

Research Article
Volume-1 Issue-1, 2021
Patterns and Differentials of Age at First Motherhood among Married Adolescents in Bangladesh
-
Received Date: August 14, 2021
-
Accepted Date: September 14, 2021
-
Published Date: September 16, 2021
Journal Information
Switch to Full Text Menu
Abstract
The main focus of this research study is to investigate the factors affecting the awareness of HIV/AIDS among ever-married women in Bangladesh. The study uses the nationally representative Bangladesh Demographic and Health Survey-2014 (BDHS) data set to accomplish this task fruitfully. The finding of this study illustrates that about 70% of the respondents have heard of AIDS. The multivariate hierarchical logistic regression analysis reveals that respondents’ education significantly impacts HIV/AIDS awareness and its transmission and prevention knowledge. The age of the respondents, place of residence, husband education, and occupation substantially impact the awareness of HIV/AIDS. The study further reflects that contraception is a predominant significant factor influencing the awareness of HIV/AIDS. Therefore, based on the results, it can be concluded that appropriate steps should be launched across the country to raise the awareness level of such a deadly disease for the reduction of its infection in Bangladesh.
Key words
HIV/AID; Awareness; Transmission; Prevention; Hierarchical logistic regression
Background Characteristics |
Categories |
N |
Percentage |
Ever heard of AIDS |
No |
4876 |
30.0 |
|
Yes |
11355 |
70.0 |
HIV/AIDS transmission Knowledge |
No |
291 |
2.6 |
|
Yes |
11041 |
97.4 |
HIV/AIDS prevention knowledge |
No |
841 |
7.5 |
|
Yes |
10443 |
92.5 |
Respondents current Age |
15-19 |
1631 |
10.0 |
|
20-24 |
2739 |
16.9 |
|
25-29 |
3032 |
18.7 |
|
30+ |
8829 |
54.4 |
Type of place of residence |
Urban |
5667 |
34.9 |
|
Rural |
10564 |
65.1 |
Division |
Barisal |
1932 |
11.9 |
|
Chittagong |
2571 |
15.8 |
|
Dhaka |
2807 |
17.3 |
|
Khulna |
2381 |
14.7 |
|
Rajshahi |
2314 |
14.3 |
|
Rangpur |
2307 |
14.2 |
|
Sylhet |
1919 |
11.8 |
Respondents education |
Illiterate |
3994 |
24.6 |
|
Primary |
4813 |
29.7 |
|
Secondary |
5935 |
36.6 |
|
Higher |
1489 |
9.2 |
Husbands education |
Illiterate |
4738 |
29.2 |
|
Primary |
4474 |
27.6 |
|
Secondary |
4669 |
28.8 |
|
Higher |
2350 |
14.5 |
Religion |
Islam |
14623 |
90.1 |
|
Others |
1608 |
9.9 |
Husbands occupation |
Agriculture |
4551 |
28.0 |
|
Service holder |
4691 |
28.9 |
|
Business |
3700 |
22.8 |
|
Others |
3289 |
20.3 |
Current marital status |
Married |
15258 |
94.0 |
|
Separated |
973 |
6.0 |
Current contraceptive method |
No |
6520 |
40.2 |
|
Yes |
9711 |
59.8 |
Socio-economic status |
Poor |
3701 |
22.8 |
|
Middle |
8753 |
53.9 |
|
Rich |
3777 |
23.3 |
Access to mass media |
No |
6145 |
37.9 |
|
Yes |
10086 |
62.1 |
Total |
|
16231 |
100% |
Background |
Ever heard |
HIV/AIDS transmission |
HIV/AIDS prevention |
||||||||||
No |
Yes |
χ2 |
P-value |
No |
Yes |
χ2 |
P-value |
No |
Yes |
χ2 |
P-value |
||
Respondents |
15-19 |
28.4 |
71.6 |
275.90 |
.000 |
2.4 |
97.6 |
5.55 |
.135 |
7.2 |
92.8 |
4.56 |
.207 |
20-24 |
22.2 |
77.8 |
2.2 |
97.8 |
8.1 |
91.9 |
|||||||
25-29 |
22.7 |
77.3 |
2.2 |
97.8 |
6.5 |
93.5 |
|||||||
30+ |
35.3 |
64.7 |
2.9 |
97.1 |
7.6 |
92.4 |
|||||||
Type of place |
Urban |
17.0 |
83.0 |
699.60 |
.000 |
2.0 |
98.0 |
9.44 |
.001 |
6.5 |
93.5 |
9.98 |
.001 |
Rural |
37.0 |
63.0 |
3.0 |
97.0 |
8.1 |
91.9 |
|||||||
Division |
Barisal |
27.3 |
72.7 |
351.07 |
.000 |
2.4 |
97.6 |
53.81 |
.000 |
6.7 |
93.3 |
67.79 |
.000 |
Chittagong |
29.7 |
70.3 |
2.4 |
97.6 |
9.4 |
90.6 |
|||||||
Dhaka |
22.8 |
77.2 |
2.4 |
97.6 |
