

Review Article
Volume-1 Issue-1, 2025
Tissue Engineering in Injured Facial Nerve: A Narrative Review
-
Received Date: August 03, 2025
-
Accepted Date: August 21, 2025
-
Published Date: August 28, 2025
Journal Information
Abstract
Study Design: Narrative review.
Objective: Most of the studies were based on the sciatic nerve rather than the facial nerve. In this narrative review, we evaluated the results of different types of stem cells, various types of biomaterials/scaffolds for fabricating tissue-engineered nerve including natural, synthetic hybrid polymers, and in combination with different growth factors. We have also reviewed whether stem cell-based tissueengineering promotes regeneration of facial nerve in the most recent and the most relevant studies to treat facial nerve injury that can help newcomers acquainted themselves with the field of tissue engineering.
Methods: Two electronic databases including Pubmed and Google scholar were extensively searched, and the results were reviewed and analyzed.
Conclusion: The study of tissue engineering for facial nerve injuries hold a promise for the successful treatment, because of their ability to differentiate into other types of cells and to improve axon function, as well, to enhance facial nerve regeneration. However, further research in human trials and larger sample size are needed to validate the therapeutic effects of tissue engineering for facial nerve injury.
Key words
Facial nerve injury; Facial nerve regeneration; Stems cells; Tissue engineering; Scaffold
Abbreviations: ADSCs: adipose-derived stem cells; bFGF: basic fibroblast growth factor; BMSC: bone marrow stem cells;BDNF: brain-derived neurotrophic factor; C/GP-NGF: chitosan--glycerophosphate-nerve growth factor; CNTF:ciliary neurotrophic factor; DPCs: dental pulp stem cells; e-PTFE: expanded polytetrafluoroethylene; FBTMSC: fetal brain tissue derived mesenchymal stem cells; GDNF: glial cell-derived neurotrophic factor; hUCS: human umbilical cord serum; HA: hyaluronic acid; NGF: nerve growth factor; NSCs: neural stem cells; NT-3: Neurotrophin-3; OSCs: olfactory Stem Cells; PLGA: poly Lactic-co-Glycolic Acid; PCL: polycaprolactone; PGA: polyglycolic acid; PGAt: polyglycolic acid tube; PLA: Polylactic acid; PTFE: polytetrafluoroethylene.
Natural polymers |
Type of Scaffold |
Seed cells used |
Animal model |
Diameter of facial nerve |
Result |
References |
Collagen |
Interposition of a collagen nerve |
Ten cats |
5 mm facial nerve gap |
Facial nerve repair |
85 |
|
Enhanced with laminin and neurotrophic factors (CNTF |
rats |
4 mm facial nerve gap |
Significant regeneration effect of facial nerve |
87 |
||
Incorporated with neurocytokines CNTF and bFGF |
mini-pigs |
35 mm facial nerve gap |
Promote facial nerve regeneration effectively |
88 |
||
Combined with CNTF |
12 mini-pigs |
10 mm facial nerve gap |
Promising effects on facial nerve |
89 |
||
NSCs |
rats |
8 mm facial nerve gap |
Facial nerve regeneration to a degree similar to the autologous nerve |
90 |
||
Immobilizing GDNF in collagen conduits |
rats |
8 mm facial nerve gap |
Improve facial nerve regeneration and results approached |
91 |
||
bFGF |
39 rabbits |
Crush or cut off |
Promote functional facial nerve recovery |
3 |
||
Gelatin |
Impregnated with |
rats |
7 mm facial nerve gap |
Regeneration of the |
98 |
|
OSCs |
mice |
Facial nerve palsy |
Recovery of the facial nerve |
99 |
||
Fibrin |
FBTMSC |
28 rats |
Traumatic facial paralysis |
Appropriate microenvironment for facial nerve |
102 |
|
Synthetic polymers |
Silk |
Silk fibroin as |
rats |
10-mm facial nerve gap |
Promote nerve |
104 |
Chitin |
NGF |
16 rabbits |
8 mm facial nerve gap |
Facial nerve |
106 |
|
Chitosan |
C/GP-NGF |
rats |
5 mm facial nerve gap |
Satisfying functional recovery of regenerated facial |
107 |
|
HA |
Embedding NSCs to HA-collagen conduit and NT-3 |
rabbit |
5 mm facial nerve gap |
Promote facial nerve regeneration |
46 |
|
PGA |
BMSC |
35 rats |
5 mm facial nerve gap |
Regeneration of the facial nerve was improved |
114 |
|
PGA–collagen |
rats |
10 mm facial nerve gap |
Functional recovery was obtained but inferior to that obtained with an |
115 |
||
PLA |
Nerve conduit |
rats |
7 mm facial nerve gap |
Induce facial nerve |
117 |
|
PLGA |
Filled with DPSCs |
rats |
7 mm facial nerve gap |
Promote facial nerve |
119 |
|
PCL |
PCL /collagen/ hUCS |
16 rats |
4 mm facial nerve gap |
Provides a favorable environment |
122 |
|
PTFE |
e-PTFE and collagen |
17 rabbits |
10 mm facial nerve gap |
May be effective in the repair of the facial nerve injury |
126 |
|
e-PTFE and undifferentiated |
7 dogs |
7 mm facial nerve gap |
Enhanced the neural repair |
128 |
 |
| Figure 1: Branches of the facial nerve |
 |
| Figure 2:Peripheral nerve anatomy |
 |
| Figure 3:Schematic representation of the classification of peripheral nerve injury. Seddon classified peripheral nerve injury severity as class I (neuropraxia), class II (axonotmesis) or class III (neurotmesis), while first- to fifth-degree classified by Sunderland |
 |
| Figure 4: Engineered scaffold Components for facial nerve regeneration. Polyglycolic acid (PGA); Polylactic acid (PLA); polycaprolactone (PCL). |
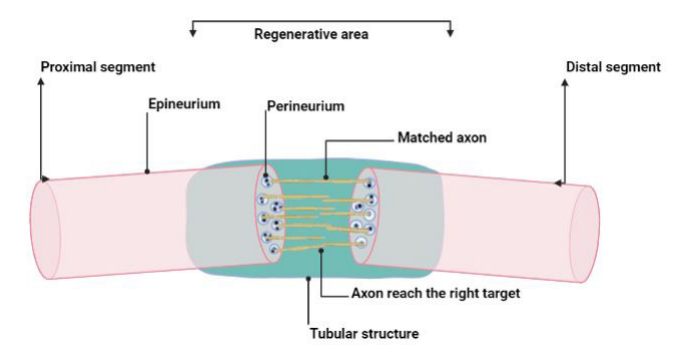 |
| Figure 5: Tubular structure of a conduit creates a microenvironment for axonal regeneration |
Introduction
Peripheral nerve injury is a widespread injury with over 300,000 cases registered in Europe and over 200,000 peripheral nerve repairs in the United States are performed each year. Although, irreversible functional impairment or complete functional loss often occurs, despite the regeneration capacity of the peripheral nervous system [1]. Furthermore, facial nerve injuries can be due to blunt, penetrating traumas and iatrogenic causes that are considered as the second most common, whereas, infections and tumors are rare [2]. Functional recovery still imposes a challenge to oral maxillofacial surgery after facial nerve injury. Nerve damage caused by crushing and cutting is more common in oral surgery using an extraoral approach than facial nerve segment defect injury. The psychological anguish caused by facial paralysis can be detrimental to a patient's personal and professional life [3].
End-to-end cooptation, cooptation with autologous or decellularized grafts, cooptation with nerve conduits, crossfacial nerve grafting, and free flap tissue transfer, or regional tissue transfer have all been used to treat facial nerve pathologies (congenital, tumor, iatrogenic operation-based) [4,5]. Besides, autologous nerve grafts have been accepted as the gold standard for repairing nerve defects, however, their disadvantages, such as sacrificing donor tissue and bad match in terms of nerve diameter, limit their clinical use [6]. Nerve conduits can be used to promote nerve regeneration in patients with nerve defects. Using only nerve conduits as a bridge between peripheral nerves injury results in nerve regeneration with a success rate of 50– 60% which is lower than that of autologous nerve grafts. The combination of axonal scaffolds and transplanted cells provides adequate support for neural regeneration, improves the success rate, and has been investigated as a technique to overcome surgical repair limitations [7,8].
Tissue engineering is the use of living cells, biomolecules, and/ or biomaterials by incorporating both biological and artificial components to provide a stronger, alternative means of treatment for tissue and organ damage such that a long-lasting repair is made [9]. A tissue-engineered artificial nerve is a bridge that acts as a physical and nutritional aid to repair nerve injury [10]. Skalak and Fox defined tissue engineering in 1988 as ‘the application of engineering and life sciences concepts and techniques to the basic understanding of structure-function relationships in normal and pathological mammalian tissues and the creation of biological replacements for the repair, maintenance or enhancement of functions’ [11]. Langer and Vacanti established three main pillars of tissue-engineering principles: (a) isolated cells and substitutescellular systems; (b) scaffolds, biomaterials, and/or matrices; and (c) bioactive molecules of tissue-inducing substances [12].
In the first pillar, the cellular system contains a wide variety of cells and most importantly, stem cells. Stem cells are undifferentiated reactive cells with varying degrees of plasticity for self-proliferation and differentiation [13]. The use of human mesenchymal stem cells (MSCs) for cell transplantation in peripheral nerves has shown that they can be differentiated into neural cells in vitro and transplanted into the injured facial nerve of the guinea pig to promote nerve regeneration [14].
The second pillar is the three-dimensional biomaterials or scaffolds that imitate the environment and natural extracellular matrix (ECM) of the place of implantation and provides shelter and structure for the cellular system. The most significant characteristics of biomaterials must be: (i) biocompatibility, which means the biomaterial itself is not liable to cause any harm to the living system and it is considered to be the key characteristic of a biomaterial; (ii) biofunctionality, because the biomaterial must have mechanical and physico-chemical properties appropriate to the function and use; and (iii) Sterilizability, specifically for polymeric materials which must be able to undergo sterilization processes [15].
The third pillar focuses on the bioactive molecules which can be signal molecules, oligonucleotides, and proteins that can promote cell migration, cell development, and/or differentiation. These bioactive molecules are classified into mitogens (stimulate cell division), growth factors (originally identified by their proliferation-inducing effects, but have multiple functions), and morphogens (control generation of tissue form) [16]. The neurotrophic effect of growth factors will indirectly impact the seed cells in the nerve conduit, whereas, nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and glial cell line-derived neurotrophic factor (GDNF) are the most frequently used [17].
In the current review, the source and application of stem cell therapy and scaffolds used to repair facial nerve were summarized and the recent trials of stem cell-based tissue-engineering in injured facial nerve were discussed.
Methods
Two electronic databases including Pubmed and google scholar have been extensively searched, and the results were reviewed and analyzed using the following terms: facial nerve injury, facial nerve regeneration, stems cells, tissue engineering, scaffold.
