

Research Article
Volume-1 Issue-1, 2022
Critical Care Physiotherapy and Rehabilitation During the Second Wave of the COVID-19 Pandemic, A Single Centre Observational Study. Part I: Physiotherapy Interventions and Functional Outcomes
-
Received Date: January 19, 2022
-
Accepted Date: February 19.2022
-
Published Date: February 22.2022
Journal Information
Switch to Full Text Menu
Abstract
Objectives: To present a description of Critical Care Physiotherapy provision in a London Hospital. Describing the volume and nature of physiotherapy interventions and time to activity milestones in our COVID- 19 population.
Methods: Physiotherapy intervention data was collected between 2nd November 2020 28th February 2021, coinciding with the second COVID- 19 pandemic surge.
Results: 312 patients were included, with 8,249 physiotherapy interventions. Secretion management had the highest frequency intervention from 70-86% across the four months. The achievement of mobility milestones was slower than pre-COVID populations. The average admission and discharge CPAx score was 10.4 and 24.7 respectively.
Conclusions: There is clear focus of interventions for respiratory optimisation and secretion management as opposed to rehabilitation and functional outcomes. It is unclear whether changes in staffing have an impact on time to activity milestones on our COVID- 19 population.
|
Demographics |
||
|
Patient Number |
|
|
|
Total |
312 |
|
|
Gender |
|
% |
|
Male |
199 |
64% |
|
Female |
113 |
36% |
|
Age |
|
SD |
|
Mean years ± SD |
57 |
±13.3 |
|
Ethnicity |
|
% |
|
Asian or Asian British |
160 |
51.3% |
|
White |
89 |
28.5% |
|
Black or black British |
36 |
11.5% |
|
Other |
27 |
8.7% |
|
Length of Stay |
|
SD |
|
Mean ± SD |
17.04 |
±13.52 |
|
Mortality |
|
% |
|
Total and % |
132 |
42% |
|
Ventilated Days |
|
SD |
|
Mean Days ± SD |
12.08 |
±13.07 |
|
Physiotherapy Interventions |
|
|
Secretion Management |
Chest Check and Limb Care Suctioning Ventilator Hyperinflation/VHI
Repositioning Manually Assisted
Cough/MAC Manual Techniques |
|
Weaning |
Ventilator Weaning Tracheostomy Wean |
|
Functional |
Sitting on the Edge of the Bed/SOEOB Sitting out in a chair/SOOBIC Walking |