4.6 |
95.4 |
|||||||
Khulna |
21.2 |
78.8 |
1.7 |
98.3 |
8.9 |
91.1 |
|||||||
Rajshahi |
34.0 |
66.0 |
1.9 |
98.1 |
5.1 |
94.9 |
|||||||
Rangpur |
39.4 |
60.6 |
2.6 |
97.4 |
8.7 |
91.3 |
|||||||
Sylhet |
38.9 |
61.1 |
5.6 |
94.4 |
9.9 |
90.1 |
|||||||
Respondents |
Illiterate |
59.2 |
40.8 |
321.37 |
.000 |
5.9 |
94.1 |
114.4 |
.000 |
8.5 |
91.5 |
10.94 |
.012 |
Primary |
36.1 |
63.9 |
3.1 |
96.9 |
8.0 |
92.0 |
|||||||
Secondary |
12.9 |
87.1 |
1.8 |
98.2 |
7.3 |
92.7 |
|||||||
Higher |
.7 |
99.3 |
.5 |
99.5 |
5.7 |
94.3 |
|||||||
Husband education |
Illiterate |
51.8 |
48.2 |
2224.78 |
.000 |
4.3 |
95.7 |
48.72 |
.000 |
8.1 |
91.9 |
7.05 |
.070 |
Primary |
34.3 |
65.7 |
2.9 |
97.1 |
7.2 |
92.8 |
|||||||
Secondary |
16.4 |
83.6 |
2.0 |
98.0 |
7.9 |
92.1 |
|||||||
Higher |
5.0% |
95.0 |
1.3 |
98.7 |
6.3 |
93.7 |
|||||||
Religion |
Islam |
29.6 |
70.4 |
14.27 |
.000 |
2.6 |
97.4 |
1.09 |
.173 |
7.2 |
92.8 |
7.14 |
.005 |
Others |
34.1 |
65.9 |
2.1 |
97.9 |
9.5 |
90.5 |
|||||||
Husbands |
Agriculture |
48.0 |
52.0 |
1359.23 |
.000 |
3.5 |
96.5 |
19.50 |
.000 |
8.1 |
91.9 |
7.11 |
.068 |
Service |
14.9 |
85.1 |
1.8 |
98.2 |
6.6 |
93.4 |
|||||||
Business |
22.3 |
77.7 |
2.5 |
97.5 |
7.7 |
92.3 |
|||||||
Others |
35.4 |
64.6 |
3.1 |
96.9 |
8.0 |
92.0 |
|||||||
Current |
Married |
29.2 |
70.8 |
79.59 |
.000 |
2.5 |
97.5 |
7.14 |
.009 |
7.4 |
92.6 |
.89 |
.194 |
Others |
42.8 |
57.2 |
4.3 |
95.7 |
8.5 |
91.5 |
|||||||
Access to mass |
No |
53.2 |
46.8 |
2534.45 |
.000 |
4.3 |
95.7 |
45.79 |
.000 |
8.3 |
91.7 |
4.11 |
.023 |
Yes |
15.9 |
84.1 |
2.0 |
98.0 |
7.2 |
92.8 |
|||||||
Socio- |
Poor |
52.8 |
47.2 |
1883.31 |
.000 |
4.6 |
95.4 |
46.98 |
.000 |
8.8 |
91.2 |
6.23 |
.044 |
Middle class |
16.2 |
83.8 |
1.9 |
98.1 |
7.1 |
92.9 |
|||||||
Rich |
39.9 |
|
3.3 |
96.7 |
7.6 |
92.4 |
|||||||
Current |
No |
33.8 |
66.2 |
74.602 |
.000 |
2.8 |
97.2 |
1.61 |
.114 |
7.5 |
92.5 |
.06 |
.413 |
Yes |
27.5 |
72.5 |
2.4 |
97.6 |
7.4 |
92.6 |
|||||||
Background Characteristics |
Model 1 |
Model 2 |
Model 3 |
Model 4 |
Confidence |
||
Odds |
Odds |
Odds |
Odds |
Lower |
Upper |
||
Respondents |
15-19 |
- |
- |
- |
- |
- |
- |
20-24 |
1.391*** |
1.598*** |
1.612*** |
1.575*** |
1.337 |
1.857 |
|
25-29 |
1.357*** |
1.996*** |
2.017*** |
1.950*** |
1.655 |
2.297 |
|
30+ |
.729*** |
1.614*** |
1.596*** |
1.567*** |
1.352 |
1.815 |
|
Respondents |
Illiterate |
-- |
- |
- |
- |
- |
- |
Primary |
|
2.112*** |
2.070*** |
2.037*** |
1.842 |
2.252 |
|
Secondary |
|
5.417*** |
5.541*** |
5.419*** |
4.766 |
6.161 |
|
|
49.407*** |
48.685*** |
47.299*** |
25.537 |
87.606 |
||
Husbands |
Illiterate |
-- |
- |
- |
- |
- |
- |
Primary |
|
1.137* |
1.145** |
1.137* |
1.028 |
1.257 |
|
Secondary |
|
1.679*** |
1.683*** |
1.700*** |
1.510 |
1.914 |
|
Higher |
|
2.102*** |
2.156*** |
2.200*** |
1.749 |
2.766 |
|
Husbands |
Agriculture |
-- |
- |
- |
- |
- |
- |
Service |
|
1.973*** |
1.796*** |
1.804*** |
1.597 |
2.036 |
|
Business |
|
1.632*** |
1.514*** |
1.504*** |
1.338 |
1.690 |
|
Others |
|
1.577*** |
1.463*** |
1.469*** |
1.317 |
1.638 |
|
Access to mass |
Yes |
-- |
2.673*** |
2.658*** |
2.655*** |
2.405 |
2.930 |
Socio-economic |
Poor |
-- |
- |
- |
- |
- |
- |
Middle |
|
1.505*** |
1.390*** |
1.388*** |
1.229 |
1.567 |
|
Rich |
|
1.075 |
1.055 |
1.049 |
.942 |
1.169 |
|
Type of placeof |
Rural |
|
|
.710*** |
.709*** |
.642 |
.784 |
Division |
Barisal |
-- |
-- |
- |
- |
- |
- |
Chittagong |
|
|
.595*** |
.607*** |
.518 |
.712 |
|
Dhaka |
|
|
.977 |
.980 |
.834 |
1.153 |
|
Khulna |
|
|
1.281** |
1.282** |
1.084 |
1.514 |
|
Rajshahi |
|
|
.575*** |
.567*** |
.483 |
.666 |
|
Rangpur |
|
|
.568*** |
.561*** |
.478 |
.658 |
|
