

Review Article
Volume-1 Issue-1, 2025
Evolution of Early Marriage and Adolescent Childbearing by Social Determinants of Health in Morocco
Received Date: March 01, 2025
Accepted Date: March 19, 2025
Published Date: March 26, 2025
Journal Information
Abstract
Objectives: Early marriage and adolescent childbearing constitute a crucial problem in Morocco. The aim of this paper is to describe and analyse the evolution of this phenomenon during the last three decades, according to social determinants of health like milieu (rural-urban), education level and wealth quintiles.
Material and Methods:Inequity in terms of early marriage and adolescent pregnancy/motherhood in Morocco was analysed using disaggregated data given by Demographic Health Surveys (DHS) and the Pan Arab Project for Family Health (PAPFAM) surveys. Beside using absolute values (gaps) and relative values (ratios) for comparison, the index of dissimilarity (ID) was used to compare the distribution of early marriage and adolescent childbearing by milieu of residence, education level and wealth quintile.
Results: Data analysis indicates that early marriage and adolescent childbearing affect more rural girls than urban ones. No educated girls are much more likely to be early married and to begin childbearing than their counterparts with secondary level of education. Poor adolescents are twice more exposed to early marriage than rich adolescents. The inequitable distribution of early marriage and adolescent childbearing is confirmed by high values of the index of dissimilarity for each social determinant.
Conclusion: According to different social determinants, sensible variations are seen in terms of early marriage and adolescent pregnancy/motherhood by milieu of residence, education level and wealth quintiles in Morocco. This is a clear appeal to decision makers to end or at least to reduce child marriage and pregnancy by acting on social determinants of health, targeting first disadvantaged girls living in rural remote areas and suffering from multiple vulnerabilities (poverty, illiteracy, school dropping, social exclusion, violence and others).
Key words
Early Marriage; Adolescent Pregnancy; Motherhood; Social Determinants; Iniquity; Milieu; Education; Wealth
Survey’s name & date Sample size |
DHS 2003-04 |
PAPFAM 2011 |
PAPFAM 2018 |
Households surveyed Urban Total |
6416 5097 11513 |
9458 5885 15343 |
8788 6234 15022 |
Individual women surveyed Urban Total |
8997 7801 16798 |
6357 4712 11069 |
5528 4441 9969 |
Survey’s name & date |
2011 |
PAPFAM 2018 |
Milieu of residence Urban |
15.6% |
12.9% |
Education level Without certificate Fundamental |
24.7% |
22.8% |
Wealth quintile Poorest quintile (Q1) Second quintile (Q2) Third quintile (Q3) Fourth quintile (Q4) Richest quintile (Q5) |