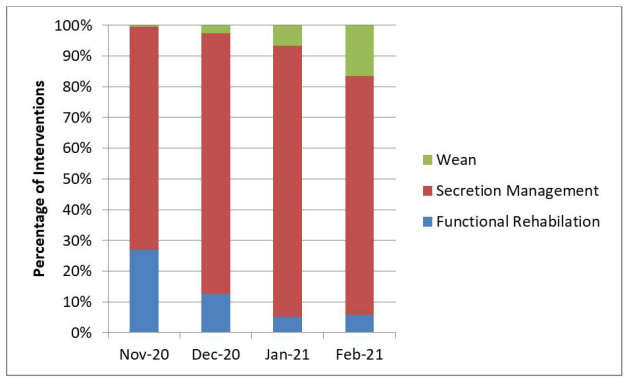 |
| Figure 1: Percentage Intervention by subcategory. (Wean, Secretion Management and Functional Rehabilitation) |
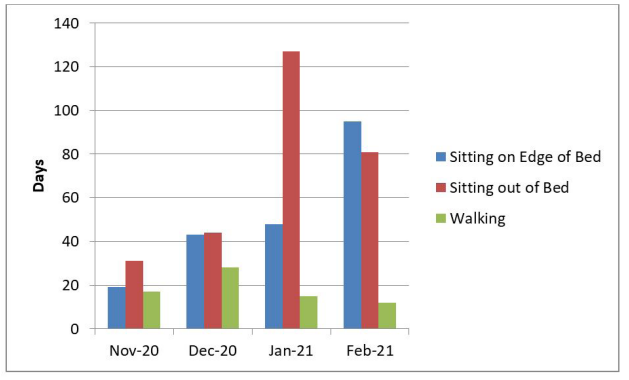 |
| Figure 2: Frequency Of Functional Rehabilitation Interventions: (SOEOB z Sitting Over the edge Of the SOOBIC Sitting out Of in Chair; and Walking) |
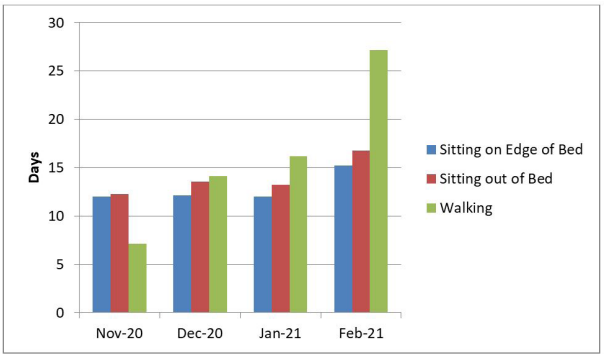 |
| Figure 3: Mean Time in Days to achieve Functional Activity Milestones. (SOEOB z Sitting over the edge Of the bed; SOOBIC Sitting out Of in Chair; Walking) |
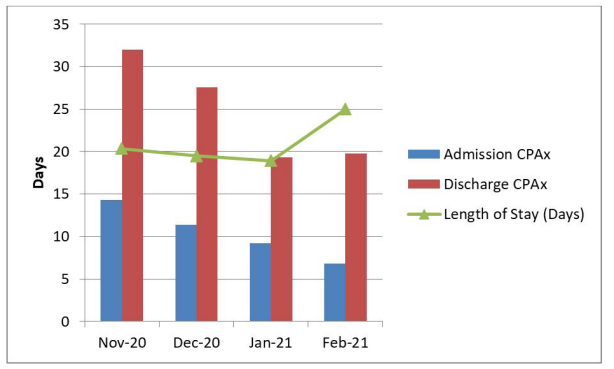 |
| Figure 4: CPAx SCOreS at Critical Care admission and discharge. compared with mean Critical Care length Of Stay |
Introduction
The COVID-19 pandemic resulted in unprecedented demand for critical care. Among the professi01* who contributed to meeting this demand were Physiotherapists; who contribute to the management of intubated and spontaneously breathing patients; develop strategies to manage musculoskeletal pathology and provide rehabilitation to deter the longstanding physical impairments suffered by Critical Care survivors (Vanhorebeek et al, 2020; Gosselink, et al. 2008). This was especially challenging since the role and indications for physiotherapy were uncertain and therapeutic interventions were tX1sed on clinical reasoning rather than clinical evidence.
The second wave of the COVID.19 pandemic at the Royal London Hospital (RLH) provided an opportunity to explore Critical Care Physiotherapy interventions and functional milestones in relation to changing patient volume over a four (4) month period. In Part I; we aim to:
a) Present time to activity milestones in our COVID- 19 cohort
b) Present Chelsea critical care physical assessment (CPAx) scores reflecting physical morbidity at critical care admission and discharge
We hope that outlining the Physiotherapy interventions in a COVID- 19 positive population, alongside functional milestones, and outcomes (via the CPAx tool) provides supportive clinical evidence into the physiotherapy management of COVID- 19 positive patients and contributes to on-going predictive modelling and debate [1-4].
