

Research Article
Volume-1 Issue-1, 2022
Critical Care Physiotherapy and Rehabilitation During the Second Wave of the COVID-19 Pandemic, A Single Centre Observational Study. Part II: Physiotherapy Workforce Metrics and Productivity
-
Received Date: January 19, 2022
-
Accepted Date: Februarv 19, 2022
-
Published Date: February 22.2022
Journal Information
Switch to Full Text Menu
Abstract
Objectives: Objectives: To present a description of Critical Care Physiotherapy staffing during the COVIDI 9 pandemic in a London Hospital. Including calculations of occupied to physiotherapy staff ratios and staff productivity.
Methods: Physiotherapy intervention data was collected between 2nd November 2020 28th February 2021, coinciding with the second COVID.19 pandemic surge, Staffing numbers were collected throughout this period, allowing calculation of staff to occupied bed ratios and staff productivity
Results: Staff productivity ranged from 44% to 130% and physiotherapist to occupied bed ratio ranged from to 1:11.
Conclusions: Staffing ratios are common practice for nursing but are novel for allied health professionals. It is unclear whether changes in staffing have an impact on time to activity milestones in our COVID-19 population. The practice of redeploying staff to improve staffing ratios is complex and training time needs to be considered for this to have a positive impact on staff productivity.
|
Demographics |
||
|
Patient Number |
|
|
|
Total |
312 |
|
|
Gender |
|
% |
|
Male |
199 |
64% |
|
Female |
113 |
36% |
|
Age |
|
SD |
|
Mean years ± SD |
57 |
±13.3 |
|
Ethnicity |
|
% |
|
Asian or Asian British |
160 |
51.3% |
|
White |
89 |
28.5% |
|
Black or black British |
36 |
11.5% |
|
Other |
27 |
8.7% |
|
Length of Stay |
|
SD |
|
Mean ± SD |
17.04 |
±13.52 |
|
Mortality |
|
% |
|
Total and % |
132 |
42% |
|
Ventilated Days |
|
SD |
|
Mean Days ± SD |
12.08 |
±13.07 |
|
Physiotherapy Interventions |
|
|
Secretion Management |
Chest Check and Limb Care Suctioning Ventilator Hyperinflation/VHI
Repositioning Manually Assisted
Cough/MAC Manual Techniques |
|
Weaning |
Ventilator Weaning Tracheostomy Wean |
|
Functional |
Sitting on the Edge of the Bed/SOEOB Sitting out in a chair/SOOBIC Walking |
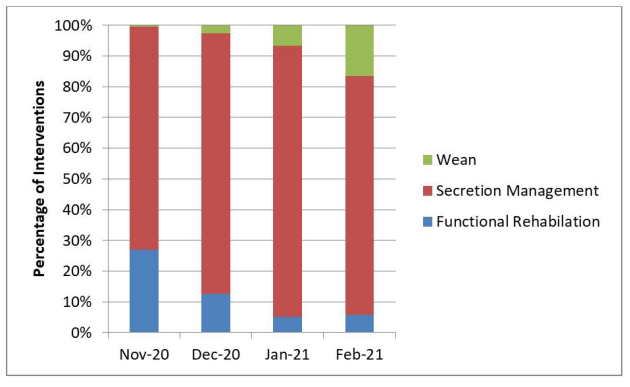 |
| Figure 1: Percentage Intervention by subcategory. (Wean, Secretion Management and Functional Rehabilitation) |
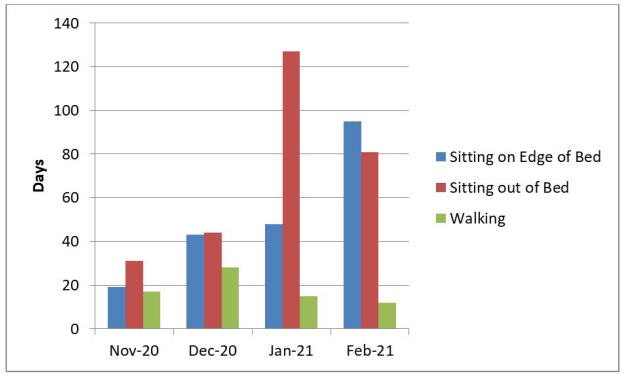 |
| Figure 2: Frequency Of Functional Rehabilitation Interventions: (SOEOB z Sitting Over the edge Of the SOOBIC Sitting out Of in Chair; and Walking) |
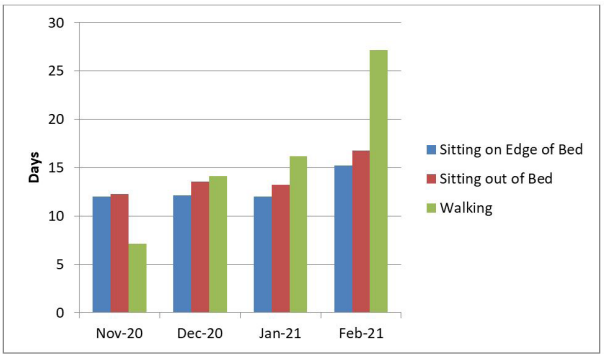 |
| Figure 3: Mean Time in Days to achieve Functional Activity Milestones. (SOEOB z Sitting over the edge Of the bed; SOOBIC Sitting out Of in Chair; Walking) |