Sylhet |
|
|
.723*** |
.748*** |
.635 |
.881 |
|
Religion |
Non-Muslim |
-- |
-- |
.748*** |
.740*** |
.645 |
.849 |
Current |
Yes |
-- |
-- |
-- |
1.242*** |
.766 |
1.073 |
Current marital |
Separate |
-- |
-- |
-- |
.907 |
1.138 |
1.356 |
-2LogLikelyhood(-2LL) |
19559.663 |
14728.806 |
14448.781 |
14417.203 |
|||
Chi-square |
281.554*** |
5112.412*** |
5392.437*** |
5424.015*** |
|||
Error Reduction |
281.554 |
4830.858 |
280.025 |
31.578 |
|||
Background Characteristics |
Model 1 |
Model 2 |
Model 3 |
Model 4 |
Confidence Interval |
||
Odds |
Odds |
Odds |
Odds |
Lower |
Upper |
||
Socio- economic |
Poor |
- |
- |
- |
- |
- |
- |
Middle |
2.521*** |
1.512** |
1.396* |
1.392* |
.965 |
2.006 |
|
Rich |
1.425** |
1.195 |
1.154 |
1.158 |
.826 |
1.623 |
|
Respondents education |
Illiterate |
-- |
- |
- |
- |
- |
- |
Primary |
1.829*** |
1.818*** |
1.795*** |
1.324 |
2.435 |
||
Secondary |
|
2.951*** |
2.912*** |
2.849*** |
2.016 |
4.026 |
|
|
11.015*** |
10.712*** |
10.389*** |
4.421 |
24.417 |
||
Husband education |
Illiterate |
-- |
- |
- |
- |
- |
- |
Primary |
|
1.064 |
1.081 |
1.073 |
.785 |
1.468 |
|
Secondary |
|
1.117 |
1.072 |
1.072 |
.755 |
1.522 |
|
Higher |
.848 |
.805 |
.811 |
.485 |
1.354 |
||
Husband occupation |
Agriculture |
-- |
- |
- |
- |
- |
- |
Service |
|
1.155 |
1.222 |
1.223 |
.856 |
1.748 |
|
Business |
|
.954 |
1.000 |
1.004 |
.710 |
1.421 |
|
Others |
|
1.079 |
1.102 |
1.102 |
.783 |
1.550 |
|
Access to |
Yes |
-- |
1.336* |
1.326* |
1.330* |
.982 |
1.800 |
Type of place |
Rural |
-- |
-- |
.901 |
.893 |
.677 |
1.178 |
Division |
Barisal |
-- |
-- |
- |
- |
- |
- |
Chittagong |
|
|
.864 |
.864 |
.540 |
1.381 |
|
Dhaka |
|
|
.939 |
.940 |
.595 |
1.485 |
|
Khulna |
|
|
1.465 |
1.475 |
.888 |
2.450 |
|
Rajshahi |
|
|
1.197 |
1.194 |
.712 |
2.002 |
|
Rangpur |
|
|
.945 |
.942 |
.577 |
1.538 |
|
Sylhet |
|
|
.453*** |
.456*** |
.295 |
.706 |
|
Current |
Separated |
-- |
-- |
-- |
.778 |
.501 |
1.207 |
-2LogLikelyhood(-2LL) |
2662.978 |
2572.119 |
2537.087 |
2535.901 |
|||
Chi-square |
42.805*** |
133.664*** |
168.696*** |
169.881*** |
|||
Error Reduction |
42.805 |
90.859 |
35.032 |
1.186 |
|||
Background characteristic |
Model 1 |
Model 2 |
Model 3 |
Confidence |
||
Odds |
Odds |
Odds |
Lower |
Upper |
||
S o cio-e co n o mic |
Poor |
- |
- |
- |
- |
- |
Middle |
1.269** |
1.155 |
1.098 |
.871 |
1.386 |
|
Rich |
1.172 |
1.140 |
1.127 |
.891 |
1.425 |
|
R e s p o n d e n t s |
Illiterate |
-- |
- |
- |
- |
- |
Primary |
1.062 |
1.058 |
.849 |
1.320 |
||
Secondary |
|
1.140 |
1.175 |
.953 |
1.450 |
|
|
1.472*** |
1.434** |
1.069 |
1.923 |
||
Access to mass media |
Yes |
-- |
1.049 |
.993 |
.817 |
1.207 |
Type of place of |
Rural |
-- |
-- |
.860* |
.735 |
1.006 |
Division |
Barisal |
|
|
- |
- |
- |
Chittagong |
|
|
.678*** |
.518 |
.886 |
|
Dhaka |
|
|
1.457** |
1.083 |
1.961 |
|
Khulna |
-- |
-- |
.728** |
.557 |
.951 |
|
Rajshahi |
|
|
1.306* |
.954 |
1.788 |
|
Rangpur |
|
|
.751** |
.565 |
.998 |
|
Sylhet |
|
|
.665*** |
.498 |
.886 |
|
-2LogLikelyhood(-2LL) |
5979.083 |
5970.482 |
5897.972 |
|||
Chi-square |
6.015** |
14.616** |
87.127*** |
|||
Error Reduction |
6.015 |
8.602 |
72.510 |
|||
 |
| Figure 1 |
Introduction
Acquired Immune Deficiency Syndrome (AIDS) is a deadly disease that leads to human life death. AIDS is an illness caused by a virus called HIV, which stands for Human Immunodeficiency Virus. Once someone is infected with HIV, the virus will remain in the body for the whole life. No cure or even no vaccine invented yet to prevent people from its infection. HIV attacks the CD4 cell (T cell), which helps the immune system fight off the infection. In addition, HIV reduces the number of CD4 cells in the body, and gradually the human immune system becomes weak and unable to fight off other opportunistic diseases. These opportunistic infections take advantage of a fragile immune system and gradually lead to the disease like AIDS.