Literature Review
Facial Nerve
Anatomy
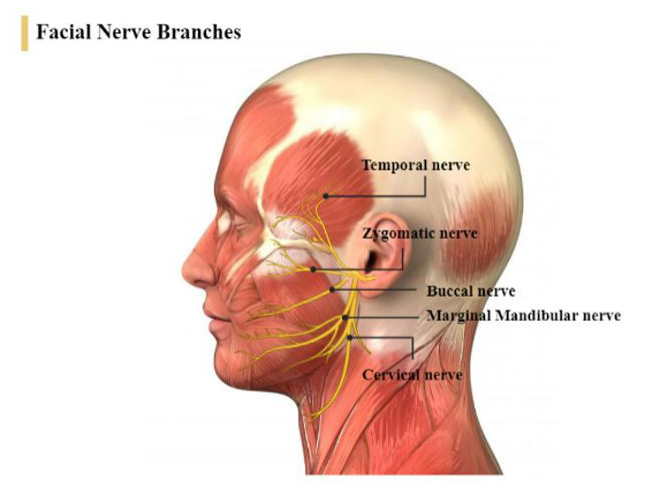
The facial nerve originates inside the pons in the facial nucleus; the motor fibers of cranial nerve VII are joined by those of the nervus intermedius before reaching the temporal bone via the internal auditory meatus. The nerve exits the temporal bone through the stylomastoid foramen then enters the parotid gland to divides into five main branches: the temporal, zygomatic, buccal, marginal mandibular, and cervical [18] (Figure 1).
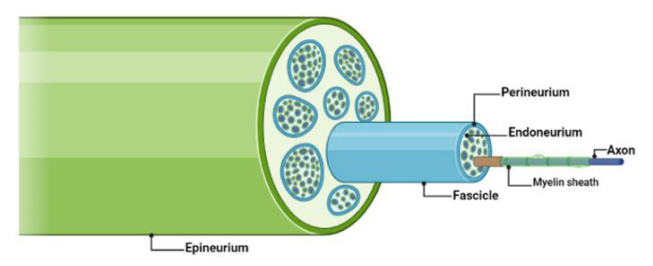
Within a nerve, multiple protective layers are surrounded by an assembly of axons, called fascicles: (i) Endoneurium represents the innermost layer covering individual axons and their related Schwann cells, which insulate axons with myelin to maintain the propagating ionic currents until recharged at intervening nodes of Ranvier; (ii) Perineurium that divides axons into neural fascicles; (iii) The outermost layer is the epineurium that provides tensile strength and structural support to maintain the robust anastomotic vascular supply of the nerve 4 (Figure 2).
Facial Nerve Injury Classification
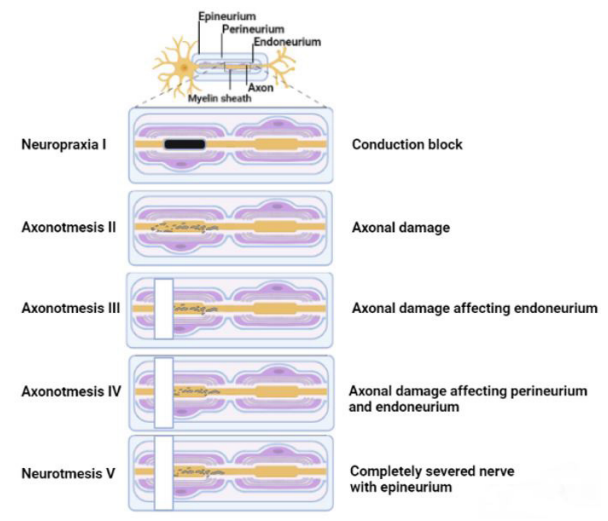
Nerve injuries were firstly categorized by Sir Herbert Seddon in 1943 into three classes of peripheral nerve injury: (i) Neuropraxia (class I) (“praxis” means “to do, to perform”), characterized by the segmentation of myelin, normally a result of compression without axon or perineurium disruption. The conduction of nerve impulses in the affected region is disrupted, motor and sensory connections are lost, but all morphological features of the nerve stump, including the endoneurium, perineurium, and epineurium, remain intact in neurapraxia. Wallerian degeneration does not occur in neurapraxia since the axon is not separated from the soma. Usually, it achieves full recovery of nerve conduction and function, and resolves itself within a few weeks, once the myelin is repaired; (ii) Axonotmesis (class II) (“tmesis” means “to cut”) involves axonal damage which arises from a crushing mechanism. The perineurium and endoneurium may be disrupted, while the epineurium is intact. Fascicular connective tissue and nerve integrity are not impaired in this situation but are accompanied by Wallerian degeneration in the axon stump distal to the injury site within 24–36 hours of peripheral nerve damage. Functional recovery is possible if the level of integrity of the physiological structure and organization retains of injured nerve stump. However, in most circumstances, self-regeneration is highly limited, and surgical intervention is necessary; (iii) Neurotmesis (class III) is a disturbance of the whole nerve and compromised sensory and functional recovery with the rupture of axon, myelin sheath, and connective tissues of the nerve trunk. Therefore, no spontaneous regeneration can occur and surgical reconstruction is necessary [19].
This classification was subsequently expanded by Sunderland to include five types of injuries, depending on the severity of the injury. The first-degree injury is close to Seddon's neurapraxia. Second, third and fourth-degree injuries are similar to Seddon’s axonotmesis, the distinction being the degree of nerve mesenchymal damage, whereas axonal damage without commitment of the endoneurium in Type II occurs and possible to achieve a full recovery, while in Type III lesions, axon impairment affecting the endoneurium, however in Type IV, there is perineurium damage besides endoneurium. Fifth-degree injury is similar to Seddon’s neurotmesis [20] (Figure 3).
Finally, a mixed type of lesion degree was described by Mackinnon and Dellon, a type VI in addition to the Sunderland classification and perhaps the most common type of lesion, with many layers of injury and not exactly a standard form as described by Sunderland. According to the type of lesion, the recovery potential and also the treatment approach may differ [21].
The facial nerve is the seventh (VII) cranial nerve, and contributes to communication, emotional expression, and oral competence while eating and drinking. It also plays a major role in nasal patency during respiration, eye closure, and hearing protection against noise exposure [4, 22]. In fact, facial nerve palsy, injury, or lacks of function are related to many etiological factors such as trauma (e.g., facial/skull fractures, lacerations, and penetrating injury), tumors, inflammatory or disease infectious (e.g., Bell’s palsy or Lyme disease), surgical injury or idiopathic causes [23]. Functional facial nerve abnormalities lead to physiological changes, speech and mastication disorders, as well as esthetic and psychological involvement leading to severe changes in selfesteem and social life [24].
Following facial nerve injury, the distal portions of axons detach from the trophic center (cell body) and degenerate in a process known as Wallerian degeneration. Alongside that, the axons extend from the proximal to distal stump through Schwann cell proliferation and eventually reinnervate their distal targets, presumably restoring function [25]. If there is a long distance between damaged ends following peripheral nerve injury and the end-end suture cannot be accomplished, an autogenous nerve graft is considered the ‘‘gold standard” therapeutic treatment for nerve regeneration [26]. However, a limited donor source for the repair method of autogenous nerve graft is a problem.
Additionally, Schwann cells are peripheral glial cells that contribute to the stabilization of the structure of the axon through the production of myelin. Schwann cells play a central role in nerve regeneration by releasing the growth factors required for neuronal maintenance [27]. However, using autologous Schwann cells as a cellular therapy for motor nerve injury is difficult for two reasons: (i) to obtain autologous Schwann cells, patient nerve tissue must be sacrificed; (ii) Schwann cells purification and expansion in culture is difficult. Therefore, Schwann cells derived from stem cells can serve as a possible strategy for accelerating nerve recovery by using immunologically matched induced pluripotent stem cells (iPSCs) precursors as the source [28].
New treatment modalities are still being created to increase patients' quality of life. In recent years, various tissue-engineered nerve grafts using stem cells and various types of biomaterials/ scaffolds have been developed, exhibiting some degree of regeneration of facial nerve defects [29].
Stem cell transplantation is a highly efficient therapeutic modality that uses tissue engineering in many different diseases. It has been shown that stem cells can be differentiated into the Schwann cell phenotype, which speeds up axonal regeneration and improves remyelination [30]. As well, stem cells enhance growth factor secretion in peripheral nerve injury, augmenting regeneration with anti-inflammatory activity, and replacing injured Schwann cells and motor neurons [31].
Certain biodegradable materials and pharmacological agents may help in nerve regeneration. These materials provide a protein-rich environment for stem cells, improve adhesion, and stimulate axonal growth [32].
Stem Cells Used For Facial Nerve Regeneration
Stem cells (SC) are undifferentiated cells that have the ability to differentiate after mitosis into any specialized cells. Stem cells can be classified into two major groups based on their source of origin: Embryonic and Adult stem cells. Also, stem cell classified based on the range of differentiation potentials into: (i) totipotent stem cells that are obtained from very early embryos which can differentiate into embryonic and extraembryonic tissues, therefore form an entire organism and the placenta;(ii) Pluripotent stem cells that can differentiate into the entire range of derivatives of all three embryonic germ layers namely, ectoderm, endoderm, and mesoderm, from which all tissues and organs develop but they do not have the ability to form embryos. They are classified into embryonic stem cells (ESC), perinatal Stem Cells (Umbilical Cord Stem Cells), and iPSCs; (iii) Multipotent stem cells include adult stem cells differentiate into specialized cell types present in a specific tissue or organ that can be differentiated into multi-cell lineages derivatives. A subset of multipotent adult stem cells arising from the mesoderm is MSCs that are able to differentiate into a variety of cell lineages that resemble chondrocytes, osteoblasts, myoblasts, adipocytes, and fibroblasts, as well as neuron‐like cells, endothelial cells, and cardiomyocytes, thus transdifferentiation occurs as a cell from one germ layer (mesoderm) differentiates into neuronal tissue (ectoderm) [31,33]; (iv) Oligopotent stem cells have the ability to self-renew and form two or more lineages within a specific tissue; for example, the pig's ocular surface, including the cornea, has been shown to contain oligopotent stem cells that produce individual colonies of corneal and conjunctival cells[34]; (v) Unipotent stem cells have the property of self-renewal but they just differentiate into a single cell type such as muscle stem cells [35].
However, under appropriate culture conditions, ESCs differentiate into a variety of cell types, and have a higher proliferation rate, as well higher production of NGF and vascular endothelial growth factor (VEGF) within a 3-D scaffold than a 2-D for a long period of time [36]. However, ESCs have ethical barriers, risks of immunogenicity, and teratocarcinoma formation, thus clinical application is impeded in human clinical application [37].
iPSCs generated by reprogramming somatic cells have largely pushed the progress of regenerative capacity. They can differentiate into neural crest stem cells or even Schwann cells with myelinating capabilities. However, they exhibit some similar characteristics to ESC such as malignant potential [38].
Wang et al. 2011, concluded in their study that the Schwannlike mesenchymal stem cell gave more positive results than in bone marrow stem cells (BMSCs) in axon regeneration and remyelination in rabbits with facial nerve damage [39].
However, different types of SC are used in facial nerve regeneration such as MSCs, BMSCs, neural stem cells (NSCs), olfactory stem cells (OSCs), adipose-derived stem cells (ADSCs), Human exfoliated deciduous teeth (SHED).
Bone marrow stem cells (BMSC)
MSCs are multipotent adult stem cells present in a variety of tissues including bone marrow, umbilical cord blood, peripheral blood, fallopian tube, and lung. BMSCs can be easily harvested using a standardized form of aspiration and then extended on a wide scale for subsequent applications [40]. Cultured fibroblastlike BMSCs were able to synthesize and release neurotrophic factors such as ciliary neurotrophic factor (CNTF), NGF, GDNF, BDNF, as well as ECM proteins such as collagen I, collagen IV, fibronectin, and laminin. Thus, there is an association between BMSC implantation factors and higher neurotrophic factor production. Furthermore, BMSC has been shown to differentiate in-vitro cultured from rat femurs into Schwann-like cells that have enhanced myelination in peripheral nerve repair [41].