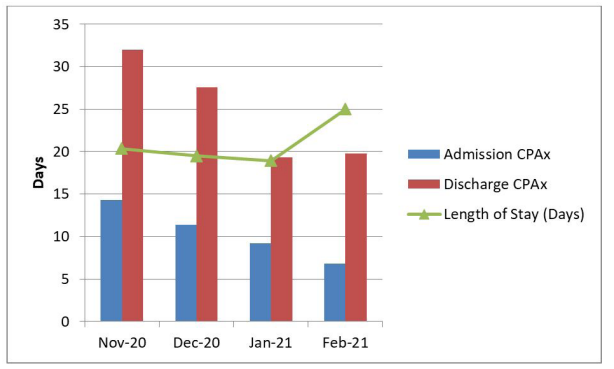 |
| Figure 4: CPAx SCOreS at Critical Care admission and discharge. compared with mean Critical Care length Of Stay |
Introduction
The COVID.19 pandemic resulted in unprecedented demand for all critical care staff including physiotherapists. Estimating the Physiotherapy labour requirement for the number of patients admitted to critical care during the pandemic was problematic. With the rapid increase in demand for critical care beds this presented a challenge to develop safe staffing guidelines in an unfamiliar environment (Escalaon, 2020) [1]
Although guidelines for Intensive Care Services in the United Kingdom exist (GPICS, 2019), what constitutes appropriate staffing during a respiratory pandemic is less clear. In addition, historical methodologies used in workforce planning remain rudimentary and poorly substantiated (Cartmill et al 2012). For example, ratio-based methodologies compare staff to an activity variable (beds, bed-days, or activities) which may be established at a service level or externally referenced from professional standards (Ridoutt, et al, 2006, Shipp, 1998). These methods rarely consider the percentage of time devoted to direct clinical care compared to supporting professional activities (NHSi, 2019) and descriptions ofratio calculations which accommodate 7 day or extended hours working are rare. In addition, ratio methodology is rarely able to establish links between staffing and a desired health outcome (Mudge et al Importantly, evidence for labour efficacy or productivity remain unreported in the ratio-based taxonomy [2-4].
The Second Wave of the COVID- 19 pandemic at the Royal London Hospital (RLH) provided an opportunity to explore Critical Care Physiotherapy incidence and outcome in relation to changing patient volume, staffing configuration and service provision over a four (4) month period. Since workforce increased incrementally with patient volume and occupied critical care beds over the time period, In Part II; we aim to:
- Present a description of our Critical Care Physiotherapy service, including the method of calculating our therapist to occupied bed ratios and a methodology for establishing staff productivity adapted from the World Health Organisation (WHO, 2019) Workload Indicators of Staffing Need (WISN) (full details in Supplementary Information Application A)
- Describe the volume and nature of Physiotherapy delivered each month by the Physiotherapy workforce to occupied bed ratio We hope that illustrating the granular detail ofworkforce metrics with productivity during the COVID- 19 pandemic supports recognition of the complexity asscxiated with Physiotherapy workforce planning, and contributes to on-going predictive modelling and debate.