Moreover, AIDS is the stage of infection that occurs when the immune system is badly damaged, and the human body becomes vulnerable to opportunistic infections, and life gradually falls at the tremendous risk of death. The first case of AIDS was officially avowed in the USA on June 5, 1981 (“Pneumocystis Pneumonia -- Los Angeles,” 1981); since then, the world experiencing a terrific health risk. At the end of 2020, 37.6 million people living with HIV worldwide (Global HIV & AIDS Statistics — Fact Sheet | UNAIDS, n.d.) [1]. Globally, the number of new HIV infections was 2.1 million, and the number of death due to AIDS was 1.1 million in 2015 (Granich et al., 2017) [2]. Since the beginning of this epidemic, the number of people infected with AIDS is 78 million, and 35 million people have died due to AIDS in the world [2]. In the Asia Pacific, the estimated number of people living with HIV was 5.1 million, and the ever prevalence rate was 0.2% in 2015 (Prevention Gap Report | UNAIDS, n.d.) [3]. In 2015, the number of death due to AIDS was 0.18 million, and the estimated number of new HIV infections was 0.3 million in the Asia Pacific (Smith & Tan, 2018) [4]. HIV/AIDS is a deadly epidemic in the current world and causing death in a great amount, so as this continuation, Bangladesh is not out of this consequence. Although Bangladesh is still a low prevalence country compared to other neighbouring countries and other countries globally, attention should be kept on spreading this dangerous disease, and regular monitoring is essential. Different studies reported that the current prevalence rate of HIV/AIDS in Bangladesh is still remains less than 0.01% (Faruk, 2017; UNAIDS HIV Data and Estimates | UNAIDS, n.d.) [5]. The first case of HIV/ AIDS in Bangladesh was detected in 1989 (Dhaka et al., 2009). The total number of new HIV infection decreases from 445 in 2014 to 433 in 2011. However, the number of new AIDS case (51) remain same in both period but the number of death due to AIDS increases to 91 in 2014 from 84 in 2011 [6-10]. Thus, it is very important to know the current scenario of awareness, knowledge, and attitude towards the HIV/AIDS epidemic in Bangladesh. Keeping it in view, it is immensely important to extensively study the awareness of HIV/AIDS along with its transmission and prevention knowledge because this disease is vulnerable due to high-risk factors in densely populated countries like Bangladesh. Therefore, this research paper attempts to extensively study the awareness of HIV/AIDS along with its transmission and prevention knowledge among ever-married women in Bangladesh.
Methodology
This research work is based on the Bangladesh Demographic and Health Survey 2014 data set. The survey was carried out under the authority of the national institute of population research and training (NIPORT). A detailed description of the survey data collection procedure and sample design can be obtained elsewhere [10]. In this survey, a total of 16,231 ever-married women were interviewed out of 17,863. First of all, HIV/AIDS awareness level is measured from these 16,231 female respondents. Secondly, to assess the comprehensive transmission and prevention knowledge of HIV/AIDS, mutually exclusive sub-samples of 11,332 and 11,284 married women who have heard of HIV/AIDS are considered, respectively, among all respondents.
