

Research Article
Volume-2 Issue-1, 2022
Women’s Perception of the Accessibility of Safe Abortion Care Services at Selected Public Institutions in Addis Ababa, Ethiopia
Received Date: January 26, 2022
Accepted Date: February 26, 2022
Published Date: February 28, 2022
Journal Information
Abstract
Background: Ethiopia ratified its abortion law in 2005, primarily to reduce the incidence of unsafe abortion and the availability of safe abortion services has increased. However, service availability has not led to a significant reduction in unsafe abortion.
Aims: This study aimed to assess women’s perception about the accessibility of safe abortion care services at selected public institutions in Addis Ababa, Ethiopia.
Study design: Institution-based cross-sectional study was conducted.
Method: The study was conducted among 432 women of reproductive age at selected non- health sector public institutions in Addis Ababa, Ethiopia. Data were entered into Epi-data, cleaned, and exported to SPSS version 24.0 for data analysis. Data analysis involved descriptive statistics, independent-sample t-test, one-way analysis of variance (ANOVA), and linear regression. Statistical significance was set at 5%. To avoid issues associated with multicollinearity, we have checked to see if (a) the condition index was < 3, (b) that the variance inflation factors (VIF) were < 5, and (c) tolerance was > 0.2.
Results: In this study, more than half (60.2%) of the participants reported that they had pregnancy at least once. Seventy-eight respondents (18.1%) had a history of previous miscarriage. Closely half of (46.2%) of the females who had miscarriage history were treated at governmental health institutions; followed by private clinics (35.9%) and traditional methods (6.4%). Whereas, 11.5% of them did not get any abortion care service. There was a significant difference in mean scores of participants faced post-abortion complications and treated at the traditional healer, and particularly the respondents attended traditional healer makes the strongest unique contribution to explaining the perception score.
Conclusions: There is an urgent need for the government and other stakeholders to provide more awareness of the accessibility and advantage of safe abortion services in the community
Key words
Women; Safe Abortion Care; Accessibility; Ethiopia
List of abbreviations: ANOVA: one-way analysis of variance IRB: Institutional Review Board LNMP: the last normal menstrual period REC: Research Ethics Committee; VIF: variance inflation factors WHO: World Health Organization
Introduction
Background of the study
Abortion is the termination of pregnancy before fetal viability, which is conventionally taken to be less than 28 weeks from the last normal menstrual period (LNMP). If the LNMP is not known, termination of birth in which the birth weight is less than 1000gm is considered an abortion[1]. Unsafe abortion is defined by the World Health Organization (WHO) as a procedure for terminating an unplanned pregnancy, performed either by persons lacking the essential skills or in an environment that does not follow to minimal health care standards, or both [2]. Providers lacking qualifications and skills to perform induced abortion frequently perform unsafe abortions, and some abortions are self-induced. Unsafe abortion continued to be the foremost cause of maternal mortality and morbidity in Africa, including Ethiopia [3]. The WHO [4] estimates that an annual 22 million unsafe abortions occur globally, almost all of which take place in developing countries and account for 13% of all maternal deaths [3]. Complications from unsafe abortion result in maternal deaths and abortion-related morbidities worldwide, placing high strain on limited health system resources and leading to severe physical, psychological, and financial consequences for women [5].
There is one in 27 women mortality from complications of gestation or delivery [6, 7], which is fifth highest in the world [8] and the maternal mortality ratio, projected to be 412 per 100,000 live births, is still enormously high in Ethiopia [9]. In Ethiopia, 32% of all maternal death is due to unsafe abortion [1]. Besides, unsafe abortion accounts for nearly 60% of all gynaecologic admissions and almost 30% of all obstetric and gynaecologic admissions in the country [1, 10].
Evidence shows that induced abortions are more likely in countries in which abortion is illegal or restricted compared to those liberated [11]. Mortality and disability from unsafe abortion can be prohibited in three ways: by preventing unplanned pregnancy, managing the complications of females who pursue post-abortion care, or administering a safe, legal substitute to unsafe abortion [7].