Methods
Setting: This was a single centre observational project completed in the Adult Critical Care (ACCU) and Queen Elizabeth Unit (QEU) of the Royal London Hospital (RLH), London, United Kingdom. The QEU is an open plan unit constructed specifically for the increase of COVID.19 patients requiring critical care admission. There was a maximum capacity of 124 critical care beds in the QEU and a further 44 beds in the ACCU
Physiotherapy Interventions: COVID-19 patients were assessed by a Physiotherapist within 24 hours of admission. Interventions were determined through clinical reasoning and referencing the critical care standard operating procedure (SOP). The SOP described safe practice for aerosol generating procedures common in respiratory physiotherapy and a prioritisation tool to support clinical decisions in relation to staff capacity For example, patients with urgent respiratory needs were prioritised over patients with rehabilitation needs alone A list of intervention options can be seen in the supplemental material
Data collection: All COVID-19 patients admitted to critical care over the data collection period were included. Data was collected retrospectively between 2nd November, 2020 and 28th February. 2021 coinciding with the second COVID- 19 surge in the United Kingdom. Data was extracted per patient. per day (by authors MC, J R, WK, J P, AS, HP and KL) from the electronic record and retrospectively entered into a password protected spreadsheet, stored locally in compliance with general data protection regulation (GDPR 2018). Data extracted included; demographic information; admission and discharge dates from critical care; days of mechanical ventilation; and up to three Physiotherapy interventions each day creating a chronological record of each patient' critical care experience.
Physical morbidity of the sample was measured using CPAx at critical care admission and discharge (Corner et al, 2012). CPAx is a measure of physical morbidity in general critical care cohorts. "lhere are 10 CPAx domains with a score from zero (complete dependence) to five (complete independence). As we were unable to measure handgrip strength during the pandemic, the maximum CPAx score anticipated was 45, rather than 50.
Derived Data: Physiotherapy interventions were categorised into three groups representing 1) Secretion Management; 2) Weaning Interventions and 3) Functional Rehabilitation consisting of 3 different domains: Sitting on the edge of the bed (SOEOB), sitting out of the bed in the chair (SOOBIC) or Walking. Please see supplementary info for full intervention outlines. Mean monthly intervention frequency could be calculated for each intervention and each category, along with the time (in days) from critical care admission to first achieving the functional rehabilitation milestones We derived the frequency of interventions per occupied bed and per therapist as a monthly average Other derived data included days of mechanical ventilation and critical care length of stay.
Data Management and Analysis: The characteristics of the cohort were summarised with continuous variables reported as means ± standard deviations and medians and interquartile ranges (IQR) reported otherwise. A descriptive analysis of the data was completed outlining the frequency of intervention type per month and the mean ± standard deviations time to achievement of 3 functional milestones
Ethical Considerations: Ethical approval and patient consent were not required as the project was registered as a service evaluation by the clinical effectiveness unit at The Royal London Hospital. There was no deviation from usual care for any patient, the project was observational.
Results
312 patients (64% male, 36% female) required critical care admission over the 4 month period. "Iheir mean age was 57 ± 13.3yrs and 51.3% were of Asian or Asian British ethnicity Ihe sample experienced a 42% mortality. For survivors, the mean length of ventilation was 12 ± 13.07 days and critical care stay was 17 ± 13.5 days (Table 1).
The intervention type delivered across the time is demonstrated in Figure 1. Secretion management techniques quired with the highest frequency representing 70%, were re 82%, 86% and 77% of the total interventions delivered from the first to the fourth month respectively Weaning strategies were required with a very low frequency in the first month (0.4% of the total interventions), but increased incrementally to represent 2.6%, 6.6% and 16.5% of the total interventions delivered in Dec 2020, Jan 2021 and Feb 2021 respectively. The frequency of weaning interventions in the last three months was driven more by an increased requirement for tracheostomy weaning compared to ventilator weaning. 17 tracheostomy weaning interventions occurred in Dec 2020, 231 in Jan 2021, and 535 in Feb 2021. In comparison, ventilator weaning was infrequent with 1 intervention in the first month, 7 in Dec 2020, 16 in Jan 2021 and 9 interventions only in Feb 2021.