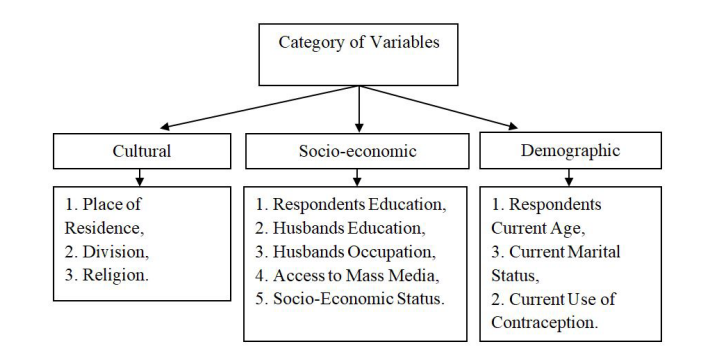
To examine the significant association between the HIV/AIDS awareness and available explanatory variables, χ2- statistic is computed after constructing contingency tables at 5% level of significance. Thereafter, the multivariate hierarchical logistic regression analysis was employed to identify the significant risk or prognostic factors of HIV/AIDS awareness, transmission, and prevention knowledge considering the variables found significant in bivariate analysis. In order to apply the hierarchical logistic regression in different models, the variables considered in this analysis are categorized into three sub-groups accordingly and presented in the following framework.
These groups of variables were entered into the regression in a stepwise fashion following a cultural, sociological and demographic hierarchy of their effect on dependent variables [11].
Results
HIV/AIDS is one of the deadliest diseases in the world. Therefore, in Bangladesh, it is very important to thoroughly analyze its
awareness, transmission, and prevention for the clear perception of the people. Therefore, at the outset, the percentage distribution of the sampled respondents regarding ever heard of HIV/AIDS by their background characteristics is analyzed and presented in Table 1. Table 1 shows that 70% of the respondents have heard of AIDS, which states that 70% of the respondents are aware of HIV/AIDS. Among the respondents who have heard of AIDS, 97.4 % know how HIV can be transmitted, and 92.5% know how to prevent it from the transmission. 54.4% of the respondents selected in this study are age above 30, and 65.1% of respondents live in rural areas. Findings in Table 1 reveal that 17.3% of the respondents are from Dhaka, followed by Chittagong (15.8%) and the lowest in Sylhet (11.8%). In the context of education, only 9.2% of respondents are highly educated whereas, 14.5% of their husbands are also highly educated.The result in Table 1 elucidates that 29.2% of husbands of the respondents are illiterate. Percentage distribution also shows that 90.1% of the respondents are Muslim, and a maximum of about 29% husbands of the respondents are service holders. The results of the study also show that 59.8% of the respondents use contraception. In Bangladesh, 53.9% of the respondents belong to the middle socioeconomic stratum, and only 62.1% have access to mass media. The findings at a glance reflect that the overall level of heard of HIV/AIDS is somewhat encouraging, but the current level should be raised to protect them from this kind of disease.
Besides the percentage distribution of the respondents by background characteristics, it is essential to examine whether there is any significant association between awareness, transmission, and prevention knowledge of HIV/AIDS with explanatory variables considered in the analysis. Therefore, to investigate whether there is an association between awareness, transmission, and prevention knowledge of HIV/AIDS and available explanatory variables, contingency tables and chisquare test statistic along with corresponding p-values are computed and given in Table 2.
Findings in the Table 2 reveal that the variables-respondents current age, type of place of residence, division, husband education, religion, husband occupation, and current marital status are significantly associated with HIV/AIDS awareness. Similarly, access to mass media, socioeconomic status, and current contraceptive use significantly connected to HIV/AIDS awareness at a 5% significance level. In addition, the variables; type of place of residence, division, respondents’ education, husbands’ education and occupation, current marital status, access to mass media, and socioeconomic status are found to have a significant association with the comprehensive knowledge of HIV/AIDS transmission. Moreover, the explanatory variables found to have a significant association with HIV/ AIDS prevention knowledge are; type of residence, division, respondents’ education, religion, access to mass media, and socioeconomic status.
The results of this study illustrate that about 70% of females are aware of HIV/AIDS in Bangladesh and 97.4% of them have HIV/AIDS transmission knowledge, and 92.5% have HIV/AIDS prevention knowledge. From Table 2 the differentials by background characteristics of the awareness of HIV/AIDS indicate that 99.3% of the highly educated respondents are aware of AIDS, followed by those whose husbands are highly educated (95.0%). Only 46.8% of respondents who have no access to mass media are aware of AIDS, followed by poor (47.2%). Therefore, mass media campaigns should be strengthened to increase the level of awareness of HIV/AIDS. Differentials
by background characteristics of the HIV/AIDS transmission and prevention knowledge among the respondents who have heard of AIDS reveals that the level of HIV/AIDS transmission knowledge is high among highly educated respondents (99.5%), followed by those whose husbands are highly educated (98.7%). HIV transmission knowledge is found relatively lower among the respondents whose husbands are illiterate (94.1%).Moreover, HIV/AIDS prevention knowledge is found high among the respondents of the Dhaka division (95.4%), followed by the respondents living in the Rajshahi region (94.9%), and prevention knowledge is found low among the respondents living in the Sylhet division (90.1%) and among non-Muslim (90.5%).