Cognizant of the extent of the problem of unsafe abortion, and with due recognition of the need for an integrated approach to reducing maternal morbidity and mortality, Ethiopia liberalized its abortion law in 2005 and consequently authorized midlevel health care providers to offer abortion services [1]. In most political systems, the enactment of law alone is however no guarantee of its implementation [12].
This has been true for abortion laws in particular, because internationally legal liberalization has not reliably led to increased access to services, particularly in more traditional settings where abortion is prohibited on religious grounds [13, 14].
While legal reform took place in Ethiopia ten years ago, social standards about abortion are just beginning to change, and the rise of safe abortion services has progressed steadily [7]. As studies, recommended legal modifications are inadequate to eliminate unsafe abortion. Scholars and policymakers have stressed the need to decrease abortion stigma, educate nations of their rights, and address inequities in abortion accessibility [1, 15].
Access to and provision of correct information about safe abortion care is a key determinant on the pathway to safe abortion. The absence of accurate knowledge and the fear of violating law creates a chilling effect and deter women from seeking health care services [2, 16]. Women’s knowledge of the law is only one factor in their being able to access appropriate care. Knowledge of accessible safe abortion services, providing women with information on the legal context, and methods to allow access to such information assist in decreasing the chances that a woman will seek unsafe abortion services and consequently decreasing her likelihood of suffering from abortion-related morbidity or mortality [16]. Therefore, it is imperative to understand women’s perception and knowledge about the accessibility of safe abortion care services.
Unsafe abortion is a major contributor to maternal deaths (32%) in Ethiopia [1, 17]; young and poor women suffer most from unsafe abortion, but all subgroups of women are also at risk [17]. Increasing access to safe abortion services is the most effective way of preventing the burden of unsafe abortion, which is achieved by increasing safe choices for pregnancy termination [18].
Although Ethiopia liberalized its abortion law in 2005, service availability has not led to a significant reduction in unsafe abortion [7]. Besides to legal and policy contributions, several interventions to surge the accessibility of safe abortion services have been implemented in Ethiopia [1, 19]. For instance, there has been a swift expansion of health facilities to provide qualified a legal abortion services in Ethiopia since 2008. Comprehensive abortion services also increased from 20% of the recommended level in 2008 to 38% in 2014 [19]. Disappointingly, the strategy and service delivery interferences have not led to a substantial drop in unsafe abortion [7] or related maternal mortality and morbidity in Ethiopia predominantly as a consequence of inadequate access to and utilization of safe abortion services. The Ethiopian ministry of health has also recognized that the revision of legal policies alone might not in itself ensure the accessibility of the service if other factors were not addressed as well [1]. Available safe abortion services are underutilized due to numerous factors, such as lack of awareness of the lawfulness of abortion, undesirable attitude of the providers, limited understanding on the effects of unsafe abortion and deficiency of information on the accessibility of safe providers and methods [20, 21]. Ensuring that all women know that safe abortion is available and legal for many indications will further reduce morbidity from unsafe abortions [7].
While there are few previous studies on safe abortion in Ethiopia and elsewhere in the world [22], there seems to be a gap in women’s knowledge of and perceptions on accessing safe abortion services [16]. Therefore, this study aimed to contribute to filling this critical gap and focus on women’s perception and knowledge about the accessibility of safe abortion care services at selected public institutions in Addis Ababa, Ethiopia.
Objectives
General Objective:The objective of this study is to assess women’s perception of the accessibility of safe abortion care services at selected public institutions in Addis Ababa, Ethiopia.
Specific objectives:Assess the women’s perception about the accessibility of safe abortion care service.
Determine factors associated with women’s perception of the accessibility of safe abortion care services.