Aggarwal S et al. harvested autologous bone marrow mononuclear stem cells from aspirated blood from iliac crest of eight patients with post-traumatic facial nerve paralysis. All patients who were subjected to stem cell implantation showed no adverse effects after more than 6 months of follow-up. It seems to be a promising modality for rehabilitation with patients suffering from post-traumatic facial nerve paralysis, but larger series with a control group is needed before recommending this modality for facial nerve paralysis [42]. Moreover, Wang et al. (2011) demonstrated the possibility of autologous BMSCs to transdifferentiate into Schwann-like cells, which were more effective in promoting rabbit facial nerve regeneration and myelination in newly regenerated axons and increasing the percentage of myelin-forming Schwann cells when combined with autologous vein conduits [39].
Wu L, showed that co-transplantation of BMSCs and monocytes (at the ratio of 1:30) in the brain stem of rats could repair the facial nerve axotomy and elevate the survival rate of facial neurons by alleviating the survival conditions for BMSCs, promoting an anti-inflammatory microenvironment by shifting the anti-/pro-inflammatory balance, regulating the chemotaxis and reducing the neuronal apoptosis. Chemokine stromalcell derived factor-1 (SDF-1), along with the CXC chemokine receptor 4 (CXCR4) expressed on the surface of stem cells or lymphocytes play an important role in the regulation of the inflammatory cells and stem cells, while co-transplantation significantly increases SDF-1/CXCR4 expression in the facial nerve nucleus, as a result of the chemotaxis effects, more BMSCs are recruited into it. This phenomenon is critical in inhibiting apoptotic processes of the facial neurons. Additionally, increased expression of CXCR4 on the surface of BMSCs could enhance BMSCs differentiation into the neuron-like cells or other neural cells in the microenvironment. These cells may either replace the apoptotic neurons or provide nutrients, ultimately reducing neuronal apoptosis throughout the facial nerve nucleus [43]. Thus, BMSCs areone of the most commonly used cell sources for nerve regeneration and showed promising results for facial nerve regeneration.
Neural stem cells (NSCs)
The subventricular zone (SVZ) and hippocampus are the main sources of adult NSC in the human brain. To obtain tissue from the SVZ or hippocampus, a craniotomy must be performed, which can result in large areas of surgical damage. Therefore, it is necessary to obtain Schwann cells or neural progenitor cells from other sources [44].
To be considered NSC, the cells must have the following properties: (i) they must be multipotent and capable to form all the nervous system cells and their subgroups, including oligodendrocytes, astrocytes, and neurons; (ii) to be able to differentiate into all nervous system cell lines, and they must be able to repopulate the damaged nervous system; (iii) they must be transplantable in series; and (iv) they must be self-renewable and capable of producing new cells with the same potential and properties [45]. An artificial nerve consisting of chitosan conduits, a natural polymer as epineurium filled with porous collagen sponges containing NSCs to repair a 10 mm defect in the rabbit facial nerve, and the result showed similar recovery as compared with nerves treated with autografts. Thus, NSCs may act as seed cells and can be used in artificial nerve to repair facial nerve defects, whereas, the three-dimensional artificial nerve act as scaffold and has good biocompatibility, thus preserving the microenvironmental stability of nerve regeneration and preventing the development of scar through neurologic defect [45].
NSCs have a special ability to differentiate into astrocytes, oligodendrocytes, and neurons even Schwann-like cells. Moreover, Neurotrophin-3 (NT-3), a neurotrophic factor in the nerve growth factor family of neurotrophins, helps in the growth, survival, and differentiation of current and new neurons and synapses both in vivo and in vitro. Zhang et al. used NSCs supplemented with hyaluronic acid (HA), collagen, and NT-3 in a rabbit model and regeneration of facial nerve injury was evident, with impressive growth of fascicles and nerve fibers.
The addition of NT-3 to NSCs embedded in a HA-collagen composite scaffold not only improved NSC differentiation and neurite outgrowth but also provided a growth factor to stimulate endogenous regeneration and reduce degeneration. This could be an alternative modality to treat peripheral nerve defects [46]. Human mastoid process bone marrow is rarely wasted in otitis media surgery for disease removal; however, MSCs from Human mastoid process bone marrow can differentiate into neuralinduced mesenchymal stem cells (nMSCs) in vitro. Additionally, platelet-rich plasma (PRP) consists of various neurotrophic factors and can be obtained easily and used promptly during surgery. Cho et al. concluded that nMSCs combined with PRP promotes facial nerve regeneration rather than administration of only stem cells in guinea pigs model, with anincreased expression of neurotrophic factors such as basic fibroblast growth factor (bFGF), NGF, angiopoietin-1, BDNF, GDNF, and NT-3 in the facial nerve fragment. This combination in peripheral nerve regeneration provides clinical application of an acute nerve injury [14].
As a result of the NSCs multipotential differentiation, high immigration ability, strong plasticity, high immigration capacity, and low immunogenicity, they have become another selectable seed cell in tissue-engineered artificial nerves [45].
Olfactory stem cells (OSCs)
Human OSCs in human olfactory mucosa are self-renewing that can be harvested from nasal biopsies, and can differentiate into neurons, astrocytes, and oligodendrocytes in vitro and induces regeneration and myelinization of nerves, axons as well can differentiate into nonneuronal cells in vivo in the meantime retaining their basic stem cell properties while replicating themselves. However, neurogenesis occurs throughout life in the human olfactory mucous membrane and hippocampus [45, 47]. A study by Batioglu-Karaaltin et al. showed an effective cell therapy modality for accelerating facial nerve regeneration by using human OSCs that could be the only available neural stem cells with conduit to treat facial nerve damage in a rat model [48].
Adipose-derived stem cells (ADSCs)
ADSCs are an attractive cell source for tissue regeneration due to their ability to self-renewal, high growth rate, and multipotent differentiation properties. They can be isolated from subcutaneous fat tissue easily by a safe and conventional liposuction procedure, also are easily purified, and are readily expanded in culture, and showed a good result in nerve repair [49].
ADSCs, which greatly improved nerve regeneration, have shown the capacity to facilitate angiogenesis and secrete a variety of growth factors and cytokines that can positively affect axonal regeneration in addition to their multipotent differentiation capacity. Erba et al. demonstrated that adipose stem cells enhance peripheral nerve regeneration in vivo by protecting the distal nerve end, where the majority of Schwann cell migration through the conduit takes place [50, 51].
ADSCs, which greatly improved nerve regeneration, have shown the capacity to facilitate angiogenesis and secrete a variety of growth factors and cytokines that can positively affect axonal regeneration in addition to their multipotent differentiation capacity. Erba et al. demonstrated that adipose stem cells enhance peripheral nerve regeneration in vivo by protecting the distal nerve end, where the majority of Schwann cell migration through the conduit takes place [50, 51].
In a study of Kamei w et al. a hybrid Polyglycolic Acid (PGA) nerve conduit containing ADSCs bridged nerves by end-toside neurorrhaphy has been used to regenerate facial nerve in a rat model, and ADSCs promoted nerve regeneration by (i) neurotrophic factors released from the artificial nerve conduit filled with ADSCs; and (ii) transformation of ADSCs into Schwann-like cells with released neurotrophic factors from facial and hypoglossal nerves at the host sites where epineural windows were created by end-to-side neurorrhaphy [54]. Abbas et al. indicated that ADSCs enhance axonal sprouting and increase the number of axons through the coaptation between the facial nerve and the nerve graft in a twelve rat model with facial paralysis. These findings indicate that administration of ADSCs caused each detached axon in the buccal branch of the facial nerve to give birth to an average of approximately three daughter axons that crossed the proximal coaptation site, also optimized myelination to achieve maximal functional and structural efficiency, and supported the functional integrity of denervated neuromuscular junctions. Additionally, immunohistochemistry was used to validate the existence of acetylcholine in the neuromuscular junctions in animals treated with ADSCs. Apart from being the primary excitatory neurotransmitter in the peripheral nervous system, acetylcholine may also induce neurite outgrowth and promote synaptic development [55]. Tan J et al. used approaches to knockdown a pro-fibrotic factor procollagen-lysine 1, 2-oxoglutarate 5-dioxygenase 1 (PLOD1) since ADSCs expressed high levels of PLOD1, by expression of either a short-hair interfering RNA for PLOD1 (shPLOD1) or a microRNA-449 (miR-449) that similarly reduced the fibrosis in the injured region, and a better therapeutic effects on facial nerve regeneration was observed [56].
Stromal vascular fraction (SVF) is best known for its angiogenic and anti-inflammatory effects, thus the authors reported facial nerve regeneration where silicone tubes filled with SVF were used as a bridge in rat nerve defect [57]. Despite the differences in their mechanisms, ADSCs and SVF were thought to have the same degree of nerve regeneration-promoting capacity. Consequently, the application of growth factors to the nerve defect site was observed to facilitate axonal regeneration in those studies [58].
On the other hand, Japanese researchers developed a preadipocyte cell line from mature mouse adipocytes in 2004 and name these cells “Dedifferentiated Fat (DFAT) cells” [59].
Following that, in 2008, the same group of researchers isolated human DFAT cells from subcutaneous fat expressing a multilineage potential [60]. Under proper inducing conditions in vitro and in vivo, DFAT cells are a largely homogeneous cell population (high purity), highly proliferative, and possess a multilineage ability for differentiation into various cell types. Furthermore, DFAT cells have a greater capacity to differentiate into chondrocytes, osteoblasts, and adipocytes than bone marrow-derived mesenchymal stem cells and/or adipose tissuederived stem cells. It has been documented that DFAT cells can be used in vivo to regenerate periodontal tissue, bone, peripheral nerve, muscle, cartilage, and fat tissue. The isolation of DFAT cells from the human buccal fat pad (BFP) is a minimally invasive procedure with few aesthetic complications for patients [61].
Kono et al. proved that DFAT and ADSC have similar immunephenotypes, but DFAT is more homogeneous than ADSC since DFAT is created by a ceiling culture [62]. Furthermore, immunostaining experiments have shown that neural stem cell markers such as nestin and SOX2 are present in DFAT cells, indicating that DFAT cells differentiate into peripheral nerve cells [62].
DFAT cells is one of the treatment technique used as a replacement for autologous nerve transplantation for treating facial nerve, whereas Matsumine et al. reported that artificial nerve regeneration made from silicone tubes filled with DFAT cells and type I collagen promote facial nerve regeneration in a rat model and DFAT cells differentiate into Schwann cells [63]. In addition, in 2020, Fujimaki H et al. revealed facial nerve regenerative capacity of collagen-coated PGA conduits with DFAT cells in a 7-mm facial nerve defect in rat model histological and physiological and this could be caused by (i) the release of growth factors from DFAT cells and (ii) the pluripotency of DFAT cells [64].
Human exfoliated deciduous teeth (SHED)
Dental pulp tends to be an alternative and less invasive type of stem cells when compared to BMSC. However, dental pulp progenitor cells are MSCs and dedifferentiate into Schwann cells and nerve cells, while can be used for the repair of injured nerves [65].
