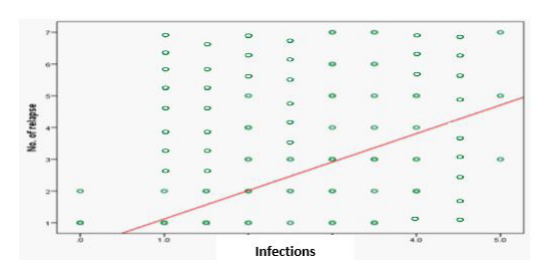
Pearson’s correlation test showed positive correlation. Here,r = 0.725 and p = < 0.001, that is the less the infections, less the
number of relapses Figure 4: Correlation between infections with number of relapses |
 |
|
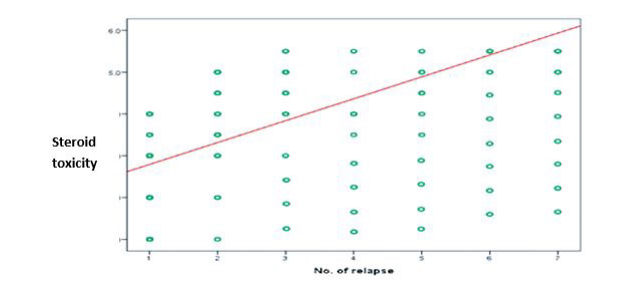
Pearson’s correlation test showed positive correlation. Here,r = 0.777 and p = < 0.001, that is the less the number of relapses, less
the steroid toxicity Figure 5: Correlation between the number of relapses with steroid toxicity |
Introduction
Nephrotic syndrome is a common and chronic disease in children. It can be defined as massive proteinuria, hypoalbuminemia, hypercholesterolemia and generalized oedema. Nephrotic range proteinuria is defined as proteinuria exceeding [1] gm/m²/day or spot urinary protein to creatinine ratio exceeding 2. The prevalence1 of this disease globally 12-16 cases per 100,000 children with incidence 2 to 7. The epidemiology shows higher incidence of nephrotic syndrome in children from Asia. [2] The condition is primary 95% and due to other causes 5% approximately [3,4].
Nephrotic syndrome is a disease of relapse and remission. During relapse patient may require hospitalization but during remission home care is essential. So management of Nephrotic syndrome requires both hospital and home care. Home care includes dietary management, weight measurement, bed side urinary protein detection and importance of medication intake, observe for any complications.
Shiau Chuen Diong et al. [5] shows parental knowledge on nephrotic syndrome and number of disease relapse is important for early recognition and treatment of relapse to prevent the complications. The parents should have knowledge about the symptoms of nephrotic syndrome, about the diet of the patients, bed side urine examination procedure and medication. Along with the knowledge, parent’s attitude towards the disease is important for the home care.
Chao et al6 concluded that the disease related knowledge of parents of children with nephrotic syndrome should be improved. By giving information, parent’s knowledge can be increased which reduce the number of relapses. Parental knowledge on nephrotic syndrome was not only associated with parental educational level but also number of disease recurrence. A study by Sarika et al [7] on 60 parents regarding their knowledge and practices on home management of children with nephrotic syndrome at three selected hospitals in Haryana, India, found that the majority of the parents (80%) had below average knowledge regarding home management of children with nephrotic syndrome. Practice of home care of nephrotic syndrome depends upon the knowledge and attitude of the parents.
Hakim et al [8] concludes parents of children with frequent relapses had higher knowledge in comparison to parents of children with infrequent attack. So knowledge, attitude and practice of parents varies from initial episode to subsequent attack. Knowledge and practice regarding home management much higher among the conscious and educated parents of developed country than the developing country. After implementation of educational programme there is significant improvement in mother’s knowledge and health care practices in children with nephrotic syndrome [9].
Inadequate parental knowledge on the disease impairs early detection of relapse and it leads to delayed treatment. Good education and communication to the family is important especially during hospital admission on initial diagnosis. This helps them to recognize the problem and seeking of the treatment [10].
Nagat F. Abolwafa et al [9] shows a positive co-relation between knowledge and practices of parents regarding home management. Upgrading parental awareness and knowledge by providing comprehensive and necessary information about the disease can greatly improve the quality of the cares levels and to live healthy and productive life [11].
Rationale
Nephrotic syndrome is one of the common nephrological problems of children. For proper management, parent’s knowledge and home practice is essential. Many studies are available regarding the management strategy, but very little information is available about the parental knowledge and practices regarding the home management of nephrotic syndrome. Parents acquire more knowledge with more relapses, however our aim is to give a good knowledge to the parents regardless the frequency of relapses. As knowledgeable parents from the beginning of their children’s disease course can prevent complication. Before enriching parent’s knowledge regarding the home care we have to assess their knowledge level. It will definitely help us to understand the present situation of knowledge, attitude and practice of parents regarding the home management of nephrotic syndrome in Bangladesh.