Material and Methods
Study areaThis study was conducted at selected non- health sector public institutions in Addis Ababa, Ethiopia, the capital city of Ethiopia. The city is subdivided into 10 sub-cities the second administrative layer of the city and 116 districts. [23]. Based on Proclamation No 35/2012, the city has 14 Bureaus and 38 executive organs, and higher education institutions re-established being legal persons [24]. From these 9 are health-related offices or institutions. There are 6 public hospitals and 53 health centers run by the Addis Ababa City Government [23].
Study design and periodAn institutional-based cross-sectional research method was conducted from April 1 to June 30, 2019.
Source of populationWomen of reproductive age (18-49 years) residing in Addis Ababa were the source population for this study.
Study populationAll reproductive age women who work in non-health related public institutions were study population of this study
Inclusion and exclusion criteria Inclusion criteria:Women with the following characteristics were included in this study:
- Reproductive age (18-49 years)
- Working in one of the selected public institutions of the Addis Ababa City Administration
Being on annual or sick leave during the data collection time
Sample size determinationThe sample size for this study has been calculated using an online calculator for women by using a 95% confidence limit, 80% power, and 0.2 effect size. We have used 10,000-population variance for women’s groups. Accordingly, the sample size required for the women’s group was 393. The final sample size was 432 for women after including a 10% non-response rate.
Sample size determinationSince it was impossible to obtain the list of reproductive age women, one-stage cluster sampling of the institutions was used to enroll the required samples in this study. Accordingly, 30% of the Bureaus or institutions in the Addis Ababa City Government were selected using a simple random sampling method. This resulted in a cluster of 13 non-health institutions. Finally, using a proportional allocation to the size approach 432 reproductive-age women were selected from the 13 non-health institutions.
Data Collection procedures and methodsData were collected using a structured questionnaire adapted from other studies [25] to assess women’s perception of the accessibility of safe abortion care services. The questionnaire consisted of 6 socio-demographic items for women, 11 reproductive health characteristics items for women, and 10 Likert scale type items to assess women’s perception of the accessibility of safe abortion care. The questionnaire was translated from English to Amharic by a bilingual expert and back translated to English by another bilingual expert to ensure meaning equivalence between the two language versions. The Amharic version questionnaire was pretested on 5% of the study sample in institutions not selected for the parent study prior to the actual data collection. Four data collectors and two supervisors (voluntary health professionals) were recruited from outside selected public institutions.
Operational definitionsAccessibility: Within health care, access is always, defined as access to a service, a provider, or an institution, and thus defined as the opportunity or ease with which consumers or communities can use appropriate services in proportion to their needs [26]. In our study, a skilled provider at an affordable price defines accessibility as the opportunity for women of reproductive age to reach and obtain appropriate safe abortion care services within an easy-to-reach distance, at the health facility.
Perceived accessibility of safe abortion care: The Oxford Advanced Learner’s Dictionary (2010:1132) defines ‘perception’ as a particular attitude towards something or viewpoint. In this study perceived accessibility of safe abortion care is defined as the woman’s expressed satisfaction and attitude concerning the convenience of care, its coordination and cost, providers’ courtesy, information obtained, and quality of care. Perceived accessibility of safe abortion care was measured by a 10-item Likert scale with 5 response options. The response options involve ‘Strongly Disagree = 1, Disagree = 2, Neutral = 3, Agree = 4, and Strongly Agree = 5.’ The total score was computed for each respondent and it ranges from 10 – 50. A higher score indicates a more favorable perception.
Data processing and analysis proceduresAfter data collection, complete questionnaires were coded, checked, cleaned, and entered into Epi data software and imported to SPSS software version 24.0 for analysis. Data analysis involved descriptive statistics, including frequency, percentage, mean and standard deviations. Bivariate analysis using correlation coefficients, independent-sample t-test, and one-way analysis of variance (ANOVA) was conducted to assess factors associated with knowledge and perception about the accessibility of safe abortion care. Statistical significance was set at 5%. Multiple linear regression analysis was used to identify variables independently predicting knowledge and perception about the accessibility of safe abortion care. Multi-categorical independent variables were dummy coded before entering into the models. To avoid issues associated with multicollinearity, we have checked to see if (a) the condition index was < 3, (b) that the variance inflation factors (VIF) were < 5, and (c) tolerance was > 0.2.