Stem cells from SHED and the dental pulp stem cells (DPSCs) merit a population of multipotent, self-renewing MSCs that effectively secrete a wide range of growth factors such as fibroblast growth factor (FGF), transforming growth factor-beta (TGF-b), connective tissue growth factor (CTGF), NGF, bone morphogenetic protein (BMP), and immunomodulatory factors. The main benefit of using SHED is that they do have a higher rate of proliferation than DPSC and were enriched with ECM. They can also be easily collected from deciduous teeth, which are regularly removed in infancy and usually discarded without any ethical concerns [66]. SHED has self-renewing capabilities, most of which express markers of neural progenitors (Doublecortin, GFAP, and Nestin), immature neural cells (bIII-tubulin, A2B5, and CNPase), oligodendrocytes, and bone marrow stromal stem cells (CD90, CD73, and CD105), but not markers of mature oligodendrocytes (MPB and APC) [67]. SHED that originates from cranial neural crest cells have been shown to differentiate in vitro in Schwann-like cells, as well as under chemically specified culture conditions are capable of rapidly proliferating into various cell lines such as cartilage, muscle bone, and neural cells. Moreover, differentiating SHEDs represent a mixture of glial cells and neuronal, as well an upregulation of tyrosine hydroxylase and the dopamine receptor 2 and transcription factor NR4A2 (also known as Nurr1) genes, where these findings suggest in the differentiating SHED cultures the presence of sympathetic and (or) dopaminergic subpopulations [68].
As well, human immature dental pulp stem cells (iDPSC) at the lesion site may act as a paracrine communication triggered by secreted trophic factors and cytokines. Consequently, these factors facilitate the migration, proliferation, and activation of Schwann cells, and stimulate endogenous repair of neurologically damaged area, thereby contributing to neuronal regeneration, proliferation, and regulating Schwann cells apoptosis leading to functional recovery [69,70].
In the study of Pereira LV, the use of stem cells from SHED associated with polyglycolic acidtube (PGAt) promotes higher regeneration of the mandibular branch of the facial nerve in rats 6 weeks after transplantation compared with the autograft group. The pattern of cell marker expression is similar to that seen in Schwann-like cells, indicating in vivo differentiation of SHED [71].
Based on a recently published report, a single use of iDPSC immediately after facial nerve crush injury in rats leads to facial nerve regeneration through a favorable microenvironment for neural cell survival and migration of endogenous cells to the injured site and promotes a beneficial local effect on neuroprotection, remyelination within 2 weeks of treatment [72].
Finally, dental pulp appears to be a more accessible and alternative source of stem cells, whereas dental pulp progenitor cells are closely related to MSC.
Scaffold Used For Facial Nerve Reconstruction
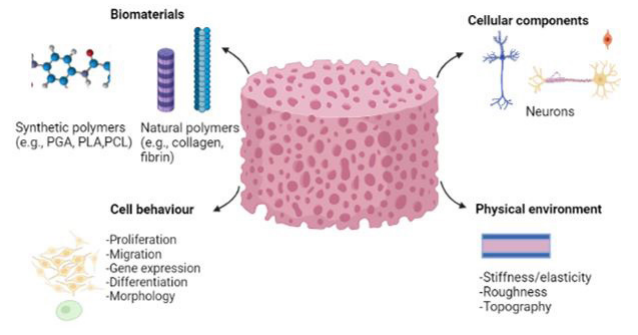
Ideally, scaffolds engineered for facial nerve repair can mimic the main physicochemical properties of the native ECM of the target tissue. The physical features of the scaffold, such as topography, roughness, and mechanical properties (e.g. stiffness and elasticity) affect cell morphology and behaviour, with effects on migration, proliferation, gene expression, and differentiation [73].
General scaffold design criteria are: (i) biocompatibility without inducing adverse immune reactions, and biodegradability with a regulated degradation rate to deal with cell/tissue ingrowth and maturation; (ii) a three-dimensional, highly porous structure with an integrated pore network for cell growth and the flow transfer of nutrients and metabolic waste; (iii) surface properties designed for the attachment, movement, proliferation, and differentiation of cell types of interest; (iv) mechanical properties that fit those of the tissue injected into, (v) simple and effective reproducibility of the scaffold structure in various shapes and sizes; (vi) easy preparatory procedures with the capacity to be sterilized. However, scaffold porosity is an important characteristic of most scaffolds, as it facilitates cell seeding and cell-matrix interaction and contributes to improve neovascularization. Moreover, the exact pore size depends on the application, the average pore diameter of 20-125 μm is appropriate for skin tissue and >300 μm for bone tissue, thus higher porosity lead to increased neovascularisation, while small pores favor hypoxic conditions [74, 75].
Various materials for nerve repair have been studied to prepare nerve conduits of either natural or synthetic products. Biological conduits themselves improve axonal regeneration as they increase the involvement of Schwann cells and contain ECM; but, to reduce the chance of rejection, they must be decellularized [76].
On the other hand, synthetic conduits have gained attention because they are biocompatible, biodegradable, and have nonimmunogenic structures that do not develop scars or fibrosis. Therefore, they are also preferred because they do not induce morbidity of the donor site and are easy to obtain. In addition, conduits provide a scaffold for stem cells because of their 3D structure, besides creating a tubular structure for axon regeneration [46, 77] (Figure 4-5).
Natural polymer
Natural polymers exhibit excellent bioactivity due to their components of ECM, and have been used to create natural hydrogels as scaffolds for tissue engineering due to their biocompatibility, intrinsic biodegradability, and essential biological functions. There are four primary types of natural polymers, which include [78]:
Proteins such as: collagen, gelatin, fibrin, silk, lysozyme, Matrigel™, and genetically engineered proteins, such as elastinlike polypeptides, calmodulin (a calcium-binding protein), and leucine zipper; Polysaccharides such as: HA, chitosan, agarose, and dextran; Protein/polysaccharide hybrid polymers such as: collagen/HA, gelatin/chitosan, fibrin/alginate, and laminin/ cellulose;
Biological polymers have high biocompatibility and degradability, offering relatively little control over their physical properties and are necessary for physiological attachment and axonal growth promotion. Collagens are the most widely used scaffold material because of their biocompatibility, abundance in the ECM, high tensile strength, promotes cellular proliferation and tissue healing, and establish importance in the regulation of Schwann cells [79, 80].
The united states Food and Drug Administration (FDA) approved Several bioresorbable nerve guidance conduits (NGCs) for human uses are: type 1 collagen (NeuraGen, NeuroMatrix, and NeuroFlex), and have shown potential to enhance facial nerve repair in preclinical trials, porcine small intestinal submucosa (Surgis Nerve Cuff), PGA(Neurotube) and poly(D,L-lactide-co-ε -caprolactone) (Neurolac). However, they are not recommended for gaps greater than 3 cm 81 and their biological output is poorer than the autograft, which remains the gold standard therapy for bridging approaches [79-83].
Collagen
Collagen is the main component of natural ECM and a natural polymer to fabricate natural hydrogels and is the most abundant protein in mammals. Collagen can be naturally degraded by metallomatrix proteinases (MMPs) – specifically, collagenase – Allowing local cell-controlled degradation in the engineered tissue [84].
In the study of Kitahara AK et al. facial nerve regeneration was achieved by the interposition of a collagen nerve guide in a 5 mm nerve gap in adult cats, giving great promise for the collagen nerve guide as a nerve conduit, and this outstanding performance can be hypothesized to lead to a similar placement in a 10–20 mm gap in humans [85]. In the study of Cao J et al, a collagen conduits filled with linear-ordered collagen (LOC) fibers enhanced with laminin and neurotrophic factors provided a compatible guide of rat axonal regeneration and functional recovery in a 5 mm sciatic nerve gap [86] and a 4 mm facial nerve gap 87 in a rat model. Another study in minipigs models, revealed that collagen nerve guide with collagen-binding domain (CBD)-CNTF or CBDbFGF promote repair 35 mm facial nerve injury [88].
In addition, Lu C et al. used a collagen scaffolds combined with CNTF in a 10 mm long gap in the buccal branch of minipigs facial nerve and showed promising effects on facial nerve regeneration. Consequently, oriented Schwann cell migration was facilitated by collagen scaffolds, while CBD-CNTF promotes axon sprout and myelin formation [89].
Ma F et al. used NSCs supplemented with bFGF a fibroblast growth factor on collagen scaffold in 8 mm facial nerve defects in rats and natural nerve conduit significantly promoted neural proliferation and functional recovery which was similar to those of the gold standard, an autograft [90]. Another study of Ma F et al. showed that collagen nerve conduits that were formed by immobilizing GDNF significantly enhanced facial nerve regenerationin 8 mm facial nerve defects in rat model, yielding results close to those of autograft. Collagen was collected from rat tails to create conduits and binding of GDNF in the collagen conduits prevented its rapid dispersion into the external fluid [91].
In the study of Wang et al. the use of collagen conduit with CBD-bFGF to repair facial nerve injury model in a rabbit model can enhance neural regeneration and obtain better nerve repair compared with the control group following injury, thus neurotrophic factors play important roles in nerve regeneration [3]. Consequently, the results confirmed those of previous studies using collagen conduit combined with modified CBD-CNTF, CBD-BDNF, and CBD-bFGF in a rat and mini-pig facial nerve model had a better effect on nerve restoration and functional recovery than with conduit that lacked CBD and neurotrophic factor [87,88].
Furthermore, the conduits serve as a physical bridge over a damaged region of tissue; however, a collagen conduit alone or empty conduits were inadequate for promoting nerve regeneration after nerve injury [92].
To be noted, GDNF can enhance the survival of both sensory and motor nerves and has major potential for the treatment of nerve injuries [93].
Gelatin
Gelatin is a denatured collagen a biodegradable polymer, created by splitting the natural triple-helix structure of collagen into single-strand molecules by hydrolysis. Gelatin is less immunogenic compared to its precursor and is likely to maintain informational signals such as the Arg–Gly–Asp (RGD) sequence, promoting cell adhesion, differentiation, migration, and proliferation [94].
Since the implanted stem cells affect their environment through the secretion of different factors, the fate of the cells is also determined by the same microenvironment. Thus, if the cells are not protected, their effects are either suppressed or the cells die before any beneficial function is induced. To prevent immediate rejection of transplanted cells by the host, it is important to inject them into gelatin mixture hydrogel [95]. It has also been shown that gelatin hydrogel act as a scaffold for MSCs, allowing their homogeneous growth [96]. Moreover, hydrogel containing bFGF has been used to treat facial nerve paralysis without any aberrant side-effects [97]. In the study of Matsumine H et al. a silicone tube filled with bFGF containing acidic gelatin hydrogel was transplanted into a 7 mm gap created in the buccal branch of the facial nerve in a rat model, whereas, the rate of nerve regeneration and the degree of nerve axon maturation was significantly increased after bFGF released from gelatin hydrogel microspheres during the first 2 weeks of nerve regeneration after peripheral nerve injury. Consequently, the regeneration of Schwann cells was promoted with the use of the sustained bFGFrelease method [98].
In this study, Esaki S. et al. evaluated in vivo the use of OSCs transplantation with biodegradable gelatin hydrogel for the treatment of facial nerve palsy (injury) in a mouse model, and the result showed more prominent and continued recovery of the facial nerve palsy compared to OSCs without biodegradable hydrogel where the recovery was limited to 1 week after facial nerve injury in the mouse model. Consequently, OSCs with biodegradable hydrogel improves the effect of transplanted cells by protecting them from the local environment and prolonging survival [99].
Fibrin
Fibrin gel is a degradable biopolymer formed from fibrinogen. Fibrin gel mimics the last step of the blood coagulation pathway which ends in a clot of fibrin [100].
In comparison to the synthetic polymeric materials, fibrin gel presents many advantages, such as excellent biocompatibility, nontoxic degradation products, and controllable degradation rate which matches those of tissue regeneration [101].