Objectives of the study
General objective:
To assess knowledge, attitude and practices of parents regarding the home management of nephrotic syndrome.
Specific objective:
1. To compare knowledge, attitude, and practice between the initial episode and subsequent relapse of nephrotic syndrome.
2. To find out the relationship between knowledge and home management practices of parents having a children with nephrotic syndrome.
3. To find out the relationship between the parent’s knowledge, attitude, practice and disease complications.
4. To find out the relationship between the parent’s knowledge, attitude, practice and number of relapse of nephrotic syndrome
5. To find out the relationship between infection and number of relapse of nephrotic syndrome.
6. To find out the relationship between the number of relapse and steroid toxicity of nephrotic syndrome.
Materials and Methods
This study was designed as a cross sectional comparative study carried out in the Department of Paediatric Nephrology, Cumilla Medical College Hospital, Cumilla conducted from April 2019 to October 2019. Study population were parents having children with nephrotic syndrome age ranging from 1-12 years were included. Initial attack were selected as controls and relapses were selected as cases. Physically and mentally ill nephrotic syndrome children were excluded. A total of 160 parent having children with nephritic syndrome were included in this study. Purposive consecutive sampling was done.
Study Procedure:
Nephrotic syndrome is diagnosed by taking detailed history, meticulous clinical examination and relevant investigation. Then it is categorized either it is 1stattack of nephrotic syndrome or relapse case. Structured knowledge questionnaire and practice rating scale was used to collect the data by using interview technique by a questionnaire from the parents of children with nephrotic syndrome. The questionnaire format included two parts. The first part was related to the mother's and child's demographic variables, such as mother's age, educational level, occupation, and child's age, age at the onset of the disease. The second part of the questionnaire format consists of structured items concerning parent’s knowledge, attitude and practices toward children having nephrotic syndrome. This part consists of 5 main sections and comprises of total 30 items, dealing with mother’s practices during edema, therapy, remission stage, child's food during acute phase and mothers' practices during the period of child's infection. Thereafter, each correct response was scored two (2) points each partially correct answer scored one (1) and each wrong response was scored zero (0). Total questions are five (5) in each section. The total score ranged from 0–10. Respondents with scores 0–4 were considered to have poor knowledge, those with 5- 6 points had a fair knowledge while those with 7–8 points had good knowledge, those with 9-10 points had very good knowledge. Compare of data regarding the knowledge, attitude and practice about the home management of nephrotic syndrome between the 1stattack and relapsing case. Inferential and descriptive analysis of data was done using SPSS version 22.
Ethical Consideration
The ethical issue was addressed duly. The aims and objectives of the study along with its procedure, methods, risks and benefits of this study were explained to the respondent and then informed written consent.
Results
This cross sectional comparative study was conducted in the Department of Pediatric Nephrology, Cumilla Medical College Hospital, Cumilla from April 2019 to October 2019 for a period of six (6) months to assess knowledge, attitude and practices regarding the home management of nephrotic syndrome. The results are as follows:
Discussion
Nephrotic syndrome (NS) is one of the common diseases in children and known among the vast majority of physicians in many countries. Literature about the epidemiology and incidence of NS vary, depending on the country and the ethnic origin of the children.
In this study, most of the patients were below or equal to 10 years in both groups. Mean age was almost similar in both groups (6.49 ± 2.67 years Vs 6.43 ± 3.06 years). In a study Franke et al [16] found most of the patients were below 10 years and mean age of the NS children was 5.5 ± 3.7 years which support our findings.
Male was predominant in both case (subsequent relapse) and control (initial episode) in this study. Male to female ratio was 1.7:1 and 1.9:1 in cases and controls. Similar finding was observed in study of Franke et.al.[16], and Sarkeret al. [17] where male to female ratio was 1.8:1 and 1.7:1 respectively
Mean score of knowledge about signs and symptoms was 6.41 ± 1.68 in cases which was significantly higher than controls (2.88 ± 0.96). Mean score of knowledge about diet was 7.69 ± 1.32 in cases which was significantly higher than controls (2.78 ± 1.16). Mean score of knowledge about weight was 7.40 ± 1.09 in cases which was significantly higher than controls (2.45 ± 1.04). Mean score of knowledge about urine examination was 7.49 ± 1.22 in cases which was significantly higher than controls (2.63 ± 1.32). Mean score of knowledge about medication was 7.19 ± 1.24 in cases which was significantly higher than controls (2.58 ± 1.61). Mean score of knowledge about infection and other complications was 6.73 ± 1.48 in cases which was significantly higher than controls (2.68 ± 1.05). Mean score of knowledge about follow up was 7.15 ± 1.18 in cases which was significantly higher than controls (2.65 ± 1.30). All parameters of knowledge regarding the home management of nephrotic syndrome were found significantly higher (P value < 0.001) in cases (subsequent relpase) than that of control (initial episode). Shiau Chuenet. al. [5] found that parents acquired more knowledge with more relapse, which support our result. Another study Elangbam A Devi et. al. [18] in Pune city of India shows that knowledge of parents depends on how many times patient got admitted into the hospital. Which also supports our result. Hospital admissions provides opportunity to obtain information on the disease from healthcare provider. [5] Nephrotic syndrome patients acquired the knowledge regarding the home management of nephrotic syndrome by experience and healthcare providers. That is why the knowledge was significantly higher in case than controls.