Besides the association of attributes, the determination of risk or prognostic factors of HIV/AIDS awareness, its transmission, and prevention knowledge, the application of multivariate analysis is inevitable. The hierarchical logistic regression is appropriate because this method does not require any distributional assumptions of the explanatory variables. Moreover, it can be
used for qualitative, quantitative, and mix of both qualitative and quantitative variables. The hierarchical logistic regression analysis results about awareness of HIV/AIDS are presented in Table 3. The findings of hierarchical logistic regression in Table 3 elucidate that the age of women has a significant impact on the awareness of HIV/AIDS. The age group, 25-29 years, is more knowledgeable about HIV/AIDS. The odds ratio of 1.95 indicates that the respondents within the age group 25-29 are approximately two times more exposed to have knowledge about HIV/AIDS compared to the reference age group of 15-19 years. The result also reveals that the highly educated respondents are 47 times more knowledgeable than those who are illiterate. Husbands education seems to have a significant influence on the awareness of HIV/AIDS in Bangladesh. Husbands' educational level is also found to have a significant impact on HIV/AIDS awareness. The odds ratio of 2.2 states that the respondents whose husbands are highly educated are 2.2 times more likely to know about HIV/AIDS than those whose husbands are illiterate. In an earlier study, knowledge of AIDS was strongly and positively associated with the education of female adolescents and their husbands and varied significantly across different parts of the country (Rahman et al., 2009). Like respondents education, husbands' occupation is also found to impact the awareness of HIV/AIDS significantly.The hierarchical logistic regression shows that the respondents whose husbands are service holders are approximately 1.81 times more knowledgeable about HIV/AIDS than their agriculturist counterparts. The respondents who have access to mass media are 2.66 times more knowledgeable about HIV/AIDS compared to the respondents who do not have any access to media. A study found that knowledge on HIV/AIDS was higher among relatively older and urban residents who had access to television or radio and whose husbands were using contraception (Rahman et al., 2009). The result shows that the respondents who belong to the middle-class stratum have more knowledge than any other socioeconomic status group. As expected of a place of residence has a significant influence on the awareness of HIV/AIDS in Bangladesh. The respondents who live in rural area are 0.71 times less likely to know about HIV/AIDS. However, overall, the administrative division has a significant influence on the awareness of HIV/ AIDS. The odds ratio of 1.28 indicates that the respondents of the Khulna division are 1.28 times more likely to know about HIV/AIDS as compared to the respondents of the Barisal region. The religion of the sampled women also influences the awareness of HIV/AIDS. The Muslim respondents are more knowledgeable than their non-Muslim counterparts. The respondents who use contraceptives are 1.24 times more likely to know about HIV/AIDS than the respondents who do not use any contraceptive methods in Bangladesh. The hierarchical logistic regression for assessing the awareness about HIV transmission knowledge and associated independent variables is given in Table 4. Results of hierarchical logistic regression revealed that the education of the respondents has a great influence on the awareness of HIV transmission. The result also reveals that the highly educated respondents are 10.39 times more likely to know about HIV transmission than those who are illiterate.
The hierarchical logistic regression illustrates that among the administrative division the Sylhet division shows only significant effect on HIV transmission knowledge and all other remains insignificant. But the respondents of the Rajshahi division have more knowledge about HIV than the respondents of other divisions. Hence it can be said that the administrative division is indirectly influencing the awareness of HIV transmission. Access to mass media has a slight impact on the knowledge of HIV transmission, as it is considered significant with a 10% level of significance. The respondents with middle socioeconomic status are 1.39 times more knowledgeable about HIV transmission than the respondents who are poor. The hierarchical logistic regression reveals that the other predictor variables such as husband educational level and husband occupation are indirectly related to HIV transmission knowledge. The hierarchical logistic regression applied to find the factors influencing HIV/AIDS prevention knowledge have shown in Table 5.
From Table 5, we found that the administrative division highly significantly influences HIV/AIDS prevention awareness. The respondents of the Dhaka division are found to have more knowledge about HIV/AIDS prevention than other divisions, and the respondents of the Rajshahi division are also found to have higher knowledge about HIV/AIDS prevention than other divisions except for Dhaka. The respondents’ education is also a significant factor that significantly impacts the awareness of HIV/AIDS prevention knowledge. The result of the hierarchical logistic regression reveals that the respondents who are highly educated are 1.43 times more likely to know about HIV/AIDS prevention knowledge. Furthermore, the type of place of residence is found to have a relationship with HIV/ AIDS prevention knowledge. The urban respondents are more knowledgeable than the rural respondents.