23.2% |
21.2% |
Survey |
DHS 2003-04 |
PAPFAM 2011 |
PAPFAM 2018 |
Milieu of residence Urban |
9.9% |
8.6% |
8.2% |
Education level Without certificate Fundamental |
14.6% |
12.5% |
15.2% |
Wealth quintile Poorest quintile (Q1) Second quintile (Q2) Third quintile (Q3) Fourth quintile (Q4) |
9.2% |
8.7% |
Not available |
 |
| Figure 1: Perinatal mortality in Morocco, 2018 |
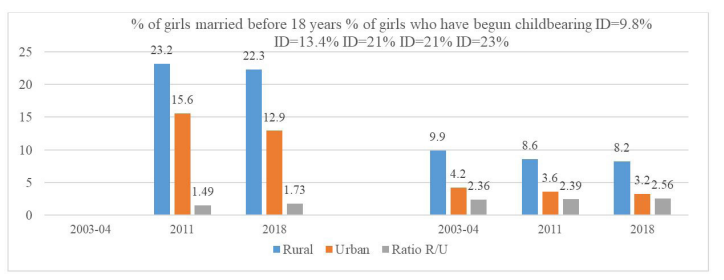 |
| Figure 2:Evolution of the % of Moroccan adolescent girls married before age 18 years and % of adolescents who have begun childbearing by milieu of residence |
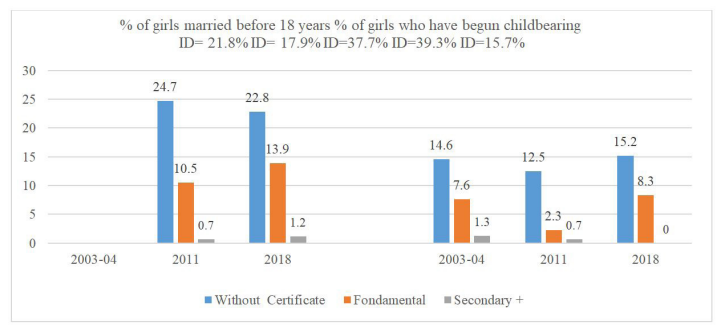 |
| Figure 3: Evolution of the % of Moroccan adolescent girls married before age 18 years and % of adolescent girls who have begun childbearing by level of education |
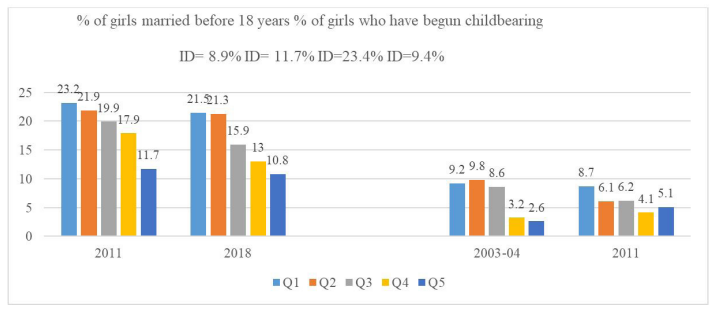 |
| Figure 4: Evolution of the % of Moroccan adolescent girls married before age 18 years and % of adolescent girls who have begun childbearing by wealth quintiles |
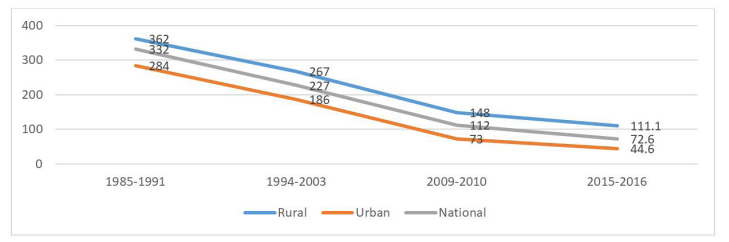 |
| Figure 5: Evolution of MMR in rural and urban zones in Morocco during the last 3 decades |
 |
| Figure 6: Early marriage under the effect of cumulative deprivations, 2021 |
Introduction
As defined by UNICEF, “child marriage refers to any formal marriage or informal union between a child under the age of 18 and an adult or another child” [1].
The Convention on the Rights of the Child recalls the need to reinforce and extend the rights of the Child stated by previous declarations and conventions [2], including: Geneva Declaration of the Rights of the Child (1924) [3], Declaration of the Rights of the Child adopted by the General Assembly on 20 November 1959 [4] and International Covenant on Civil and Political Rights (1966) [5].
Considering that the child should be fully prepared to live an individual life in society, and brought up in the spirit of the ideals proclaimed in the Charter of the United Nations, and in particular in the spirit of peace, dignity, tolerance, freedom, equality and solidarity, the Convention on the Rights of the Child defines the age limit of a child in Article 1:“For the purposes of the present Convention, a child means every human being below the age of eighteen years unless under the law applicable to the child, majority is attained earlier” [2].
Early marriage and teenage pregnancy/motherhood is a silent phenomenon crucially affecting the rights of the Child in many low and middle income countries around the world. As stressed by the World Health Organization, “first pregnancy at an early age is risky. Although births among adolescents account for 11% of all births worldwide, they account for 23% of the overall burden of disease (in terms of disability-adjusted life years)” [6].