Functional rehabilitation represented 26% of the total interventions in the first month, but declined to 12% in the second, 5% in the third and 6% in the last month (Figure 1). Figure 2 demonstrates the numlkr and type of rehabilitation interventions which were delivered each month across the time period. Sitting out of bed in a chair cncurred with the highest frequency, occurring 31, 44, 127 and 81 times in the first to fourth month respectively. Walking interventions occurred with the lowest frequency across the data collection period.
The mean time from critical care admission to achieve functional rehabilitation milestones is depicted in Figure 3. The mean time to first sitting on the edge of the (SOEOB) occurred consistently at 12 ± 14.4 days for the first three months, increasing to 15 ± 13.3 days in the last month. Mean time to sitting out of bed in a chair (SOOBIC) occurred at 12 ± 17.8 days in the first month, 13.5 ± 15.9 days in the second, 13.2 ± 13.6 days in the third and 16.7 ± 14.4 days in the last month. In contrast, the mean time to walk increased each month from 7.1 ± 3.3 days in Nov 2020 to 14.12 ± 17 days in Dec 2020, 16.2 ± 17 days in Jan 2021 and 27.18 ± 16.4 days in Feb 2021.
For the second COVID.19 surge, our institutions average admission and discharge CPAx score was 10.4 and 24.7 respectively. Figure 4 depicts the admission and discharge scores in relation to mean length of stay.
Discussion
This single-centre observation describes the Physiotherapy service delivered to patients in Adult Critical Care at the Royal London Hospital with laboratory confirmed COVID-19 infection over a 4-month period. The COVID-19 pandemic presented a unique opportunity to assess the impact of therapist to occupied bed ratios on therapeutic metrics and functional outcomes in a population with acute hypoxic respiratory failure. Historically, lack of homogeneity within critically ill populations has been a problem when comparing patient outcomes. The COVID- 19 Pandemic provided an opportunity to overcome this limitation.
In the United Kingdom Critical Care Physiotherapists are responsible for providing respiratory care, secretion management, ventilation weaning plans, tracheostomy management and the initiation of functional mobility In total we delivered 8,249 Physiotherapy interventions to 312 COVID- 19 positive patients over the 4-month data collection The incidence of total Physiotherapy intervention is rarely reported in Critical Care Physiotherapy literature and comparisons are limited by methodological differences and reporting styles. For example, Black et al (2021) reported 2171 documented Physiotherapy sessions for 97 ventilated patients across a three. month period during the first COVID.19 pandemic surge, while our previous publication (Rich et al 2021) observed 3106 physiotherapy interventions delivered to 213 mixed COVID-19 positive and negative patients irrespective of their ventilation status over an 8 week period. Pre-COVID- 19 related critical care Physiotherapy incidence reporting is plagued by similar issues. For example, McWilliams et al (2018) re-B»rt a total of 560 completed rehabilitation sessions in their control group, and 616 sessions in their enhanced care group over 15 months, although patients were included if they had received mechanical ventilation for at least 4 days only, and Knott et al (2015) reported 194 Physiotherapy sessions which included rehabilitation interventions, for patients who were admitted to critical care for greater than 48 hours.
Of the total number of interventions reported in our study, greater than 70% were designed to manage pulmonary secretions. These techniques included assessing the need for secretion management intervention, suctioning events, manually assisted coughing, manual techniques, ventilator and repositioning. During the peak month, secretion management represented 86% of the total physiotherapy intervention delivered Black et al (2021) reported an unanticipated volume of COVID-19 patients with excess secretion load and 66% of documented treatment sessions involving at least one airway clearance technique due to absent or ineffective cough, levels of sedation and neuromuscular blcxkade. Notably, these authors identified the need for 2 physiotherapists to deliver these treatments, as further illustration of the staffing burden these techniques represent. In our earlier paper we reported 44% of the total interventions were associated with secretion management (Rich et al 2021). An explanation for the st—ring increase in these techniques during this surge lies in our improved classification of respiratory assessment which was incorporated into the secretion management category.