Data quality controlTo maintain data quality, all data collectors were health professionals and all of them were trained on data collection procedures by the principal investigator and co-investigators. Moreover, the data collection instrument and procedures were pretested on 5% of the study sample in the institutions not selected for the parent study to evaluate the accuracy of responses, language clarity, appropriateness of data collection tools, and to estimate the time required; the necessary amendments were considered.
Ethical considerationEthical approval was obtained from the Institutional Review Board (IRB) of the College of Health Sciences at Addis Ababa University. A letter of permission was obtained from the Addis Ababa Health Bureau, which also provided us a letter of cooperation written to all selected public institutions. Following an explanation of the purpose of the study informed consent was obtained from those who met the inclusion criteria and agreed to participate. In addition, information regarding their unconditional right to withdraw consent and discontinue participation without any form of prejudices was provided. Confidentiality of information and privacy of participants has been maintained for all the information provided, to preserve the confidentiality the data have been kept in a locked cupboard and not accessible by any other person except the principal and co- investigators.
Patient and Public InvolvementPatients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Socio-demographic characteristicsFour hundred thirty-two (432) women participated in this study with a 100.0% response rate. More than half (55.8%) of the respondents were married and the majority (81.5%) of them were orthodox Christian. The age of study participants ranged from 18 to 48 years, with a mean age of 29.51. The distribution by the biosocial characteristic of the respondents is shown in Table 1.
Reproductive health characteristics and exposure to abortion informationIn this study, more than half 260(60.2%) of the participants reported that they had at least one pregnancy; among which majority were primigravid 102(39.2%) (Figure 1). Seventy-eight (18.1%) respondents had a history of a previous miscarriage, among these, the majority (74.4%) happened due to spontaneous abortion.
Among the respondents studied, 283 (65.5%) of them had heard of abortion care and media was the major source of information (79.5%), while peers, books, internet, and others accounted for 23%, 21.6%, 9.9%, and 1.8% respectively. Regarding abortion care provision for women who had a history of miscarriage, nearly half of them (46.2%) were treated at governmental health institutions; followed by private clinics (35.9%) and traditional methods (6.4%). Moreover, 11.5% of them did not get any abortion care service.
Concerning complications after the abortion, the majority of the participants (74.4%) did not face any complications. Among the 20(25.6%) women who suffered a post-abortion complication, the majority 15(75%) of the participants mentioned that they encountered hemorrhage (Figure 2).
Factors affecting women’s perceptions towards abortion care service provisionTable 2 shows an independent-sample t-test conducted to compare the perception scores among dichotomous independent variables. There was significant difference in scores for participants with post abortion complications (M = 52.2, SD = 6.54) versus those that did not face complications (M = 53.5, SD = 6.05; t (54) = 2.12, p = 0.39, two-tailed). In addition, there was significant difference in scores for participants treated at traditional healer (M = 62.8, SD = 3.42) and those did not (M = 54.93, SD = 6.5; t (73) = 2.7, p = 0.009, two-tailed). The magnitude of the differences in the means (mean difference = .00, 95% CI: 2.01 to 13.73) was very small. In this study, the analysis of variance (ANOVA) showed that the effect of education, marital status and religion was not significant: F (2, 423) = 1.86, p= 0.16; F (2, 429) = 1.36, p= 0.26 and F (2, 429) = 0.85, p= 0.43 respectively.
Moreover, the univariate linear regression model indicated that there are significant differences in the perception score with the participants’ level of knowledge. The size of the estimated regression coefficient suggests that for one additional knowledge mark, the respondents’ perception score also increases by 0.5. The models did not show any significant differences in the score with marital status, several deliveries, or religion.