In Morocco, the family code (Moudawana) which was adopted in 2004, fixed the minimal age of marriage at 18 years for both girls and boys. However, judges may “exceptionally” allow girls and boys to be married at an earlier age [7]. Consequently, the Ministry of Justice registered 38710 (with 87% accepted) and 39249 (with 83% accepted) early marriage proposals in 2007 and 2017 respectively of which 99% concerning girls [8].
Beyond affecting seriously health indicators like maternal and infant mortality, early marriage is a violation of human rights seriously hindering healthy life and wellbeing of adolescent girls at (1) An individual level (Physical, mental, reproductive health, exposition to physical/ psychological/sexual violence, school dropout, exclusion from training programs and infringement of individual freedom), (2) Socioeconomic level (social exclusion, precarious economic situation, gender inequality, divorce and family problems, underdevelopment in terms of health, education and social life, general lack of women empowerment)[8].
A recent study conducted by the Public Ministry stressed that the phenomenon of early marriage in Morocco is a complex problem generated by poverty and difficult social conditions, school dropout and few years of education, violence and family instability and other [9]. The conclusion of this study shed light on the need to act on social determinants of health to end child marriage in Morocco.
As stressed by the WHO Commission on Social Determinants of Health (CSDH) in its report released in 2008, social determinants of health are defined as the conditions in which people are born, grow, live, work and age. Social determinants of health are seen to be responsible for unfair and avoidable health inequities within and between countries [10,11]. In its report published in 2021, the Commission on Social Determinants of Health in the Eastern Mediterranean Region (CSDH-EMR) stressed the urgent necessity for WHO Eastern Mediterranean countries to reduce health inequities by acting on social determinants of health [12]. However, reducing inequalities in early marriage and adolescent pregnancy/motherhood by acting on social determinants of health was given very little consideration in the report of the WHO Eastern Mediterranean Region Commission.
Material and Methods
In this paper, we use available disaggregated (secondary) data to describe and analyse the evolution of early marriage and teenage pregnancy/motherhood in Morocco under the effect of the following social determinants of health: milieu of residence (rural-urban), level of education and wealth quintiles.
Evolution of early marriage and adolescent childbearing in Morocco is considered through data provided by Demographic Health Surveys (DHS 2003-04) [13] and the Pan Arab Project for Family Health surveys (PAPFAM 2011 and PAPFAM 2018) [14,15]. Sampling techniques are those used in household surveys by Demographic Health Surveys. For each survey, the number of households surveyed and the number of women surveyed individually in urban and rural areas are given in Table 1.
Beside absolute differences (gaps) and relative differences
(ratios), the index of dissimilarity (ID) is used to compare the
distributions by milieu of residence, education level and wealth
quintile at each period. This index is a commonly used method
of measuring inequality between two populations according
to geographic, demographic and socio-economic factors. It
compares how evenly one population sub-group A is spread
out compared to another population sub-group B. The ID is
computed using the formula ID = .
.
Where A is the sub-group A population and ai represents the subgroup A population in category i, and similarly, B is the sub-group B population and bi is the sub-group A population in category i.
The index of dissimilarity has a value between 0 and 1 (also given as a percentage between 0% and 100%). A value of ID near zero means that the distribution between the two groups shows no (or little) difference while a value of ID approaching 1 indicates an inequitable distribution between the two groups.
Results
The persisting problem of early marriage and teenage pregnancy/ motherhood constitutes a real challenge for health decision makers in Morocco [8]. For instance, in 20018, the numbers of stillbirths and early neonatal deaths as well as the perinatal mortality rate were much higher in Group 1 of young married women aged less than 20 years than among married women of Group 2 (aged 20-29) or Group 3 (30-39 years) (Figure 1).