The hierarchical logistic regression also reveals that the predictor variables Access to Mass Media and Socio-Economic Status are indirectly influence the awareness of HIV/AIDS prevention knowledge.Discussion
Among the factors considered in this analysis, the respondents’ education is found very significant predictor in explaining the awareness of HIV/AIDS. A major factor that significantly influences HIV/AIDS awareness and highly and positively influences HIV/AIDS transmission and prevention knowledge is respondents’ education. The respondents who are highly educated are more knowledgeable about HIV/AIDS. Studies conducted in Bangladesh (Health Popul Nutr ; Khan & Nutr, 2002; Hossain et al., 2014; Khan et al., 1997; Mou et al., 2015; Nazrul Islam Mondal et al., 2012; Sarafian, 2012) [11,12,13,14,15,16] found that knowledge on AIDS was strongly and positively associated with education. This result is in the same direction with also an earlier study (Health Popul Nutr ; Khan & Nutr, 2002) [11]. In Bangladesh, people do not like to talk about HIV/AIDS as it is related to sexuality and other illegal activities, so there is a very narrow space to know about HIV/AIDS. A study conducted in Northan Ethiopia found that the respondents who discuss HIV/AIDS are less likely to be positive (Mehari, 2021) [17]. Hence, the people who are secondary or highly educated can read more extra academic papers, pamphlets, and storybooks from which they can come to know about HIV/AIDS epidemic and gather knowledge about its transmission and prevention process. Like education, access to mass media is also an important factor that significantly influences the awareness of HIV/AIDS. A recent study also suggested that mass media campaigns may be an important tool to increase the knowledge of HIV/ AIDS (Nazrul Islam Mondal et al., 2012) [15]. Media like TVs, newspapers, and radio can play a vital role in increasing the awareness level of HIV/AIDS. Nowadays, most of the people in Bangladesh and around the world have a tendency on media as entertainment. As most media proclaim different awareness-raising programs, including HIV/AIDS, the mass people can come to know about such kind of disease. Hence, it can be concluded that access to mass media is one of the key factors that greatly influence awareness of HIV/AIDS. The type of place of residence has a significant and positive influence on the awareness of HIV/AIDS. It also impacts comprehensive knowledge of HIV/AIDS, along with its transmission and prevention. Urban areas are adorned with modern facilities with hospitals, schools, universities, community centres, and greater mass media exposure; hence, the respondents who live in the urban area are more knowledgeable about HIV/ AIDS. Therefore, the campaign should be strengthened in the vast rural areas about the awareness of HIV/AIDS.
Husbands’ occupation influences the primary awareness of HIV/AIDS but not on transmission and prevention knowledge. The administrative division is found to impact the awareness of HIV/AIDS significantly. It is also significant for both HIV/AIDS transmission and prevention knowledge, and this may be due to wide variation of socioeconomic and geographical settings. Findings show that the respondents of the Khulna division are more knowledgeable than other divisions, but in the case of HIV prevention knowledge, the Dhaka division is found to have more knowledge. Since most at-risk groups of HIV/AIDS live in Dhaka city, the overall awareness level should increase in Dhaka city. Comparative findings confirm that the respondents of Khulna city are more knowledgeable about HIV/AIDS. Husband education is positively associated with the awareness of HIV/AIDS. It is seen from the result that the respondents whose husbands are highly educated are more knowledgeable about HIV/AIDS. This may be because the respondents must discuss the matter about sexuality and the STIs related to HIV/ AIDS; hence, the respondents whose husbands are highly educated can provide more information and hence become more knowledgeable about the consequences of HIV/AIDS.
The age of the respondents has an impact on the awareness of HIV/AIDS but does not have an influence on the comprehensive knowledge on HIV/AIDS. The respondents' socioeconomic status is also associated with the awareness of HIV/AIDS, but it does not affect the comprehensive knowledge of HIV/ AIDS. Couples who use contraceptive methods are more knowledgeable about HIV/AIDS (Shariful Islam et al., 2015) [18], which means that the use of contraception has a significant influence on the awareness of HIV/AIDS in Bangladesh. Hence contraceptive use has a substantial influence on the awareness of HI/AIDS, but it does not have an impact on HIV/ AIDS transmission and prevention knowledge. The marital status of the respondents has a significant influence on the awareness of HIV/AIDS but no significant influence on HIV/ AIDS transmission and prevention knowledge. Thus, findings confirmed that the basic need to increase the awareness of HIV/AIDS in Bangladesh is education. Access to mass media, age, type of place of residence, husband’s education and occupation, socioeconomic status, and contraception have a significant influence on the awareness of HIV/AIDS in Bangladesh [19].
Conclusion
Thus, based on the findings obtained from the multidimensional analyses, concerned authorities should take fruitful measures to increase the peoples' educational level and socioeconomic conditions across the country. Moreover, electronic and print media campaigns should be strengthened regarding the consequences of HIV/AIDS. Furthermore, an increase in the contraceptive prevalence rate (CPR) could be an important significant factor for raising the awareness level of HIV/AIDS. Finally, it can be concluded that proper implementation of the recommendations given above is likely to raise awareness, transmission, and prevention knowledge of HIV/AIDS, which could be the best course of action for reducing its infection in Bangladesh.