It has been shown in a study by Bayir O et al. that fetal brain tissue-derived mesenchymal stem cell (FBTMSC) combined fibrin glue offered the most effective microenvironment for nerve regeneration and could play a promising role as an adjunctive regenerative therapy in facial nerve crash injury [102].
Silk
Silk fibroin (SF) materials may facilitate the release of nerve growth factor particles and have more nutritional factors, and a more suitable microenvironment to promote nerve repair [103]. Hu A et al. showed that SF nanofibers as nerve conduits induce the facial nerve regeneration in a rat model after facial nerve injury with results comparable to those achieved with nerve autograft, and is widely considered as the ‘‘gold standard" for nerve with long-gap defects [104].
Chitin
Chitin is an abundant polysaccharide, derived from shellfish, that is biocompatible, biodegradable, and nontoxic, and they are easily processed into scaold [105]. It has been shown that chitin containing NGF induces facial nerve regeneration in a 8 mm facial nerve gap in rabbits model [106].
Chitosan
Chitosan is a deacetylated chitin, which interacts with ECM molecules, but is brittle in dry form, thus has to be chemically cross-linked [91]. Chao X et al. tested the effects of using autologous veins, which are rich in ECM, combined with NGF and the chitosan/glycerophosphate (C/GP) hydrogel on injured facial nerves in a rat model. Results showed an improvement in the facial nerve regeneration, whereas, C/GPNGF hydrogel acted as a scaffold in the vein conduit and continuously release NGF [107].
Hyaluronic acid (HA)
Is a linear polysaccharide, biocompatible, biodegradable, noncytotoxic, and anti-scarring aid, that possesses a nonsulfated glycosaminoglycan (GAG) structure and is commonly distributed throughout the ECM of all connective tissues [108]. As we mentioned above, Zhang H et al. revealed facial nerve regeneration in a 5 mm gap defect after implantation of neural stem embedded in hyaluronic acid, collagen composite scaffold and NT-3 in a rabbit model [46]
Synthetic polymers
The main motive of an artificial nerve conduit is to fill the nerve gap, by connecting the proximal and distal stumps of the injured nerve. Biodegradable polymers such as polylactic acid (PLA), PGA, polylactic-co-glycolic acid (PLGA), and polycaprolactone (PCL), allow nerve regeneration, showing comparable results to autografts [109].
Artificial synthetic biomaterials have good biocompatibility and biodegradability, as well, better control over their physical and chemical properties, such as nerve conduit rigidity, regulated rate of deterioration, and the presence of micropatterns and porosity. However, hardness and elasticity are poor of such materials [79, 82]. Polyester is the common synthetic material used in nervous tissue engineering which includes; PGA, PLA, and PCL [110].
Polyglycolic acid (PGA)
PGA is a synthetic biomaterial that has been active in improving facial nerve repair despite its rapid degradation. Navissano et al. showed 71% positive clinical results when using FDA-approved nerve conduit PGA-based, Neurotube, to improve facial nerve regeneration in seven patients with nerve gaps less than 3 cm [111]. As well, Ichihara S et al. revealed that PGA has good mechanical properties for the repair of a long nerve defect [112].
Wang et al. demonstrated in two weeks an increased expression of neuronal cytoskeleton molecules (GAP43, light chain neurofilament) and growth factors (NGF and BNDF) in nerves that had received BMSc in the PGAt/chitosan conduits [113]. Furthermore, Costa et al. showed a significant improvement of the facial nerve regeneration in six weeks after the introduction of the mesenchymal BMSC within PGAt in rats and has a more satisfying functional and morphological outcome for the injured facial nerve than the same surgical procedure without cell implant [114]. However, a study showed facial nerve regeneration in 10 mm defect after using PGA–collagen conduit in a rat model [115].
Polylactic acid (PLA)
PLA is a biocompatible aliphatic polyester, biodegradable, and slowly degraded by hydrolysis due to hydrophobic methyl group [116]. PLA conduit showed strong rat facial nerve regeneration in a 7 mm defect comparable to autograft [117].
Poly Lactic-co-Glycolic Acid (PLGA)
PLGA is a copolymer of PGA and PLA where is degraded by hydrolysis. However, a 50:50 combinations of PGA and PLA degrades faster than either PGA or PLA alone, and no secondary removal operation was required [118].
In the study of Sasaki R et al. PLGA tubes artificial nerve conduits filled with DPSCs are effective and promote facial nerve remyelination and regeneration in 7 mm rat facial nerve gaps without the need for a secondary removal operation [119]. Whereas, Kaka et al. combined bone marrow mesenchymal stem cells with a PLGA nanofiber scaffold, and transected sciatic nerve regeneration was improved, since stem cells release neurotrophic factors and thereby regulate the microenvironment [120].
Polycaprolactone (PCL)
PCL is aliphatic polyester, highly biocompatible, and it is slowly degraded by hydrolysis [121]. Jang CH et al. used PCLbased nerve conduit and collagen supplemented with human umbilical cord serum (hUCS) and showed strong facial nerve regeneration after 4 mm gap defect in rat model. Thus, growth factors in hUCS promoted neural regeneration and angiogenesis [122]. According to Shin et al. PCL material has a similar effect in repairing nerve to that of autografts and its performance was higher than PLA conduit [123]. When PCL nanofiber scaffolds combined with interleukin-β10, alternatively activated (M2) macrophages around the injured peripheral nerve which are important to its repair was promoted [124].
Polytetrafluoroethylene (PTFE)
PTFE is a fluorocarbon solid, inert, porous, has low adhesion and low inflammation with poor tissue attachment [125]. However, expanded polytetrafluoroethylene (e-PTFE) and collagen tubes as conduits may be effective in the repair of facial nerve defects in a rabbit model [126]. Undifferentiated stem cells can protect the distal nerve stump and improve the initial regeneration process by releasing neurotrophic factors, such as BDNF, and anti-inflammatory cytokines [127]. However, Ghoreishian et al., used an e-PTFE tube filled with undifferentiated ADSCs in a facial nerve gap size of 7 mm, and significantly greater facial nerve conduction velocity and action potential amplitude were observed compared with controls without stem cells in dogs [128]. Consequently, various materials have been used in tissue engineering for facial nerve regeneration (Table1).
Novel Technique for Facial Nerve Regeneration
The use of nanoparticles and lentiviruses as vectors for strengthening nerve guidance conduits for facial nerve repair is a possibility. Their properties allow continuous drug release with controlled parameters of concentration and time, resulting in greater synergistic regeneration of axons [129].
Lentiviral transduction of stem cells expressing neurotrophic factors is a novel strategy for precisely transferring desired neurotrophic factors within a virus. Because of the long-term increase in neurotrophic factor levels, this technique has an important benefit for long-term damage to a facial nerve. As a result, lentiviral transduction with a nerve guidance conduit has enormous potential as a therapeutic technique for clinical treatments of facial nerve degeneration [130].
On the other hand, the future of facial nerve regeneration will most likely include the combination of novel tissue-engineered techniques with bionics that emphasizes bioelectrical interfaces. Electrical interfaces allow the recording and induction of electric signals, which are essential for axonal signaling. An optimal interface is stable and can receive electrical signals from the contralateral intact facial nerve and transmit them to the deinnervated facial muscle to elicit a symmetric response. This tackles the clinical problem of facial asymmetry while simultaneously shielding the muscles from atrophy [22].
Discussion
Injuries to the facial nerve cause esthetic, functional, and psychological problems for the patient. Functional recovery is often slow, particularly after a complete transaction, despite advances in the medical and surgical management of facial nerve injuries. However, Facial nerve functional regeneration normally necessitates new axons outgrowth, myelination, and their correct reinnervation of the target organ. Tissue-engineered artificial nerve consists of scaffold material, ECM, seed cells, and factors to induce and promote growth [45].
Furthermore, stem cells are specialized cells that can be derived from a variety of sources, as they have the ability to shape the whole body, divide into several distinct cell forms during the course of the organism's life, and reproduce and proliferate. Clinical stem cell research has recently expanded with developments in regenerative medicine [31].
Scaffolds are designed to provide ideal conditions for neuronal guidance and regeneration. These methods imitate the normal architecture of an autograft. These grafts can ideally be impregnated with several neurotrophins, signaling molecules, glial cells, NSCs, and ECM structural proteins [131]. Sufficient scaold permeability allows for the steady diffusion of oxygen, nutrients, and growth factors, all of which are essential for nerve regeneration. Progressive scaffold degradation reduces nerve inflammation, nerve compression, and eliminates the need for a second operation to remove the implant. Degradation can occur after enough time for axonal reinnervation and result in quickly excreted, non-toxic materials [132].
BMSCs have been widely used for facial nerve regeneration that in cultured can differentiate into Schwann-like cells [41]. A study reports the successful use of autologous bone marrow mononuclear stem cells from the blood aspirated from iliac crest in eight patients with post-traumatic facial nerve paralysis [42]. Compared with BMSCs, ADSCs are more plentiful and easier to harvest, and a growing number of studies are looking into the prospect of using ADSCs instead of BMSCs for stem cell transplantation [133]. In a rat model, authors showed that ADSCs gives approximately three daughter axons between the facial nerve and the nerve graft with facial paralysis and optimized myelination [55]. In fact, DFAT is more homogenous than ADSC, but have similar immune-phenotypes; however, several studies showed that conduit tube filled with DFAT in a rat model promote facial nerve regeneration [62-64].
Dental pulp, as compared to BMSC, is a less invasive and an alternative form of stem cell, although SHED and DPSCs are a population of multipotent, self-renewing MSCs. Recently, several studies have shown that SHED and DPSCs can be successfully used for recovery of facial nerve damage through beneficial local effect on neuro-protection, remyelination and by providing a favorable microenvironment for neural cell survival and endogenous cell migration to the damaged site [71, 72].
NSCs embedded in a scaffold induce NSC differentiation and neurite outgrowth, also provided a growth factor to stimulate endogenous regeneration, thus NSC is a selectable seed cell in tissue engineering for facial nerve regeneration [46]. Whereas, OSCs are multipotent neural stem cells that can differentiate into cells from all germ layers and can be harvested from nasal biopsies. They are likely the only accessible stem cells with neurogenic properties for nerve regeneration and have shown an effective result in treating facial nerve injuries [48].
On the other side, various materials such as natural or synthetic (biodegradable and nondegradable) products can be used for repairing facial nerve injury. Biological conduits themselves increase axonal regeneration, while synthetic conduits have gained popularity since they are easy to obtain and do not induce morbidity of the donor site.
Natural polymers have been used as scaffolds for tissue engineering due to their biocompatibility, biodegradability, whereas collagens are the most widely used to repair facial nerve injury. The application of collagen with neurotrophic factors played more important roles for facial nerve regeneration, and the combination of CNTF-BDNF or CNTF-bFGF showed a significant regeneration of nerve fibers and nerve function when compared with using scaffolds alone. Thus, the advantage of collagen is being semipermeable, allowing nerve growth factors to diffuse into the tube [87, 88]. Moreover, several studies have shown that collagen scaffolds combined with CNTF or GDNF or bFGF in mini-pigs, rats, rabbits promotes axon sprout, myelin formation and improve nerve regeneration of the facial nerve when compared to the control group; thus, neurotrophic factors play important roles in nerve regeneration [3, 89, 91]. Furthermore, when collagen was supplemented with NSCs and bFGF in a rat model, regeneration of the facial nerve was observed to a degree similar to autologous nerve grafting [90].