Methods
This was a single centre observational project completed in the Royal London Hospital (RLH), London, United Kingdom. Please see Part I for more details of the setting, data collection method and data management.
Physiotherapy Staffing: The increase in COVID- 19 admissions and expanded critical care elicited a graded therapy staffing response, reaching a peak of 26 Physiotherapists in January 2021. Core services were delivered between Sam and 6pm Monday to Friday, with a prioritised physiotherapy weekend service, and overnight on-call from 6pm to Sam. Redeployed therapists were provided with local induction and clinical skills training. All therapy staff were fit tested and provided with Protective Equipment (PPE) training.
Staffing Ratios:Physiotherapist to occupied patient ratios were calculated by using the number of beds occupied by COVID-19 patients and dividing this by the number of Physiotherapists dedicated to providing the COVID-19 Physiotherapy service. Due to differences in the weekday / weekend prioritised service we calculated a ratio for weekdays and for weekends separately, then combined these ratios to calculate a monthly average.
Productivity Calculation:A modified version of the World Health Organisations Workload Indicators of Staffing Need (WISN: WHO, 2019) was used This human resource tool, developed by the World Health Organisation (WHO) provides a systematic process to guide staffing decisions to optimise human resource management. Ihe application of this allowed calculation of productivity, staffing levels and interventional data. For full application ofthe WISN please refer to supplemental information (Application A).
Ethical Considerations: Ethical approval and patient consent were not required as the project was registered as a service evaluation by the clinical effectiveness unit at The Royal London Hospital, There was no deviation from usual care for any patient, the project was observational
Results
Patient volume and critical care bed capacity increased over the first 3 months peaking in Jan 2021 when 3(1) critical care patients were cared for in 127 critical care beds. In the last month (Feb 2021 ), these numbers reduced to 183 patients, cared for in critical care beds. The Physiotherapist to cxcupied bed ratio changed monthly from I Physiotherapist for every 11 beds in the first month (Nov 2020), to 1 Physiotherapist for every 9 beds in the fourth month (Feb 2021). Table I demonstrates how increased critical care beds and Physiotherapy availability elicited increases in the number of interventions delivered from 260 interventions in Nov 2020 to 3,759 interventions in Jan 2021. These numbers equate to 10.8 interventions per month per bed in Nov 2020, 18 in Dec 2020, 29.6 in Jan 2021 and 36.6 in Feb 2021. Productivity was calculated as 64% in Nov 2020, 44% in Dec 2020, 86% in Jan 2021 and 130% in Feb 2021 [5-7].
interventions in their COVID- 19 cohort. A previous report (Rich et al 2021), exploring Physiotherapy in a COVID.19 positive and negative cohort reported a Physiotherapist to bed ratio of 1:5, a value which aligned with Black et al (2021) and approximated the Faculty of Intensive Care Medicine in the United Kingdom (GPICS, 2019) and the European Intensive Care Society (Valentin and Ferdinande, 2011 ) recommendations [8,9]
Given the variance in reported therapist to patient, and therapist to occupied critical care bed ratio's above, we present a translation of our staffing ratios into productivity metrics as a tool to evaluate service provision. Productivity can be defined as the rate of work per unit, where the work represents interventions delivered (converted to a time unit) and the unit represents the available therapy staff hours (accounting for non- clinical activity). Staffing enhancement (as occurred during)
Discussion
Ratio-based staffing is well established for professions such as nursing and medicine (NQB/CNO 2013; RCP 2018) but less so for the allied professions. Disclosure of our therapist to occupied bed ratio is novel with respect to other critical care physiotherapy literature where staffing ratios are rarely reported (Rich et al, 2021). Over the 4 month period, our therapist to critical care occupied bed raticß varied between l: 9 and 1: 11. McWilliams et al (2021) report one physiotherapist for every 10 patients in a study of rehabilitation in COVID.19 patients requiring invasive ventilation. In contrast Black et al (2021) described the need for 1 therapist for every 5 beds occupied by intubated and ventilated patients to accommodate the large volume of secretion clearance interventions they observed. and the need for more than one physiotherapist to deliver these the pandemic) increases available working hours, but this enhancement did not automatically improve work productivity in the initial period. Our low derived productivity scores in the first 2 months may a period of "over. staffing" but more likely this period was associated with increased non.clinical activity allocation. Tasks such as training and up-skilling, strategic planning, developing resources and role allocation were occurring alongside clinical delegation and supervising interventions. These non-clinical tasks were necessary to ensure staff met minimum standards of critical care clinical practice (Twose, et al 2019), and had an appreciation of the evidence base underlying treatment recommendations in this environment (Hanekom et al 2011; Sommers et al, 2015; Van Willigen et al, 2016; Schweickert et al, 2009; Ntoumenopoulos, 2015; ) , and the recommended staff required to complete interventions (Green et d, 2016) (8-15].