Ethics statements
The National Institute of Population Research and Training (NIPORT) authority of the Ministry of Health and Family Welfare conducted the nationally representative Bangladesh Demographic and Health Survey 2014 (BDHS-2014). Mitra and Associates, a Bangladeshi research firm located in Dhaka, implemented the survey. As part of its international Demographic and Health Surveys Program (MEASURE DHS), the technical assistance to the project was provided by the ICF International of Calverton, Maryland, USA. The respondent provided their verbal consent in response to being read out an informed consent statement by the interviewer. The permission of the BDHS data set was available from https:// dhsprogram.com/data, and their user instructions were strictly followed. The NIPORT took ethical approval for the BDHS 2017-18 from the BMRC (Bangladesh Medical Research Council).
Acknowledgements
We acknowledge the Measure DHS (Demographic and Health Surveys) Data Archive, ICF. International, USA for access to all the seven rounds of the Bangladesh Demographic and Health Survey (1993–2018) data.
Statement of Authorship
MAK: Conceptualization, Methodology, Data collection, Formal analysis, Writing- Original draft preparation, Review & Editing, & Supervision. MOF: Conceptualization, Methodology, Software, Writing - Review & Editing. MSR: Writing- Original draft preparation, Review & Editing.
Funding
The authors received no specific funding for the research work
Declaration of Interest Statement
The authors declare that they have no conflicts of interest regarding this work or the publication of this article.
References
- UNAIDS (2021) Global HIV & AIDS statistics — Fact sheet, USA.
- Granich R, Williams B, Montaner J, Zuniga JM (2017) 90-90-90 and ending AIDS: necessary and feasible. Lancet. 390: 341-3.
- UNAIDS (2021) Prevention gap report, USA.
- Smith JD, Tan KL (2018) Workforce Considerations, Training, and Diseases of the Asia-Pacific Region.Otolaryngol Clin North Am 51: 659-65.
- Faruk O (2017) Trends of HIV/AIDS Epidemic and Awareness Levels in Bangladesh. International Journal on Data Science and Technology 3: 56.
- Dhaka A (2016) Bangladesh Demographic and Health Survey 2014 National Institute of Population Research and Training Ministry of Health and Family Welfare Dhaka, Bangladesh.
- Dhaka A, Measure Dhs B (2013) Bangladesh Demographic And Health Survey 2011 National Institute of Population Research and Training Dhaka, Bangladesh.
- Dhaka A, Road I, Mohammadpur BA (2009) Bangladesh Demographic and Health Survey 2007, Bangladesh.
- Thebodypro (1981) Pneumocystis Pneumonia -- Los Angeles, USA.
- Rahman MM, Kabir M, Shahidullah M (2009) Adolescent Knowledge and Awareness about AIDS/HIV and Factors Affecting Them In Bangladesh. Int J Ayub Med Coll Abbottabad 21.
- Khan J (2002) Knowledge on AIDS among Female Adolescents in Bangladesh: Evidence from the Bangladesh Demographic and Health Survey Data 20: 130-7.
- Hossain M, Mani KKC, Sidik SM, Shahar HK, Islam R (2014) Knowledge and awareness about STDs among women in Bangladesh. BMC Public Health 14: 775.
- Khan MA, Rahman M, Khanam PA, Barkat-e-Khuda, Kane TT, Ashraf A (1997) Awareness of sexually transmitted disease among women and service providers in rural Bangladesh. International Journal of STD and AIDS 8: 688-96.
- Mou S, Bhuiya F, Islam SS (2015) Knowledge and perceptions of sexually transmitted diseases, HIV/AIDS, and reproductive health among female students in Dhaka, Bangladesh. International Journal of Advanced Medical and Health Research 2: 9.
- Nazrul Islam Mondal M, Mahfuzar Rahman M, Obaidur Rahman M, Naznin Akter M (2012) Level of Awareness about HIV/AIDS among Ever Married Women in. Food and Public Health 2: 73-8.
- Sarafian I (2012) Process assessment of a peer education programme for HIV prevention among sex workers in Dhaka, Bangladesh : A social support framework. Social Science and Medicine 75: 668-75.
- Mehari M (2021) Human Immune Deficiency Virus Serostatus and Associated Factors Among Children of Adult Index Cases in Northern Ethiopia 699–707.
- Shariful Islam SM, Biswas T, Bhuiyan FA, Islam MA, Rahman MM, et al. (2015) Injecting Drug Users and Their Health SeekingBehavior: A Cross-Sectional Study in Dhaka, Bangladesh. Journal of Addiction 10.1155/2015/756579.
- UNAIDS (2021) HIV Data and estimates, USA.
Artcle Information
Research Article
Received Date: August 14, 2021
Accepted Date: September 14, 2021
Published Date: September 16, 2021
Patterns and Differentials of Age at First Motherhood among Married Adolescents in Bangladesh
Volume 1 | Issue 1
Citation
Faruk MO, Md. Karim A (2021) Patterns and Differentials of Age at First Motherhood among Married Adolescents in Bangladesh. World J Immunol Respir Med 1: 103
©2022 Faruk MO. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jmsr.2022.1.103