The factors influencing women’s perception of the accessibility of safe abortion care servicesBesides, multiple linear regressions were used to assess the effect of age, number of pregnancies, number of deliveries, knowledge about abortion, those attended traditional healers, place of grew up, and history of pregnancy factors to predict levels of perception. After the variance explained by all other variables in the model were controlled, the respondents those attended traditional healer makes the strongest unique contribution to explaining the perception score recording a standardized beta value of 0.328. As shown in Table 3, the knowledge on abortion and women who attended traditional healer is making a significant unique contribution to the prediction of the perception level.
Discussion
This study aimed to develop an evidence base to realize concerns related to the perception of accessibility of safe abortion services in Addis Ababa from the perspective of public servant women. We discussed findings of women’s socio-demographic characteristics, information exposure, reproductive history, place of abortion care-seeking, and perceptions. The findings have implications for the promotion of safe abortion service and the reduction of unsafe abortion that is one of the leading causes of maternal morbidity and mortality in Ethiopia.
In this study, one-fifth of the participants had a history of previous miscarriage and it has happened predominantly due to spontaneous abortion. The study is in contrast to a study done in southern Ethiopia which showed that virtually all of the abortions were induced and the reason may rely on the study population, which was among tertiary education students [27, 28]. In addition, another study done in rural southern Ethiopia revealed a high level of induced abortion, and the discrepancy was probably due to the study setting where modern family planning is less spread and as a result consequences unwanted pregnancy [29]. Furthermore, it is not in agreement with a study done in Cambodia whish shown that induced abortion was widely used [30] and the reason could be the study population as the study participants were women sex workers which might rise chance of the unwanted pregnancy. Among the respondents studied, two-third of the women had heard of safe abortion care and the media was the major source of information. This is in agreement with a study done in South Africa which indicated that radio and television as their main source of information and little has been done to promote safe abortion service through health care providers and other means of communication [31]. In contrast, a study conducted in India showed that the respondents had limited exposure to mass media [32].
Although access to basic abortion care services in Ethiopia exceeded the recommended level of facilities providing the service [33], the current study showed that about 46.2% of the women stated that they attended governmental health institutions to get abortion care service; while the others went to private clinics (35.9%), traditional procedures (6.4%), and 11.5% of them didn’t get any abortion care service. This is in parallel with the studies done in Kenya which showed that abortion services outside public health facilities were mentioned frequently [34, 35]. Probably the reasons are the need for confidentiality to escape condemnation, hesitation about the law, and perceived expensive safer abortion services.
WHO reported that abortions performed by qualified persons using correct techniques and sanitary conditions are safe and seldom presents complications [36]. In the present study, when asked about complications after abortion, three-fourths of the women reported that they did not face any complications. This could be a result of a large number of respondents who reported spontaneous abortion, which proceeds rare fatality and infrequently acquires complications. However, the study revealed that hemorrhage was the commonly reported type among the women who suffered post- abortion complications.
After the variance explained by all other variables in the model was controlled, the respondents those attended unhygienic procedure make the strongest unique contribution to explaining the perception score. Moreover, the knowledge of abortion made a significant unique contribution to the prediction of the perception level. This is in line with the study conducted in Ihar and Jharkhand, India [32]. Dissimilarity, the study conducted in western Kenya indicated that the health care provider, the social, economic, and cultural norms influenced the perception of women’s access to safe abortion services [34].
Conclusions
The Ethiopian federal ministry of health declared and implemented policies and guidelines about access to womencentred services that are provided by trained and competent professionals with up-to-date technologies and that are easyto-reach, inexpensive, and unbiased over the past decade to reduce the magnitude of unsafe abortion complications and deaths. However, this study indicated that a significant number of women still unheard about accessibility of the safe abortion care and attending the untrained personnel services and risky procedure of care. There is an urgent need for the government and other stakeholders to provide more awareness of the accessibility and advantage of safe abortion services in the community
Strengths and limitations of this study StrengthThe instrument was pretested and modified before actual data collection.