It is noteworthy that during the first two months of data collection, caseload commitments of our staff were divided between a COVID- 19 negative cohort on ACCU and COVID 19 positive cohort on QEU, This situation changed at the end of December when the caseload of COVID- 19 positive patients dominated the workload, partially accounting for the low productivity values in the first two months of data collection.
We also recognise that less experienced staff may take more time to evaluate, plan and complete interventions, and that our activity standards may have poorly estimated the actual time inexperienced staff spend delivering interventions. Other factors such as donning and doffing, providing clinical assistance outside predetermined therapy tasks and orienting to a constantly adapting working process were also likely to have influenced the 0.2WTE non-clinical allocation we applied. As staff training, supervision and delegation reduced in the later months of the analysis, productivity scores improved to 86% and 130% respectively, despite escalating patient numbers. These productivity scores that the available clinical working time was appropriate for the number of interventions required or the non-clinical time allocation was reduced as work processes became more efficient [ 16-18]
The advantages of evaluating productivity in relation to therapist to occupied bed ratio include an appreciation of the time commitment associated with non-dinical tasks which increases throughout the clinical bandings, and recognition of the impact of sickness and annual leave on caseload performance. For example, the productivity asscxiated with Dec 2020 was low, but accurately reflected the number of staff who required sickness absence due to isolation and authorised leave over Christmas. However, productivity as a derived metric does not recognise patient complexity and represents patients as negating human factors such as rapport. It is difficult to establish the relationship between productivity and quality patient care when patient reported qualitative feedback has not been sought.
In addition, productivity metrics do not reflect whether the Physiotherapy needs of our critical care patients were being met. Evaluating the need for Physiotherapy intervention in critical care and its objective assessment remains an area of contention which is difficult to quantify outside individual therapist clinical reasoning (Rich et al, 2021) although evidence-based Physiotherapy recommendations for adult patients with critical illness do exist (Gosselink et al 113-15]. Critical Care Therapy services are historically delivered using a prioritisation model necessitated by workforce capacity, where daily patient needs may not be met due to insufficient staffing, or excessive workload. We suggest that recording accurate staffing ratios and deriving productivity scores to align with the incidence frequency and timing of physiotherapy may be a starting point to explore this issue.
Our description of critical care Physiotherapy intervention during the second pandemic wave demonstrates a clear focus of interventions for respiratory optimisation and secretion management. There does not appear to be an association between volume of interventions delivered or staff productivity and duration to achieve functional milestones. During the final month of the analysis staff pr(kåuctivity was high, and rehabilitation tasks continued to be delivered, yet time to achieve activity metrics was prolonged in comparison to preceding months [19-21].
Limitations
This was a single centre observation and may not be representative of the experience of other sites. Our data is inclusive of all patients who occupied a critical care bed during the study period. Consequently, care must be taken when comparing this data to other reports detailing the experiences of invasively ventilated patients or critical care survivors. Although our aim was to provide a descriptive analysis of our observations, lack of statistical testing of observed associations explains our low confidence in definitive interpretation of the data.
Conclusions
We have presented a description oftheCritical Care Physiotherapy service delivered to patients with confirmed COVID-19 over a four-month period coinciding with the second pandemic wave at one London Hospital. We have described Physiotherapy availability each month, in terms of therapist to occupied critical care bed ratios, and provided a methodology for reporting productivity in relation to the time required to deliver both the volume and nature of interventions. Despite staff productivity improving over the four-month period our time to achieve mobility milestones were progressively longer than previously reported for non-COVID- 19 populations. Competing clinical demands dictated by prioritisation of respiratory management clearly influenced these observations, particularly since many respiratory and rehabilitation tasks require more than one therapist to safely perform. It remains unclear whether further enhancement of the therapist to occupied bed ratio would have improved the percentage of rehabilitation activity observed. Further investigation of the barriers to rehabilitation participation may assist in defining ideal Physiotherapy staffing requirements in critical care.