Gelatin, which acts as a scaffold, is a denatured collagen a biodegradable polymer that has been used in several studies for facial nerve regeneration. However, applying bFGF impregnated gelatin in a 7 mm gap demonstrated regeneration of Schwann cells of the facial nerve, as well as, the number of regenerated nerve axons is induced, and a greater degree of nerve axon maturation in the bFGF group was observed compared to the bFGF-free group in a rat model [98]. Furthermore, OSCs were implanted into gelatin hydrogel, which aided to maintain the OSCs around the injury site and boosted their survival and function, allowing them to release the cytokines and various factors to mediate an improved and accelerated healing response after facial nerve injury [99].
Fibrin is a natural polymer that is highly biocompatible when combined with FBTMSC, provides a suitable microenvironment that may be a potential regenerative therapy for post-traumatic facial paralysis [102]. Additionally, Chitin tubes carrying NGF successfully produce an ideal condition for facial nerve regeneration in a rabbit model with an 8 mm gap [106].
Likewise, the biomedical applications of SF that are considered as bioscaffolds for tissue engineering in 10 mm long gap facial nerve defect in rats could promote facial nerve regeneration with axonal growth and formation of the myelin sheaths [104]. Also, Chitosan, a deacetylated chitin demonstrated functional and morphological healing of the injured facial nerve following delivery of C/GP-NGF hydrogel in a 5 mm gap in the buccal branch of a rat facial nerve [107]. Similarly, embedding NSCs to HA-collagen conduit promotes facial nerve regeneration in the rabbit model [46].
Additionally, Synthetic biomaterials offer good biocompatibility and biodegradability, as well as more control over their physical and chemical characteristics. When PGAt and BMSC were mixed in autografted rat facial nerve, regeneration of the facial nerve was enhanced, demonstrating the favorable benefits of BMSC in the surgical repair of peripheral nerve lesions [114]. However, PGA– collagen tubes may be used in facial nerve gap reconstruction, yet functional recovery was inferior in comparison to that obtained with an autograft. The lack of a cellular component, such as Schwann and endothelial cells, was assumed to be the cause of this difference [115]. As well, transplantation of a PLA nonwoven fabric tube into a 7 mm gap in the buccal branch of the facial nerve in rats resulted in nerve regeneration. According to histological testing, non-woven fabric produced superior results for facial nerve regeneration than silicon tube control [117].
Sasaki et al., used Silicone neuroconduit and DPSCs embedded in a three-dimensional collagen gel (2008), and they evaluated facial nerve regeneration in rats after configuring a 7 mm gap and tubulization with or without DPSCs by the degree of neural attachment, while PLGA neuroconduit was used in the second study (2011). In both cases, the regeneration of the DPSCs group was found to be faster and more effectively regenerate the nerve than in the control group. However, comparing the two types of conduits, silicone was not absorbable, and thus if not removed, local chronic inflammatory processes and pain are generated, whereas, PLGA neuroconduit is absorbable and gradually dissolves over time where revascularization begins with the improvement in the nutrient supply, thus removing the complications mentioned above, preventing the need for reoperation. Consequently, it is shown that DPSCs has a higher potential to be simpler with higher rates of cell proliferation and neurotrophic factors production in vitro and a greater potential for neural regeneration, likely because they are specifically derived from the neural crest [119, 134].
Natural polymers, on the other hand, have weak mechanical qualities, leading the conduit to degrade quickly in vivo; hence, PCL is a good biocompatible scaffold due to its slow rate of degradation. According to a study, PCL supplemented with collagen and hUCS provides more favorable microenvironmental conditions by facilitating facial regeneration in a nerve gap of 4 mm and exhibits more therapeutic potential for rat facial nerve regeneration than the autograft approach. Thus, compared to pure PCL and PCL/collagen fibrous conduits, PCLbased nerve conduits showed considerably greater bioactivities in vitro and in vivo, whereas growth factors in hUCS enhanced angiogenesis and neural regeneration [122]. Whereas, PTFE, a physiologically inert material that may be considered a good nerve conduit showed improved the functional outcomes of facial nerve regeneration in a gap size of 7 mm when undifferentiated ADSCs are added [128].
In summary, advances in tissue engineering have fueled the creation of numerous nerve conduits that are intended to act as autologous nerve graft alternatives. Various stem cells that have been filled in a scaffold whether natural or synthetic showed a great and promising result for facial nerve injuries as they promote and enhance regeneration of facial nerve, especially when they are combined with growth factors as they collaborate synergistically. Further research is required to determine the effective concentration and administration duration required in each material to induce facial nerve regeneration; hence, these results must be confirmed in a larger sample size in animal and human studies.
Conclusion
Not only is the facial nerve (cranial nerve VII) important for facial expression and communication, but it is also important for eye closing, oral competence, and hearing protection. The use of stem cells improved the clinical effects of tissue-engineered nerve grafts. Scaffolds are playing an increasingly important role in the treatment of facial nerve injuries, ultimately supplying both the structural elements and the microenvironment required to promote neurite development and reinnervation, which will continue to shape the future of facial nerve rehabilitation. Furthermore, growth factors have been found to enhance facial nerve regeneration. The study of tissue engineering for facial nerve injuries hold a promise for the successful treatment, because of their ability to differentiate into other types of cells and to improve axon function, as well, to enhance facial nerve regeneration. However, further research in human trials and large sample size are needed to search the appropriate seed cells/ scaffold/growth factor and to validate the therapeutic effects of tissue engineering for facial nerve injury; to determine the effective concentration and administration duration required in each material to induce facial nerve regeneration; and finally to evaluate the role of new cells formation in the long-term success.
References
- Ichihara S, Inada Y, Nakamura T (2008) Artificial nerve tubes and their application for repair of peripheral nerve injury: an update of current concepts. Injury.39 Suppl 4: 29-39.
- Flint PW, Cummings CW, eds. Cummings (2015) Otolaryngology: Head and Neck Surgery ; [Get Full Access and More at ExpertConsult.Com]. 6. ed. Elsevier, Saunders.
- Wang P, Zhao H, Yao Y, et al. (2020) Repair of facial nerve crush injury in rabbits using collagen plus basic fibroblast growth factor. J Biomed Mater Res. 108:1329-37.
- Kim J (2021) Neural Reanimation Advances and New Technologies. Facial Plast Surg Clin North Am. 2016;24(1):71-84. doi:10.1016/j.fsc.2015.09.006
- Volk GF, Pantel M, Guntinas-Lichius O (2010) Modern concepts in facial nerve reconstruction. Head Face Med. 2010;6(1):25. doi:10.1186/1746-160X-6-25
- Lavasani M, Gehrmann S, Gharaibeh B, et al. (2011) Venous Graft-Derived Cells Participate in Peripheral Nerve Regeneration. Chin W-C, ed. PLoS ONE. 2011;6(9):e24801. doi:10.1371/ journal.pone.0024801
- Rodrigues MCO, Rodrigues AA, Glover LE, Voltarelli J, Borlongan CV (2012) Peripheral Nerve Repair with Cultured Schwann Cells: Getting Closer to the Clinics. The Scientific World Journal 1-10.
- Welin D, Novikova LN, Wiberg M, Kellerth JO, Novikov LN (2008) Survival and regeneration of cutaneous and muscular afferent neurons after peripheral nerve injury in adult rats. Exp Brain Res 186: 315-23.
- Sterodimas A, De Faria J, Correa WE, Pitanguy I (2009) Tissue Engineering in Plastic Surgery: An Up-to-Date Review of the Current Literature. Annals of Plastic Surgery 62: 97-103.
- Ghasemi-Mobarakeh L, Prabhakaran MP, Morshed M, et al. (2011) Application of conductive polymers, scaffolds and electrical stimulation for nerve tissue engineering. J Tissue Eng Regen Med 5: e17-35.
- Skalak R, Fox CF (1988) eds. Tissue Engineering: Proceedings of a Workshop Held at Granlibakken, Lake Tahoe, California, February 26-9.
- Langer R, Vacanti J (1993) Tissue engineering. Science 260: 920-6.
- Muschler GF, Nakamoto C, Griffith LG (2004) ENGINEERING PRINCIPLES OF CLINICAL CELL-BASED TISSUE ENGINEERING: The Journal of Bone and Joint Surgery-American 86: 1541-58.
- Cho HH, Jang S, Lee SC, et al. (2010) Effect of neural-induced mesenchymal stem cells and platelet-rich plasma on facial nerve regeneration in an acute nerve injury model: MSCs and PRP Effects on Nerve Regeneration. The Laryngoscope 120: 907-13.
- Zavaglia CAC, Prado da Silva MH (2016) Feature Article: Biomaterials. In: Reference Module in Materials Science and Materials Engineering. Elsevier B9780128035818041000.
- Lee K, Silva EA, Mooney DJ (2011) Growth factor delivery-based tissue engineering: general approaches and a review of recent developments. J R Soc Interface 8: 153-70.
- Haastert K, Ying Z, Grothe C, Gómez-Pinilla F (2008) The effects of FGF-2 gene therapy combined with voluntary exercise on axonal regeneration across peripheral nerve gaps. Neuroscience Letters 443: 179-83.
- May M, Schaitkin BM (2000) The Facial Nerve. May’s 2. ed. Thieme.
- Kaya Y, Sarikcioglu L. Sir Herbert Seddon (1903–1977) and his classification scheme for peripheral nerve injury. Childs Nerv Syst 31: 177-80.
- Sunderland S (1951) A CLASSIFICATION OF PERIPHERAL NERVE INJURIES PRODUCING LOSS OF FUNCTION. Brain 74: 491-516.
- Mackinnon SE, Dellon AL (1988) Surgery of the Peripheral Nerve. Thieme Medical Publishers ; G. Thieme Verlag
- Langhals NB, Urbanchek MG, Ray A, Brenner MJ (2014) Update in facial nerve paralysis: tissue engineering and new technologies. Current Opinion in Otolaryngology & Head and Neck Surgery 22: 291-9.
- Hohman MH, Hadlock TA (2014) Etiology, diagnosis, and management of facial palsy: 2000 patients at a facial nerve center: Diagnosis and Management of Facial Palsy. The Laryngoscope 124: E283-93.
- Lee LN, Lyford-Pike S, Boahene KDO (2013) Traumatic Facial Nerve Injury. Otolaryngologic Clinics of North America 46: 825-39.
- Pan YA, Misgeld T, Lichtman JW, Sanes JR (2003) Effects of neurotoxic and neuroprotective agents on peripheral nerve regeneration assayed by time-lapse imaging in vivo. J Neurosci. 2003;23(36):11479-11488.
- Bhangra KS, Busuttil F, Phillips JB, Rahim AA (2016) Using Stem Cells to Grow Artificial Tissue for Peripheral Nerve Repair. Stem Cells International 1-18.
- Hall S (2001) Nerve Repair: A Neurobiologist’s View. Journal of Hand Surgery 26: 129-36.
- Nishiura Y, Brandt J, Nilsson A, Kanje M, Dahlin LB (2004) Addition of Cultured Schwann Cells to Tendon Autografts and Freeze–Thawed Muscle Grafts Improves Peripheral Nerve Regeneration. Tissue Engineering 10: 157-64.
- Gu X, Ding F, Williams DF (2014) Neural tissue engineering options for peripheral nerve regeneration. Biomaterials 35: 6143-56.
- Kingham PJ, Kalbermatten DF, Mahay D, Armstrong SJ, Wiberg M, et al. (2007) Adipose-derived stem cells differentiate into a Schwann cell phenotype and promote neurite outgrowth in vitro. Experimental Neurology 207: 267-74.