This study is the first to assess women’s knowledge about the accessibility of safe abortion care services at non-health sector public institutions in Addis Ababa, Ethiopia.
Limitations
- The information obtained from women could be subject to recall bias.
- The study as being cross-sectional, it did not tell us about the cause and effect relationship between various factor and perception score.
References
- FMOH: Technical and Procedural Guidelines for Safe Abortion Services in Ethiopia. Addis Ababa: Federal Ministry of Health Ethiopia. In.; 2006.
- Musembi J: Determinants of Adherence to Cotrimoxazole Preventive Therapy among HIV Infected Persons on Treatment in Machakos District Hospital, Machakos County, Kenya. 2014.
- WHO: Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2003. Geneva: World Health Organisation; In.; 2007.
- Organization WH: Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008, 3rd edition. Geneva: (http://www.who.int/reproductive health/publications/unsafe_abortion/9789241501118/en,(accessed June 20,2017) In.; 2011.
- Assefa Y, Kiflie A, Tesfaye D, Mariam DH, Kloos H, Edwin W, Laga M, Van Damme W: Outcomes of antiretroviral treatment program in Ethiopia: retention of patients in care is a major challenge and varies across health facilities. BMC health services research 2011, 11(1):81-81.
- Population Reference Bureau (PRB), 2008 World Population Data Sheet,Washington, DC: PRB, . In.; 2008.
- Gebreselassie H, Fetters T, Signh S, Abdella A, Gebrehiwot Y, Tesfaye S, Geressu T, Kumbi S: Caring for women for abortion complications in Ethiopia: National estimates and future implications. International Perspective of Sexual and Reproductive Health 2010, 36(1):6-15.
- WHO, Maternal Mortality in 2005: Estimates Developed by WHO, UNICEF, UNFPA and theWorld Bank, Geneva: WHO, . 2005.
- Ethiopian Central Statistical Agency and ORC Macro, Ethiopia Demographic and Health Survey: Key Indicators 2016, Addis Ababa, Ethiopia: Central Statistical Agency; and Calverton, MD, USA: ORC Macro, . In.; 2016.
- Singh S: Hospital admissions resulting from unsafe abortion: estimates from 13 developing countries. . Lancet 2006, 368(9550):1887-1892.
- Sedgh G, Singh S, Shah I, Ahman E, Henshaw S, Bankole A: Induced abortion: incidence and trends worldwide from 1995 to 2008. Lancet. . 2012, 379(9816):625-632.
- Patashnik E: “After the public interest prevails: The political sustainability of policy reform,” Governance 2003, 16(2):203- 234.
- Benson, Janie, Kathryn A, Ghazaleh S: Reductions in abortion-related mortality following policy reform: Evidence from Romania, South Africa and Bangladesh. Reproductive Health 2011, 8(39):1-12.
- Singh, Susheela, Gilda S, Akinrinola B, Rubina H, London S: Making abortion services accessible in the wake of legal reforms: A framework and six case studies. New York: Guttmacher Institute. www. guttmacher.org/pubs/abortion-services-laws.pdf. In: Guttmacher Institute. 2012.
- Gebresilase H, Fetters T, Singh S, Abdella A, Gebrehiwot Y, Tesfay S, Geresu TK, S. : Caring for women with abortion complications in Ethiopia: national estimates and future implications. Guttmacher Institute 2008.
- Assifi A, Berger B, Tunçalp, Khosla O, Ganatra B: Women’s Awareness and Knowledge of Abortion Laws: A Systematic Review. PLOS one 2016, 11(3).
- Singh S, Wulf D, Hussain R, Bankole A, Sedgh G: Abortion Worldwide: A Decade of Uneven Progress. Yew York. Guttmacher Institute. In.; 2009.
- Woldetsadik M, Sendekie TY, White MT, Zegeye DT: Client preferences and acceptability for medical abortion and MVA as early pregnancy termination method in northwest Ethiopia. Reprod Health 2011, 8:19.