Supplementary information
Application A: Workload Indicators of Staffing Need (WISN: WHO, 2019)
The WISN method is based on a health worke€s workload, with activity (time) standards applied for each workload component. The method:
- Determines how many health workers of a particular type are required to cope with the workload of a given health facility
- Assesses the workload pressure of the health workers in that facility
Firstly, the available working time (AWT) per month is calculated by factoring all authorised and non-authorised staff absences, such as: non-working and training days, sickness and annual leave:
AWT- [A - (B + C + D + E)] x F
where,
- AWT is the total available working time per month (Hrs)
- A is the number of possible working days per month (Days)
- B is the number of days off for public holidays per month (Days)
- C is the number of days off for annual leave (actual) per month (Days)
- D is the number of days off due to sick leave (actual) per month (Days)
- E is the number of days off due to other leave, such as training. per month (Days)
- F is the number of working hours in one day (Hrs)
The AWT per month represents the total time available for each therapist to complete all work requirements, including clinical and non-clinical support or additional activity (as depicted in Table X).
For this project we estimated non-clinical activities represent 0.2 whole time equivalent (WTE) or 7.44 hours per week per therapist. This estimation recognises the decreasing clinical expectations of each grade as banding prcvesses (Band 8 with a 0.5 clinical commitment, to Band 5 with a 0.9 clinical commitment),
Subsequently, clinical activity availability was averaged for all staffing at 0.8 to provide a total clinical available working time per month (Hrs) according to the formula.'
TCAWT - AWT x 0.8
Where,
- TCAWT is an individual's total clinical available working time per month (Hrs)
- AWT is the total available working time per month (Hrs)
The team TCAWT can be calculated for a staff compliment (n) resulting in the total clinical available time for the entire workforce, per month:
TCAWT x (n) = Team TCAWT
where,
- TC„AWT is total clinical available working time per month (Hrs)
- (n) is the number of therapists
- Team TCAWT is the workforce total clinical available working time (Hrs)
The next step is to standardise service delivery activity by assigning a time unit to each clinical activity. The time unit represents the time necessary for a well-trained, skilled, and motivated worker to perform to professional standards in the local circumstances (WISN, WHO, 2019). An example of the standards used for this project are outlined in Table Y.
Therapist discretion was used as the amount of time devoted for each treatment session as treatment time can vary
These time standards can be applied to each of the recorded physiotherapy interventions to enable the calculation of a time commitment associated with delivery of the number and type of interventions recorded per month.
TCRWT - (PAALC (n) x 0.75hrs) + (SM (n) x + 0.75/1hrs) + (FR (n) x 0.75/1 hrs) + (W (n) x 0.5hrs)
where
- TCRWT is the total clinically required working time per month (Hrs)
- PAALC is the number of physical assessment and limb care interventions per month
- SM is the number of secretion management interventions per month
- FR is the number of functional rehabilitation interventions per month
- W is the number of weaning interventions per month.
Productivity can then be calculated by comparing the TCRWT and the Team TCAWT to generate a percentage value:
Productivity = TCRWT/ Team TCAWT
where
- Productivity is the % of available work time required to deliver interventions.
- TCRWT is the total clinically required working time per month (Hrs)
- Team TCAWT is the workforce total clinically available working time (Hrs)
References
- Black C, Klapaukh R, Gordon A, Scott F, Holden N (2021) Unanticipated demand of Physiotherapist-Deployed Airway Clearance during the COVID.19 Surge 2020, a single centre report. Physiotherapy
- Cartmill L, Comans TA, Clark MJ, Ash S, Sheppard L (2012) Using staffing ratios for workforce planning: evidence on nine allied health professions. Human Resources for Health 10:2.
- Corner E, Wooda H, Englebretsena C, Thomas A, Grant RL, Nikoletouc D, Soni N (2012) The Chelsea Critical Care Physical Assessment Tool (CPAx): validation of an innovative new to measure physical morbidity in the general adult critical care population; an observational proof-of-concept pilot study. Physiotherapy.