- Wang TV, Delaney S, Pepper JP (2016) Current state of stem cell-mediated therapies for facial nerve injury: Current Opinion in Otolaryngology & Head and Neck Surgery 24: 285-93.
- Vakharia KT, Lindsay RW, Knox C, et al. (2011) The Effects of Potential Neuroprotective Agents on Rat Facial Function Recovery Following Facial Nerve Injury. Otolaryngol Head Neck Surg 144: 53-9.
- Marion NW, Mao JJ (2006) Mesenchymal Stem Cells and Tissue Engineering. In: Methods in Enzymology. 420: 339-61.
- Majo F, Rochat A, Nicolas M, Jaoudé GA, Barrandon Y (2008) Oligopotent stem cells are distributed throughout the mammalian ocular surface. Nature 456: 250-4.
- Ousset M, Van Keymeulen A, Bouvencourt G, et al. (2012) Multipotent and unipotent progenitors contribute to prostate postnatal development. Nat Cell Biol 14: 1131-8.
- Alessandri M, Lizzo G, Gualandi C, et al. (2014) Influence of biological matrix and artificial electrospun scaffolds on proliferation, differentiation and trophic factor synthesis of rat embryonic stem cells. Matrix Biology 33: 68-76.
- Chambers SM, Fasano CA, Papapetrou EP, Tomishima M, Sadelain M, et al. (2009) Highly efficient neural conversion of human ES and iPS cells by dual inhibition of SMAD signaling. Nat Biotechnol 27: 275-80.
- Wang A, Tang Z, Park IH, et al. (2011) Induced pluripotent stem cells for neural tissue engineering. Biomaterials 32: 5023-32.
- Wang X, Luo E, Li Y, Hu J (2011) Schwann-like mesenchymal stem cells within vein graft facilitate facial nerve regeneration and remyelination. Brain Research 1383: 71-80.
- Yi S, Zhang Y, Gu X, et al. (2020) Application of stem cells in peripheral nerve regeneration. Burns Trauma 8: tkaa002.
- Chen CJ, Ou YC, Liao SL, et al. (2007) Transplantation of bone marrow stromal cells for peripheral nerve repair. Experimental Neurology 204: 443-53.
- Aggarwal S, Gupta A, Modi M, Gupta R, Marwaha N (2012) Safety Profile of Bone Marrow Mononuclear Stem Cells in the Rehabilitation of Patients with Posttraumatic Facial Nerve Paralysis—A Novel Modality (Phase One Trial). J Neurol Surg B 73: 245-52.
- Wu L, Han D, Jiang J, et al. (2020) Co-transplantation of bone marrow mesenchymal stem cells and monocytes in the brain stem to repair the facial nerve axotomy. Eur J Histochem. Published online June 19, 2020.
- Gage FH (2000) Mammalian Neural Stem Cells. Science 287: 1433-8.
- Guo BF, Dong MM (2009) Application of neural stem cells in tissue-engineered artificial nerve. Otolaryngol Head Neck Surg 140: 159-64
- Zhang H, Wei Y, Tsang K, et al. (2008) Implantation of neural stem cells embedded in hyaluronic acid and collagen composite conduit promotes regeneration in a rabbit facial nerve injury model. J Transl Med 6: 67.
- Mackay-Sim A (2010) Stem cells and their niche in the adult olfactory mucosa. Arch Ital Biol 148: 47-58.
- Batioglu-Karaaltin A, Karaaltin MV, Oztel ON, et al. (2016) Human olfactory stem cells for injured facial nerve reconstruction in a rat model: Olfactory stem cells for injured facial nerve reconstruction. Head Neck 38: E2011-20.
- Gomillion CT, Burg KJL (2006) Stem cells and adipose tissue engineering. Biomaterials 27: 6052-63.
- di Summa PG, Kingham PJ, Raffoul W, Wiberg M, Terenghi G, et al. (2010) Adipose-derived stem cells enhance peripheral nerve regeneration. Journal of Plastic, Reconstructive & Aesthetic Surgery 63: 1544-52.
- Erba P, Mantovani C, Kalbermatten DF, Pierer G, Terenghi G, et al. (2010) Regeneration potential and survival of transplanted undifferentiated adipose tissue-derived stem cells in peripheral nerve conduits. J Plast Reconstr Aesthet Surg 63: e811-7.
- Liu Y, Zhang Z, Qin Y, et al. (2013) A new method for Schwann-like cell differentiation of adipose derived stem cells. Neuroscience Letters 551: 79-83.
- Kingham PJ, Reid AJ, Wiberg M (2015) Adipose-Derived Stem Cells for Nerve Repair: Hype or Reality? Cells Tissues Organs 200: 23-30.
- Kamei W, Matsumine H, Osaki H, et al. (2018) Axonal supercharged interpositional jump-graft with a hybrid artificial nerve conduit containing adipose-derived stem cells in facial nerve paresis rat model. Microsurgery 38: 889-98.
- Abbas OL, Borman H, Uysal ÇA, et al (2016) Adipose-Derived Stem Cells Enhance Axonal Regeneration through Cross-Facial Nerve Grafting in a Rat Model of Facial Paralysis: Plastic and Reconstructive Surgery 138: 387-96.
- Tan J, Xu Y, Han F, Ye X (2019) Genetical modification on adipose-derived stem cells facilitates facial nerve regeneration.Aging 11: 908-20.
- Matsumine H, Numakura K, Climov M, Watanabe Y, Giatsidis G, et al. (2017) Facial-nerve regeneration ability of a hybrid artificial nerve conduit containing uncultured adipose-derived stromal vascular fraction: An experimental study: Facial Nerve Regeneration Using SVF in Rats. Microsurgery 37: 808-18.
- Watanabe Y, Sasaki R, Matsumine H, Yamato M, Okano T (2017) Undifferentiated and differentiated adipose-derived stem cells improve nerve regeneration in a rat model of facial nerve defect: Improvement of facial nerve regeneration by transplantation of adipose-derived stem cell. J Tissue Eng Regen Med 11: 362-74.
- Yagi K, Kondo D, Okazaki Y, Kano K (2004) A novel preadipocyte cell line established from mouse adult mature adipocytes. Biochemical and Biophysical Research Communications 321: 967-74.
- Matsumoto T, Kano K, Kondo D, et al. (2008) Mature adipocyte-derived dedifferentiated fat cells exhibit multilineage potential. J Cell Physiol 215: 210-22.
- Kishimoto N, Honda Y, Momota Y, Tran S (2018) Dedifferentiated Fat (DFAT) cells: A cell source for oral and maxillofacial tissue engineering. Oral Dis 24: 1161-7.
- Kono S, Kazama T, Kano K, Harada K, Uechi M, et al. (2014) Phenotypic and functional properties of feline dedifferentiated fat cells and adipose-derived stem cells. The Veterinary Journal 199: 88-96.
- Matsumine H, Takeuchi Y, Sasaki R, et al. (2014) Adipocyte-Derived and Dedifferentiated Fat Cells Promoting Facial Nerve Regeneration in a Rat Model: Plastic and Reconstructive Surgery 134: 686-97.
- Fujimaki H, Matsumine H, Osaki H, et al. (2020) Corrigendum to “Dedifferentiated fat cells in polyglycolic acid-collagen nerve conduits promote rat facial nerve regeneration” [Regen Ther 11 (2019) 240–248]. Regenerative Therapy 15: 35-43.
- Tobita M, Mizuno H (2013) Adipose-Derived Stem Cells and Periodontal Tissue Engineering. Int J Oral Maxillofac Implant 28: e487-93.
- Nakamura S, Yamada Y, Katagiri W, Sugito T, Ito K, et al. (2009) Stem Cell Proliferation Pathways Comparison between Human Exfoliated Deciduous Teeth and Dental Pulp Stem Cells by Gene Expression Profile from Promising Dental Pulp. Journal of Endodontics 35: 1536-42.
- Didilescu AC, Rusu MC, Nini G. (2013) Dental pulp as a stem cell reservoir. Rom J Morphol Embryol. 54: 473-8.
- Jarmalavičiūtė A, Tunaitis V, Strainienė E, et al. (2013) A New Experimental Model for Neuronal and Glial Differentiation Using Stem Cells Derived from Human Exfoliated Deciduous Teeth. J Mol Neurosci. 51: 307-17.
- Hui L, Yuan J, Ren Z, Jiang X (2015) Nerve growth factor reduces apoptotic cell death in rat facial motor neurons after facial nerve injury. Neurosciences (Riyadh) 20: 65-8.
- Yamamoto T, Osako Y, Ito M, et al. (2016) Trophic Effects of Dental Pulp Stem Cells on Schwann Cells in Peripheral Nerve Regeneration. Cell Transplant 25: 183-93.
- Pereira LV, Bento RF, Cruz DB, et al. (2019) Stem Cells from Human Exfoliated Deciduous Teeth (SHED) Differentiate in vivo and Promote Facial Nerve Regeneration. Cell Transplant 28: 55-64.
- Saez DM, Sasaki RT, Martins D de O, Chacur M, Kerkis I, et al. (2019) Rat Facial Nerve Regeneration with Human Immature Dental Pulp Stem Cells. Cell Transplant 28: 1573-84.
- Ross AM, Jiang Z, Bastmeyer M, Lahann J (2012) Physical Aspects of Cell Culture Substrates: Topography, Roughness, and Elasticity. Small 8: 336-55.
- Henkel J, Hutmacher DW (2013) Design and fabrication of scaffold-based tissue engineering. BioNanoMaterials 14(3-4).
- Yannas IV (2013) Emerging rules for inducing organ regeneration. Biomaterials 34: 321-30.
- Sun F, Zhou K, Mi W, Qiu J (2011) Combined use of decellularized allogeneic artery conduits with autologous transdifferentiated adipose-derived stem cells for facial nerve regeneration in rats. Biomaterials. 32: 8118-28.
- Brännvall K, Bergman K, Wallenquist U, et al. (2007) Enhanced neuronal differentiation in a three-dimensional collagen-hyaluronan matrix. J Neurosci Res 85: 2138-46.
- Zhu J, Marchant RE (2011) Design properties of hydrogel tissue-engineering scaffolds. Expert Review of Medical Devices 8: 607-26.
- Hasirci V, Arslantunali D, Dursun T, Yucel D, Hasirci N (2014) Peripheral nerve conduits: technology update. MDER 405.
- Koopmans G, Hasse B, Sinis N (2009) The Role of Collagen in Peripheral Nerve Repair. In: International Review of Neurobiology 87: 363-79.
- Kehoe S, Zhang XF, Boyd D (2012) FDA approved guidance conduits and wraps for peripheral nerve injury: A review of materials and efficacy. Injury 43: 553-72.
- Nectow AR, Marra KG, Kaplan DL (2012) Biomaterials for the Development of Peripheral Nerve Guidance Conduits. Tissue Engineering Part B: Reviews 18: 40-50.
- Tan A, Rajadas J, Seifalian AM (2012) Biochemical engineering nerve conduits using peptide amphiphiles. Journal of Controlled Release 163: 342-52.
- Tan H, Marra KG (2010) Injectable, Biodegradable Hydrogels for Tissue Engineering Applications. Materials 3: 1746-67.
- Kitahara AK, Nishimura Y, Shimizu Y, Endo K (2009) Facial nerve repair accomplished by the interposition of a collagen nerve guide. Journal of Neurosurgery 93: 113-20.