- Dibaba Y, Dijkerman S, Fetters T, Moore A, Gebreselassie H, Gebrehiwot Y, Benson J: A decade of progress providing safe abortion services in Ethiopia: results of national assessments in 2008 and 2014. DOI 10.1186/s12884-017-1266-z. Pregnancy & Childbirth 2014, 17(76).
- Banerjee SK, Andersen KL, Buchanan RM, Warvadekar J: Woman-centered research on access to safe abortion services and implications for behavioral change communication interventions: a cross-sectional study of women in Bihar and Jharkhand, India. BMC public health 2012, 12(1).
- Ganatra B, Banerjee SK: Expanding Community-Based Access to Medical Abortion in Jharkhaand: a Pre-intervention Baseline Survey in Selected Two Blocks of Ranchi and Khunti districts New Delhi:. Ipas India 2010.
- Loi UR, Gemzell-Danielsson K, Faxelid E, Klingberg-Allvin M: Health care providers' perceptions of and attitudes towards induced abortions in sub-Saharan Africa and Southeast Asia: a systematic literature review of qualitative and quantitative data. BMC Public Health 2015, 15.
- City_Government_of_Addis_Ababa: Socio-economic profile of Addis Ababa for the year 2004 E.C./2011/12 G.C. In. Addis Ababa: Policy Study and Analysis Sub Process; 2013.
- Dameksa K: "Addis Ababa City Government Executive and Municipal Service Organs Re- establisment Proclamation N 35/2012". In.: Addis Negarit Gazeta No 35; 2012.
- Low WY, Tong WT, Gunasegaran V: Issues of safe abortions in Malaysia : reproductive rights and choice. In: Malaysia University. 2013.
- Daniels N: Equity of Access to health care: some conceptual and ethical issues. Milbank Mem Fund Q 1982, 60:51-81.
- Gelaye AA, Taye KN, Mekonen T: Magnitude and risk factors of abortion among regular female students in Wolaita Sodo University, Ethiopia. BMC women's health 2014, 14(1):50.
- Mitiku1 S, PMD, FB, Mengistu Meskele4, 1. Healing hands of joy HE: Prevalence of Induced Abortion and Associated Factors among Wachamo University Regular Female Students, Southern Ethiopia. 2015.
- Gezahegn Tesfaye MTH, 1 Agumasie Semahegn2: Induced Abortion and Associated Factors in Health Facilities of Guraghe Zone, Southern Ethiopia. 2014.
- Delvaux T, Crabbe F, Seng S, Laga M: The need for family planning and safe abortion services among women sex workers seeking STI care in Cambodia. Reproductive health matters 2003, 11(21):88-95.
- Varkey SJ: Abortion services in South Africa: available yet not accessible to all. International Family Planning Perspectives 2000, 26(2):87-88.
- Banerjee SK, Andersen KL, Buchanan RM, Warvadekar J: Woman-centered research on access to safe abortion services and implications for behavioral change communication interventions: a cross-sectional study of women in Bihar and Jharkhand, India. BMC public health 2012, 12(1):175.
- Dibaba Y, Dijkerman S, Fetters T, Moore A, Gebreselassie H, Gebrehiwot Y, Benson J: A decade of progress providing safe abortion services in Ethiopia: results of national assessments in 2008 and 2014. BMC pregnancy and childbirth 2017, 17(1):76.
- Marlow HM, Wamugi S, Yegon E, Fetters T, Wanaswa L, Msipa-Ndebele S: Women’s perceptions about abortion in their communities: perspectives from western Kenya. Reproductive Health Matters 2014, 22(43):149-158.
- Jayaweera RT, * FMN, KSH, CG: Women's experiences with unplanned pregnancy and abortion in Kenya: A qualitative study. 2017.