Mean score of practices of urine was 7.64 ± 1.29 in cases and 2.55 ± 1.22 in controls, there was significant difference between cases and controls (p< 0.001).Mean score of practices of dietary modification was 7.53 ± 1.51 in cases and 2.76 ± 1.34 in controls, there was significant difference between cases and controls (p< 0.001).Mean score of practices of skin care was 7.31 ± 1.50 in cases and 2.64 ± 1.42 in controls, there was significant difference between cases and controls (p< 0.001).Mean score of practices of prevention from infection and other complication was 7.20 ± 1.07 in cases and 2.56 ± 1.38 in controls, there was significant difference between cases and controls (p< 0.001).Mean score of practices of medication was 6.68 ± 1.37 in cases and 2.49 ± 1.13 in controls, there was significant difference between cases and controls (p< 0.001).Mean score of practices of daily living activity was 6.95 ± 1.34 in cases and 2.46 ± 1.29 in controls, there was significant difference between cases and controls (p< 0.001). Mean score of practices of emotional support was 6.41 ± 1.46 in cases and 2.50 ± 1.06 in controls, there was significant difference between cases and controls (p< 0.001).Mean score of practices of emotional support was 7.09 ± 1.14 in cases and 2.66 ± 1.15 in controls, there was significant difference between cases and controls (p< 0.001).Mean score of practices of home management was 6.35 ± 2.20 in cases and 2.45 ± 1.09 in controls, there was significant difference between cases and controls (p< 0.001). Chao et al.6 found similar type result which is in confrontation of our result. Parents of nephrotic syndrome patient learns the practices by repeated admission in nephrology ward for treatment of relapse.
Attitude regarding home management of nephrotic syndrome was found significantly higher in case than that of control (7.80 ± 1.10 vs 2.81 ± 0.85).
There was a significant positive correlation between the parental knowledge of home management of nephrotic syndrome with practice (r = 0.979 and p = < 0.001) of home care of nephrotic syndrome patients. Higher level of knowledge ensures more home management practice. Sarika et. al. [7], Nagat F. Abolwafaet. al. [9] and Hend Mohamed et. al.[12] shows same result which are in confrontation of our result.
Increase level of parental knowledge, attitude and practice significantly reduces the complication (r = - 0.806 and p = < 0.001). Diong SC et. al.5 2019 found that fair level of knowledge of parents prevents complications, which supports our result
There is a negative correlation between the level of knowledge, attitude and practice and number of relapse (r = -0.589 and p=< 0.001). Increased level of knowledge and home care reduces the frequency of relapse. Khider SI et. al. [19] founds number of relapse can be reduced by enhancing parents knowledge and ensuring proper home care, which supports our study.
There is a positive correlation between the infections and number of relapses r = 0.725 and p = < 0. 001.Study in the Bangalore, India Dakshayani B et. al. [20] 2018 concluded that infection during remission predicts future relapses. This supports our result. Another study in the tertiary center of Bangladesh Akter AHMM et. al. [21] 2020 shows that higher risk of relapse in boys with respiratory tract infection. This is in consistent to our study. Infection is one of the major predictor of relapse. So more infection causes more relapse.
There is a correlation between the number of relapse and steroid toxicity. Here we found a positive correlation between the number of relapse and steroid toxicity. Less number of relapse causes less steroid toxicity r = 0.777 and p < 0.001. A study Durkan AM et. al. [22] 2008 shows more frequency of relapses has more risk to develop adverse effects of corticosteroids. This has a similarity to our study.
Conclusions
Practices of home management of Nephrotic syndrome are related to knowledge, attitude and number of relapse. Relapse enriches knowledge and more knowledge ensures more practice of the home care.
Limitation of the study
The limitation of this present study was that the study was done in a single center and sample size is sma
Recommendations
• Further large scale study should be conducted.
• Multi centered study should be done.
References
- Eddy AA, Symons JM (2003) Nephrotic syndrome in childhood. The lancet 362: 629-39.