Functional rehabilitation interventions represented only 6% of the total intervention incidence over our time period. During the previous wave, rehabilitation interventions represented 17% of the total volume of physiotherapy delivered (Rich et al 2021). In contrast, during pre-pandemic periods the incidence of rehabilitation techniques, as a percentage of the total of physiotherapy interventions, has been reported as high as 55% (Thomas et al 2009), 51% (Knott et al 2015) and 41 % (Patel et al, 2010). Despite the confirmed importance of early rehabilitation in patients with critical illness, several authors (McWilliams et al. 2021; Escalaon et al. 2020) have noted the impact of the COVID- 19 pandemic on the culture of critical care, shifting to early discharge of stable patients to accommodate admission demand, which de-emphasises early mobility.
Another method of reporting the incidence of functional rehabilitation has been to report the time to achieve functional milestones within the critical care setting. These metrics were first reported as methods to evaluate service improvement (Morris et al 2008), or secondary critical care outcomes (Schweickert et al 2009) More recently, time to activity metrics have become a standard for benchmarking rehabilitation within critical care, particularly recording the first time to mobilisation, such as sitting over the edge of the bed (Knott et al, 2015; Van Willigen et al 2016; McWilliams et al 2018), or the highest level of mobility achieved at critical care discharge (McWilliams et al 2021). The time point from which these metrics have been calculated is not always reported, and may vary between investigators. We reported the mean time to achieve 3 functional milestones (SOEOB, SOOBIC and walking) in our COVID.19 cohort, calculated from critical care admission, since not all of our patients were invasively ventilated [5-8].
The only time to activity metric which we can compare to similar investigations is the mean time to SOEOB, representing the number ofdays to first mobilisation from critical care admission. We report a consistent value of 12 ± 14.4 days for the first three months which increased to 15 ± 13.3 days in the last month. Similarly, McWilliams et al (2021) reported a mean (± SD) time to first mobilisation of 14 ± 7 days in their COVID- 19 ventilated cohort. Ihese values are consistently longer than reports in pre- COVID-19 populations. For example, McWilliams et al (2018) reported 8 days to first mobilisation in the intervention group of their randomised controlled trial; Van Willigen et al (2016) reported time to first mobilisation ranging between 4.3 and 9.3 days over 4 improvement cycles in a general intensive care unit, while Knott et al (2015) report a median time to commencing active rehabilitation from ICU admission of 3 days [9-12].
Our mean time to SOOBIC and walk were also consistently longer than reported values from pre-COVID. 19 populations (Thomas et al Patel et al 2010) and increased across the 4-month period, achieving the longest durations in the final month of data collection. These findings are curious and may reflect that when patient volume was low (initially), there was a focus on rehabilitation and transition to home. As patient volume increased and stretched capacity, the therapy emphasis switched from rehabilitation to respiratory priorities to promote critical care discharge. It is also likely that patients who remained critically ill in the last month of data collection had higher disease severity/organ support and were not clinically stable enough to participate in rehabilitation activities, supported by worse admission and discharge CPAx scores in the months Of Jan and Feb. Longer length of stay for patients in our final month further reinforces this possibility. As our mean duration of ventilation was also 12 days, we propose that our time to activity followed the cessation of ventilation and associated sedation requirements.
McWilliams et al (2021) recognised additional barriers to mobilisation in their COVID.19 cohort including the capacity of the nursing workforce to assist with rehabilitation tasks, the high proportion of patients with delirium and the impact of high BMI on time to first mobilise, At the Royal London Hospital, the purpose built "open plan" structure of the Queen Elizabeth Unit reinforced multidisciplinary team (MDT) working and nursing teams took initiative for low.risk rehabilitation plans, However, complex rehabilitation interventions for patients with critical care induced muscle weakness often req uire multiple skilled staff and specialist equipment to complete, Ntoumenopoulos (2015) described the requirement for up to five staff to assist a patient to mobilise from the bed, taking into consideration acquired muscle weakness, ventilator support and other lines and devices which must be managed safely during the task [13,14].