- Escalaon NIX, Herrera J (2020) Adapting to the coronavirus disease 2019 pandemic in New York City. American J Physical Medicine and Rehabilitation, 453-8.
- Gosselink R, Bott J, Johnson M, Dean E, Nava S, et al. Physiotherapy for adult patients with critical illness: recommendations for the European Respiratory Society and the European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically ill Patients. Intensive Care Medicine 34: 1188-99.
- Green M, Marzano V, Leditschke A, Mitchell I, Bissett B (2016) Mobilisation of intensive care patients: a multidisciplinary practical guide for clinicians. J Multidisciplinary Healthcare 9: 247-56.
- Hanekom S, Gosselink R, Dean E, van Aswegen H, Roos R, et al. (2011) Ihe development of a clinical management algorithm for early physical activity and mobilisation of critically ill patients: synthesis of evidence and expert opinion and its translation into practise. Clinical Rehabilitation 1-17.
- Mudge A, Laracy S, Richter K, Denaro C (2016) Controlled trial of multidisciplinary care teams for acutely ill medical inpatients: enhanced multidisciplinary care. Internal Med J 36: 558-63
- National Quality Board /Chief Nursing Officer (2013) How to ensure the right people, with the right skills, are in the right place at the right time.
- NHS England and NHS Improvement (2019) Job planning the clinical workforce — allied health professionals, a best practice guide , NHS Improvement publication code: SL 20/19.
- Ntoumenopoulos G (2015) Rehabilitation during mechanical ventilation: Review of the recent literature. Intensive and Critical Care Nursing, 31: 125-32.
- Ridoutt L, Schoo A, Santos T Workload Capacity Measures for Use in Allied Health Workforce Planning - Final Report. Human Capital Alliance, I)epartment of Human Services Victoria.
- Rich J, Coman M, Sharkey A, Church D, Pawson J, et al. (2021) A single center observational study of the incidence, frequency and timing of critical care physiotherapy intervention during the COVID- 19 pandemic. J the Intensive Care Society
- Royal College of Physicians (2018) Guidance on Safe Medical Staffing: Report of a working group.
- Sommers J, Engelbert RHH, Dettling-lhnenfeldt D, Gosslink R, Spronk PE. et al. (2015) Physiotherapy in the intensive care unit: an evidence-based, expert driven, practical statement and rehabilitation recommendations. Clinical Rehabilitation. 29•. 1051-63.
- Schweickert WD, Pohlman MC, Nigos C, Pawlik AJ, Esbrook CL, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial Lancet 373 : 1874-82.
- Shipp Peter J (1998) Workload Indicators of Staffing Need (WISN): A Manual for Implementation v. 2. World Health Organization, Division of Human Resources Development and Capacity Building, Geneva.
- The Faculty of Intensive Care Medicine, Intensive Care Society (2019) Guidelines for the Provision of Intensive Care Services. 2nd edition
- Twose P, Jones U, Cornell G (2019) Minimum standards of clinical practice for physiotherapists working in critical care settings in the United Kingdom: A modified Delphi technique. Journal of the Intensive Care Society 20: 11 8-31.
- Valentin A, Ferdinande P (2011) ESICM Working Group on Quality Improvement. Recommendations on basic requirements for intensive care units: structural and organizational aspects. Intensive Care Medicine 37: 1575-87.
- Van Willigen Z, Collings N, Richardson D, Cusack R (2016) Quality improvement: The delivery of true early mobilisation in an intensive care unit. BMJ Quality Improvement Reports 5: 11211734.w4726.
Article Information
Research Article
Received Date: January 19.2022
Accepted Date: February 19, 2022
Published Date: February 22.2022
Critical Care Physiotherapy and Rehabilitation During the Second Wave of the COVID-19 Pandemic, A Single Centre Observational Study. Part I: Physiotherapy Interventions and Functional Outcomes
Volume 1 | Issue 1
Citation
Mark Coman (2022) Critical Care Physiotherapy and Rehabilitation During the Second Wave of the COVID-19 Pandemic, A Single Centre Observational Study. Part I: Physiotherapy Interventions and Functional Outcomes. J Phys Rehabil Physiotherapy l: 1-10
Copyright
©2025 Mark Coman. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jprp.2022.1.102