- McKinney PA, Feltbower RG, Brocklebank JT, Fitzpatrick MM (2001) Time trends and ethnic patterns of childhood nephrotic syndrome in Yorkshire, UK. Pedia Nephrol 16: 1040-4.
- Bagga A, Srivasta RN (2016) Nephrotic Syndrome. In: Srivasta, R.N., Bagga, A., editors. Pediatric Nephrology 6th ed. New Delhi; Jaypeek 191-233.
- Moudgil A, Nast CC, Bagga A, Wei L, Nurmamet A, et al. (2001) Association of parvovirus B19 infection with idiopathic collapsing glomerulopathy. Kidney international, 59: 2126-33.
- Shiau Chuen Diong, Syed Zulkifli Syed Zakaria, RahmahRasat, Wan Jazilah Wan Ismail, Med J Malaysia 74: 4.
- Chao XH, Wu SC, Jin R, Jin J, Ren XB (2010) Survey on cognition of parents of children patients with recurrent nephrotic syndrome and analysis of the related influencing factors. J Nursing 30: 71-5.
- Sarika. at al. (2017) Assessment of Knowledge and Practices of Parents Regarding Home Management of Children with Nephrotic Syndrome at Selected Hospitals of Haryana, India. Int. J. Curr. Microbiol. App. Sci 6: 1496-503
- Hakim A, Madhooshi S, Valavi E (2013) A study about knowledge of parents of children with nephrotic syndrome toward recurrence of disease. Jundishapur J Chronic Disease Care 2: 49- 55.
- Nagat F, Abolwafa, Yosria El-Sayed Hossein (2018) Am J Nursing Res 6: 244-52.
- Rudol M (1996) Rudolph's pediatrics. 2nd ed. Appleton&Bange; 1366-71.
- Mamatha M, Chandrashekar M, Sheela Williams (2015) Effectiveness of information booklet on knowledge regarding nephrotic syndrome and its home care management among parents of children with nephrotic syndrome at selected hospitals of Mysuru. Int. J. Nur. Edu. and Res 3: 284-7.
- Hend Mohamed Husain, Seham Guirguis Ragheb, Shimaa Fathy Mikky (2018) Mother’s Care for Children with Nephritic Syndrome at Home. Egyptian Journal of Health Care 9: 4
- Zhao J, Shen K, Xiang KL, Zhang GQ, Xie M, et al. (2013) The knowledge, attitudes and practices of parents of children with asthma in 29 cities of China: a multi-center study. BMC Pediat 13: 20.
- Suazan I, Khider M, Afkar R, Mohamed D, Naglaa F. (2017) Med. J. Cairo Univ 85: 515-22.
- Kliegman RM et. al. (2019) Nelson Text Book of Paediatrics 21st edition, Elsevier, New Delhi
- Franke I, Aydin M, Kurylowicz L, Lopez CEL, Ganschow R, et al. (2019) Clinical course & management of childhood nephrotic syndrome in Germany: a large epidemiological ESPED study. BMC Nephrol 20: 45.
- Sarker MN, Islam MMSU, Saad T, Shoma FN, Sharmin LS, et al. (2012) Risk factor for relapse in childhood nephrotic syndrome-a hospital based retrospective study. Faridpur Medical College J 7: 18-22.
- Elangbam Aruna Devi, Dr. Sneha Pitre, Bhagyashree Jogdeo (2017) Int J Appl Res 3: 610-5.
- Khider SI, Mohamed AR, Mahmoud NF, Essame R (2017) **Med. J. Cairo Univ 85: 515-22.
- Dakshayani B, Lakshmanna M, Premalatha R (2018) Predictors of frequent relapsing and steroid-dependent nephrotic syndrome in children. Turk Pediatri Ars 53: 24-30.
- Akter AHMM, Muinuddin G, Rahman MH, Roy RR, Begum A, et al. (2020) Predictors of Relapse in Idiopathic Nephrotic Syndrome in Children Presenting to a Tertiary Center, J Pediatric Nephrol 8: 23-7.
- Durkan AM, Hodson EM, Willis NS, et al. (2005) No corticosteroid treatment for nephrotic syndrome in children. Cochrane Database Syst Rev 2005; CD002290.
Artcle Information
Review Article
Received Date: June 05, 2025
Accepted Date: June 23, 2025
Published Date: June 30, 2025
Journal of Hepatology, Nephrology, Endocrinology Science
Volume 1 | Issue 1
Citation
MA Hossain, AU Amin, N Parvin, MM Ahmed, AKMH Rashid, et al. (2025) Knowledge, Attitude and Practices of Parents Regarding Home Management of Nephrotic Syndrome. J Hepatol, Nephrol, Endocrinol Sci 1: 103
Copyright
©2025 MA Hossain. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jhne.2025.1.103