- Unsafe abortion: global and regional estimates of incidence of unsafe abortion and associated mortality in 2003
Variable |
Number |
Percent |
Mean age(Range; SD) |
29.51(18-48;5.4) |
|
Marital status Single Married Others* |
163 |
37.7 |
Educational status |
85 |
20.0 |
Religion |
352 |
81.5 |
Place grew up UrbanRural |
345 |
79.9 |
*widowed and divorced ** Muslim, Catholic. |
|
|
Variable |
|
N % |
t |
P value |
Place of grew up |
Urban |
79.9 |
1.71 |
0.089 |
|
Rural |
20.1 |
|
|
History of Pregnancy |
Yes |
60.2 |
0.96 |
0.34 |
|
No |
39.8 |
|
|
Treated at a traditional healer |
Yes |
1.2 |
2.68 |
0.009 |
|
No |
98.8 |
|
|
Abortion awareness |
Yes |
65.5 |
0.9 |
0.37 |
|
No |
34.5 |
|
|
History of Abortion complications |
Yes |
4.62 |
2.12 |
0.039 |
No |
95.38 |
|
|
Variable |
Beta (standard) |
P |
Confidence interval |
Collinearity statistics |
||
|
|
|
Lower |
Upper |
Tolerance |
VIF |
Age |
-0.104 |
0.474 |
-0.442 |
0.208 |
0.616 |
1.622 |
Number of pregnancies |
0.137 |
0.544 |
-1.711 |
3.219 |
0.254 |
3.941 |
Number of deliveries |
-0.004 |
0.986 |
-2.887 |
2.837 |
0.276 |
3.621 |
Knowledge about abortion |
0.233 |
0.049 |
0.002 |
0.995 |
0.948 |
1.055 |
Attended traditional healer |
-0.328 |
0.007 |
-13.609 |
-2.187 |
0.911 |
1.098 |
Place grew up |
0.114 |
0.333 |
-1.803 |
5.242 |
0.936 |
1.068 |
Pregnancy history |
0.042 |
0.740 |
-2.615 |
3.660 |
0.792 |
1.262 |
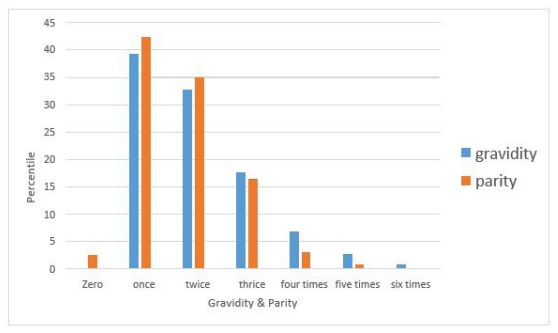 |
| Figure 1: Status of gravidity and parity of women at selected public institutions in Addis Ababa, Ethiopia 2019 |
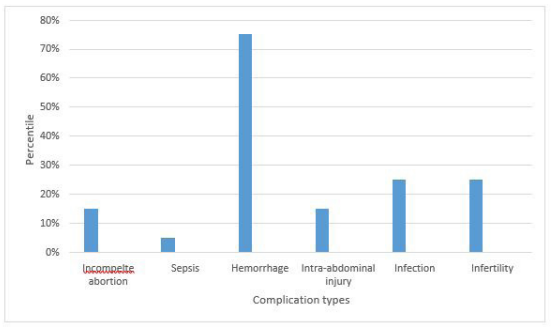 |
| Figure 2: Abortion complication types faced by women at selected public institutions in Addis Ababa, Ethiopia 2019 |
Artcle Information
Research Article
Received Date: January 26, 2022
Accepted Date: February 26, 2022
Published Date: February 28, 2022
Journal of Women Health Care and Reproductive Medicine
Volume 2 | Issue 1
Citation
Sendo Endalew G (2022) Women’s Perception of the Accessibility of Safe Abortion Care Services at Selected Public Institutions in Addis Ababa, Ethiopia. J Women Health Care Reprod Med 2: 1-12
Copyright
©2022 Negalign Getahun Dinegd. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jwrm.2022.2.102-(1)