It remains difficult to determine whether the low frequency of rehabilitation interventions, and extended time to achieve mobility milestones was due to clinical instability or clinical judgement, taking into consideration risk assessment, staff and equipment availability. It is possible that rehabilitation incidence was consistent with available staff resources on any given day, especially since inadequate staffing is a recognised barrier to physical rehabilitation of mechanically ventilated patients (Mendez-Tellez et al 2013). It is also possible that our previous COVID- 19 pandemic experience impacted our clinical reasoning. Anecdotally, early functional activity appeared to be detrimental in the acute COVID-19 cohort who present with excessive work of breathing out of proportion to the physical activity performed. COVID-19 remains a novel disease with limited data concerning the functional milestones expected of this cohort [11-14].
Our description of critical care Physiotherapy intervention during the second pandemic wave demonstrates a clear focus of interventions for respiratory optimisation and secretion management as opposed to rehabilitation and functional outcomes. Part II of our study looks at further detail the relationship of periods of highJlow productivity within a workforce and its possible effect on functional outcomes and activity metrics. does not appear to an association between volume of interventions delivered or staff prcxiuctivity and duration to achieve functional milestones.
Limitations
This was a single centre observation and may not be representative of the experience of other sites, Our data is inclusive of all patients who occupied a critical care bed during the study period. We did not exclude patients who did not survive the admission or patients that did not require invasive ventilation. We collected data continuously throughout each patient journey, therefore monthly representations of patient numbers were mutually inclusive. An individual patient's data might appear over several months depending on their overall length of critical care stay. Our choice of recorded outcomes for activity and rehabilitation events was dictated by usual clinical practice in our critical care, such that comparison to other recognised mobility scales reported in comparable literature is not possible. No information was recorded the underlying decision making of the Physiotherapists regarding applied interventions. or reasons to not treat a patient. Understanding the clinical reasoning may have supported identification of barriers and strengthened any association with low rehabilitation incidence. We did not follow our patients through to hospital discharge to report hospital discharge destination, or the need for on- going rehabilitation. Ihe COVID-19 pandemic has highlighted limitations in rehabilitation provision for critical care survivors and a greater proportion of COVID•19 patients requiring inpatient and community rehabilitation compared to patients without COVID- 19 (Puthucheary et al 2021) [5-18].
Conclusions
We have presented a description of the Critical Care Physiotherapy service delivered to patients with confirmed COVID-19 over a four-month period coinciding with the second pandemic wave at one London Hospital. We have reported time to activity metrics and CPAx scores. While many previous studies have demonstrated early mobilisation of critically ill patients equates to improved functional outcomes, our rehabilitation intervention incidence was small in comparison to the volume of respiratory interventions delivered. Over the four-month period our time to achieve mobility milestones were progressively longer than previously reported for pre-COVID.19 populations. Competing clinical demands dictated by prioritisation of respiratory management clearly influenced these observations, particularly since many respiratory and rehabilitation tasks require more than one therapist to safely perform. It remains unclear whether further enhancement of the therapist to occupied bed ratio would have altered the percentage of treatment modalities observed in this study. Further investigation of the barriers to rehabilitation participation may assist in defining ideal Physiotherapy staffing requirements in critical care.
References
- Black C, Klapaukh R, Gordon A, Scott F, Holden N (2021) Unanticipated demand of Physiotherapist-Deployed Airway Clearance during the COVID.19 Surge 2020, a single centre report. Physiotherapy.
- Corner E, Wooda H, Englebretsena C, Thomas A, Grant RL, Nikoletouc D, Soni N (2012) The Chelsea Critical Care Physical Assessment Tool (CPAx): validation of an innovative new tool to measure physical morbidity in the general adult critical care population; an observational proof.of.concept pilot study. Physiotherapy,
- Escalaon NIX, Herrera J (2020) Adapting to the coronavirus disease 2019 pandemic in New York City. American J Physical Medicine and Rehabilitation, 453-8.