- Cao J, Sun C, Zhao H, et al. (2011) The use of laminin modified linear ordered collagen scaffolds loaded with laminin-binding ciliary neurotrophic factor for sciatic nerve regeneration in rats. Biomaterials 32: 3939-48.
- Cao J, Xiao Z, Jin W, et al. (2013) Induction of rat facial nerve regeneration by functional collagen scaffolds. Biomaterials 34: 1302-10.
- Cui Y, Lu C, Meng D, et al. (2014) Collagen scaffolds modified with CNTF and bFGF promote facial nerve regeneration in minipigs. Biomaterials 35: 7819-27
- Lu C, Meng D, Cao J, et al. (2015) Collagen scaffolds combined with collagen‐binding ciliary neurotrophic factor facilitate facial nerve repair in mini‐pigs. J Biomed Mater Res 103: 1669-76.
- Ma F, Zhu T, Xu F, et al. (2017) Neural stem/progenitor cells on collagen with anchored basic fibroblast growth factor as potential natural nerve conduits for facial nerve regeneration. Acta Biomaterialia 50: 188-97.
- Ma F, Xu F, Li R, et al. (2018) Sustained delivery of glial cellderived neurotrophic factors in collagen conduits for facial nerve regeneration. Acta Biomaterialia. 69: 146-55.
- Ribeiro-Resende VT, Koenig B, Nichterwitz S, Oberhoffner S, Schlosshauer B (2009) Strategies for inducing the formation of bands of Büngner in peripheral nerve regeneration. Biomaterials 30: 5251-9.
- Shakhbazau A, Mohanty C, Shcharbin D, et al. (2013) Doxycycline-regulated GDNF expression promotes axonal regeneration and functional recovery in transected peripheral nerve. Journal of Controlled Release 172: 841-851.
- Sakai S, Hirose K, Taguchi K, Ogushi Y, Kawakami K (2009) An injectable, in situ enzymatically gellable, gelatin derivative for drug delivery and tissue engineering. Biomaterials. 30: 3371-7.
- Kelly S, Bliss TM, Shah AK, et al. (2004) Transplanted human fetal neural stem cells survive, migrate, and differentiate in ischemic rat cerebral cortex. Proceedings of the National Academy of Sciences 101: 11839-44.
- Umehara K, Iimura T, Sakamoto K, et al. (2012) Canine Oral Mucosal Fibroblasts Differentiate into Osteoblastic Cells in Response to BMP-2. Anat Rec 295: 1327-35.
- Hato N, Nota J, Komobuchi H, et al. (2012) Facial Nerve Decompression Surgery Using bFGF-Impregnated Biodegradable Gelatin Hydrogel in Patients with Bell Palsy. Otolaryngol Head Neck Surg 146: 641-6.
- Matsumine H, Sasaki R, Tabata Y, et al. (2016) Facial nerve regeneration using basic fibroblast growth factor-impregnated gelatin microspheres in a rat model: Facial nerve regeneration with bFGF-impregnated gelatin in rats. J Tissue Eng Regen Med 10: E559-67.
- Esaki S, Katsumi S, Hamajima Y, Nakamura Y, Murakami S (2019) Transplantation of Olfactory Stem Cells with Biodegradable Hydrogel Accelerates Facial Nerve Regeneration After Crush Injury: OSCs with Hydrogel Accelerate Facial Nerve Regeneration. STEM CELLS Translational Medicine 8: 169-78
- Wolberg AS (2007) Thrombin generation and fibrin clot structure. Blood Reviews 21: 131-42.
- Sidelmann JJ, Gram J, Jespersen J, Kluft C (2000) Fibrin Clot Formation and Lysis: Basic Mechanisms. Semin Thromb Hemost 26: 605-18.
- Bayir Ö, KaragÖz T, Alpaslan Pinarli F, et al. (2020) IMPACT OF FETAL BRAIN TISSUE DERIVED MESENCHYMAL STEM CELL and FIBRIN GLUE ON FACIAL NERVE CRASH INJURY. Turk J Med Sci. Published online November 27, 2020.
- Han X, Liu H, Kuang X, Wang Z, Wang X (2018) Silk Fibroin Improves the Release of Nerve Growth Factor from Hydroxyapatite Particles Maintaining its Bioactivity. CDD 15: 879-86.
- Hu A, Zuo B, Zhang F, Zhang H, Lan Q (2013) Evaluation of electronspun silk fibroin-based transplants used for facial nerve repair. Otol Neurotol 34: 311-8.
- Yang TL (2011) Chitin-based Materials in Tissue Engineering: Applications in Soft Tissue and Epithelial Organ. IJMS 12: 1936-63.
- Zhang SL, Meng ZY, Ma J (2000) [Experimental studies on rabbit facial nerve regeneration in chitin tubes containing nerve growth factor]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 14: 340-2.
- Chao X, Xu L, Li J, et al. (2016) Facilitation of facial nerve regeneration using chitosan- β -glycerophosphate-nerve growth factor hydrogel. Acta Oto-Laryngologica 136: 585-91.
- Yasui G, Yamamoto Y, Shichinohe R, et al. (2016) Neuregulin-1 released by biodegradable gelatin hydrogels can accelerate facial nerve regeneration and functional recovery of traumatic facial nerve palsy. Journal of Plastic, Reconstructive & Aesthetic Surgery 69: 328-34.
- Daly WT, Yao L, Abu-rub MT, et al. (2012) The effect of intraluminal contact mediated guidance signals on axonal mismatch during peripheral nerve repair. Biomaterials 33: 6660- 71.
- Gonçalves C, Ribeiro J, Pereira T, et al. (2016) Preparation and characterization of electrical conductive PVA based materials for peripheral nerve tube-guides: Electrical Conductive PVA. J Biomed Mater Res 104: 1981-7.
- Navissano M, Malan F, Carnino R, Battiston B (2005) Neurotube® for facial nerve repair. Microsurgery 25: 268-71.
- Ichihara S, Facca S, Liverneaux P, et al. (2015) Mechanical properties of a bioabsorbable nerve guide tube for long nerve defects. Chirurgie de la Main 34: 186-92.
- Wang J, Ding F, Gu Y, Liu J, Gu X (2009) Bone marrow mesenchymal stem cells promote cell proliferation and neurotrophic function of Schwann cells in vitro and in vivo. Brain Research 1262: 7-15.
- Costa HJZR, Ferreira Bento R, Salomone R, et al. (2013) Mesenchymal bone marrow stem cells within polyglycolic acid tube observed in vivo after six weeks enhance facial nerve regeneration. Brain Research. 1510: 10-21.
- Oatari M, Uehara M, Shimizu F (2018) Evaluation of the effects of a polyglycolic acid–collagen tube in the regeneration of facial nerve defects in rats. Int J Artif Organs 41: 664-9.
- Goulart CO, Pereira Lopes FR, Monte ZO, et al. (2016) Evaluation of biodegradable polymer conduits – poly(l-lactic acid) – for guiding sciatic nerve regeneration in mice. Methods 99: 28-36.
- Matsumine H, Sasaki R, Yamato M, Okano T, Sakurai H (2014) A polylactic acid non-woven nerve conduit for facial nerve regeneration in rats: PLA non-woven nerve conduit for facial nerve regeneration. J Tissue Eng Regen Med 8: 454-62.
- Yi S, Xu L, Gu X (2019)Scaffolds for peripheral nerve repair and reconstruction. Experimental Neurology 319: 112761.
- Sasaki R, Aoki S, Yamato M, et al. (2011) PLGA artificial nerve conduits with dental pulp cells promote facial nerve regeneration. J Tissue Eng Regen Med 5: 823-30.
- Kaka G, Arum J, Sadraie SH, Emamgholi A, Mohammadi A (2017) Bone Marrow Stromal Cells Associated with Poly L-Lactic-Co-Glycolic Acid (PLGA) Nanofiber Scaff old Improve Transected Sciatic Nerve Regeneration. Iran J Biotechnol 15: 149-56.
- Barbarisi M, Marino G, Armenia E, et al. (2015) Use of polycaprolactone (PCL) as scaffolds for the regeneration of nerve tissue. J Biomed Mater Res 103: 1755-60.
- Jang CH, Lee H, Kim M, Kim G (2016) Effect of polycaprolactone/collagen/hUCS microfiber nerve conduit on facial nerve regeneration. International Journal of Biological Macromolecules 93: 1575-82.
- Shin RH, Friedrich PF, Crum BA, Bishop AT, Shin AY (2009) Treatment of a Segmental Nerve Defect in the Rat with Use of Bioabsorbable Synthetic Nerve Conduits: A Comparison of Commercially Available Conduits: The Journal of Bone and Joint Surgery-American 91: 2194-204.
- Potas JR, Haque F, Maclean FL, Nisbet DR (2015) Interleukin-10 conjugated electrospun polycaprolactone (PCL) nanofibre scaffolds for promoting alternatively activated (M2) macrophages around the peripheral nerve in vivo. Journal of Immunological Methods 420: 38-49.
- Kahraman A, Kahveci R (2015) Evaluating the effect of polytetrafluoroethylene and extractum cepae-heparin-allantoin gel in peripheral nerve injuries in a rat model. CAN J PLAST SURG 23(1).
- Vasconcelos BCE, Gay-Escoda C. (2000) Facial nerve repair with expanded polytetrafluoroethylene and collagen conduits: An experimental study in the rabbit. Journal of Oral and Maxillofacial Surgery 58: 1257-62.
- Shastri V (2003) Non-Degradable Biocompatible Polymers in Medicine: Past, Present and Future. CPB 4: 331-7.
- Ghoreishian M, Rezaei M, Beni BH, Javanmard SH, Attar BM, et al. (2013) Facial Nerve Repair With Gore-Tex Tube and Adipose-Derived Stem Cells: An Animal Study in Dogs. Journal of Oral and Maxillofacial Surgery 71: 577-87.
- Zhang L, Zhou Y, Li G, Zhao Y, Gu X, et al. (2014) Nanoparticle mediated controlled delivery of dual growth factors. Sci China Life Sci 57: 256-62
- Angelova A, Angelov B, Drechsler M, Lesieur S (2013) Neurotrophin delivery using nanotechnology. Drug Discovery Today 18: 1263-71.
- Zhang BGX, Quigley AF, Myers DE, Wallace GG, Kapsa RMI, et al. (2014) Recent advances in nerve tissue engineering. Int J Artif Organs 37: 277-91.
- Muheremu A, Ao Q (2015) Past, Present, and Future of Nerve Conduits in the Treatment of Peripheral Nerve Injury. Biomed Res Int 237507.
- Nakagami H, Morishita R, Maeda K, Kikuchi Y, Ogihara T, et al (2006) Adipose tissue-derived stromal cells as a novel option for regenerative cell therapy. J Atheroscler Thromb 13: 77-81.
- Sasaki R, Aoki S, Yamato M, et al. (2008) Tubulation with Dental Pulp Cells Promotes Facial Nerve Regeneration in Rats. Tissue Engineering Part A 14: 1141-7
Artcle Information
Review Article
Received Date: August 03, 2025
Accepted Date: August 21, 2025
Published Date: August 28, 2025
Journal of Neuroscience Research and Alzheimer’s Disease
Volume 1 | Issue 1
Citation
Banine Khalifeh, Nissrine Ballout, Ali Al Arab (2025) Tissue Engineering in Injured Facial Nerve: A Narrative Review”. J Neurosci Res and Alzheimer's Dis 1: 104
Copyright
©2025 Banine Khalifeh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jnra.2025.1.104