- Gosselink R, Bott J, Johnson M, Dean E, Nava S, et al. (2008) Physiotherapy for adult patients with critical illness: recommendations for the European Respiratory Society and the European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically ill Patients. Intensive Care Medicine 34: 1188-99.
- Hmigson C (2012) ICU Activity Codes and Definitions, http://www.mobilization-network.org/Network/.
- Knott A, M, Harlow SKM (2015) Benchmarking rehabilitation practice in the intensive care unit. J the Intensive Care 16:24-30.
- McWilliams D, Jones C, Atkins G, Hodson J, Whitehouse J, et al- (2018) Earlier and enhanced rehabilitation of mechanically ventilated patients in critical care: A Feasibility randomised controlled trial Journal of Critical Care 44:407-12.
- McWilliams D, Weblin J, Hodson J, Veenith T, Whitehouse T, et al. (2021 ) Rehabilitation levels in patients with COVID- 19 Admitted to Intensive Care Requiring Invasive Ventilation. Ann Am Thorac Soc 18:122-9.
- Mendez-Tellez PA, Dinglas VD, Colantuoni E, Ciesla N, Sevransky JE, et al. (2013) Factors associated with timing of initiation of physical therapy in patients with acute lung injury. J Critical Care 28.
- Morris PE, Goad A, Thompson C, Taylor K, Harry B, et al. (2008) Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Critical Care Medicine, 36:2238-43.
- Ntoumenopoulos G (2015) Rehabilitation during mechanical ventilation: Review of the recent literature. Intensive and Critical Care Nursing 31:125-32.
- Patel M, Thomas AJ, Boot S (2010) Time to activity within a general/trauma Intensive Care Unit. J ACPRC 42:35.
- Puthucheary Z, Brown C, Corner E, Wallace S, Highfield J, et ale (2021) The Post.ICU presentation screen (PICUPS) and rehabilitation prescription (RP) for intensive care survivors part II: Clinical engagement and future directions for the national Post-Intensive care Rehabilitation Collaborative. J the Intensive Care Society.
- Rich J, Coman M, Sharkey A, Church D, Pawson J, Thomas AJ (2021) A single center observational study of the incidence, frequency and timing of critical care physiotherapy intervention during the COVID- 19 pandemic. J the Intensive Care Society.
- Schweickert WI, Pohlman NIC, Nigos C, Pawlik AJ, Esbrook CL, et al. Early physical and occupational therapy mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet 373: 1874-82.
- Thomas A, Wright K, Mill L 'Ihe incidence of physiotherapy practice and rehabilitation activities within a general intensive care unit. J ACPRC 49: p3-8.
- Vanhor&ek I, Latronico N, Van den Berge G (2020) ICU- acquired weakness. Intensive Care Medicine 46:637-53.
- Van Willigen Z, Collings N, Richardson D, Cusack R (2016) Quality improvement: The delivery of true early mobilisation in an intensive care unit. BMJ Quality Improvement Reports, 5: 11211734.w4726.
Article Information
Research Article
Received Date: January 19, 2022
Accepted Date: February 19, 2022
Published Date: February 22.2022
Critical Care Physiotherapy and Rehabilitation During the Second Wave of the COVID-19 Pandemic, A Single Centre Observational Study. Part I: Physiotherapy Interventions and Functional Outcomes
Volume 1 | Issue 1
Citation
Mark Coman (2022) Critical Care Physiotherapy and Rehabilitation During the Second Wave of the COVID-19 Pandemic, A Single Centre Observational Study. Part I: Physiotherapy Interventions and Functional Outcomes. J Phys Rehabil Physiotherapy l: 1-10
Copyright
©2025 Mark Coman. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jprp.2022.1.101