Data source:PAPFAM survey Morocco 2018./p>
Data provided by the Pan Arab Project for Family Health surveys in Morocco (PAPFAM 2011, 2018) [14,15] indicate that the average percentage of Moroccan girls who were early married varies considerably by milieu of residence (rural-urban), level of education and wealth quintiles. Moreover, inequalities are persisting if not increasing (Table 2).
Similarly, the percentage of adolescent girls who have begun childbearing (those who have had a live birth or where pregnant at the period of the survey) also varies by socio-demographic factors as illustrated by Table 3 below.
Early marriage and adolescent pregnancy/motherhood in Morocco by milieu of residence (rural-urban)
As illustrated by Figure 2 below, the percentages of early marriage and early pregnancy/ motherhood are higher in rural areas than in urban areas. Moreover, the ratios Rural/Urban increased regularly for early marriage (from 1.49 in 2011 to 1.73 in 2018) and for early childbearing (from 2.36 in 2003-2004 to 2.56 in 2018). The iniquity distribution by milieu of residence is confirmed by the high values of the index of dissimilarity which increased from 9.8% in 2011 to 13.4% in 2018 for early marriage and from 21% in 2003-04 to 23% in 2018 for early childbearing.
Early marriage and adolescent childbearing in Morocco by education level
Early marriage and adolescent childbearing in Morocco affect clearly more girls without certificate than girls with secondary level of education. Indeed, Figure 3 shows that girls without certificate were 35 times more likely to be married before age 18 years (24.7%) than girls having a secondary level of education or plus (0.7%) in 2011. Although the difference decreased in 2018, the ratio was still 19 between the % of girls without certificate (22.8%) and the % of girls with secondary level or plus (1.2%). Consequently, the % of early pregnancy and motherhood also showed the same pattern of iniquity according to the level of education. The inequity is confirmed by the high values of the index of dissimilarity.
Early marriage and adolescent childbearing in Morocco by wealth quintiles
According to data provided by PAPFAM surveys in 2011 and 2018, the percentage of Moroccan girls who were early married is highly correlated with wealth quintiles. As illustrated by Figure 4, the ratio Q1/Q5 persisted around the same value (1.98 vs 1.99), meaning that the poorest girls are nearly twice as likely as to be early married than their counterparts from the richest quintile. However, the inequitable distribution accentuated since the index of dissimilarity increased from 8.9% in 2011 to 11.7% in 2018.
Unfortunately, the PAPFAM survey 2018 does not provide early pregnancy/motherhood by wealth quintile and consequently, comparison is only done using available data from DHS 2003- 04 and PAPFAM 2011 which shows that iniquity was reduced between 2003-04 (ID=23.4% and Ratio Q1/Q5= 3.5) and 2011 (ID=9.4% and Ratio Q1/Q5=1.7).
Discussion
Early marriage is harmful not only for girls but also for society as a whole. Indeed, when married before the age of 18, girls loose their basic rights of access to health, education, development and wellbeing. As a result, they will be more exposed to maternal mortality due high risk of complications during pregnancy or childbirth and if they survive, they will face crucial problems in the raise and development of their children.
According to UNICEF, in 2018, globally around 21% of young women were married before their 18th birthday with the highest prevalence (37%) of child marriage seen in sub-Saharan Africa [16].
In 2019, Yaya and al. published an interesting study on the prevalence of child marriage and its impact on fertility outcomes in 34 sub-Saharan African countries. The authors used secondary DHS data on 60215 women aged 20-24 years. The mean prevalence (in the 34 countries) of women who experienced child marriage was 54.0% but a large disparity was seen between countries. Indeed, the prevalence of child marriage varied from 15% to 50% in 16 countries, from 51% to 60% in 10 countries and from 61% to 82% in 8 countries. A huge gap was seen between the highest prevalence (81.7%) in Niger and lowest prevalence (16.5%) in Rwanda [17].
In the Arab region, the prevalence of child marriage is around 14% but it varies from 1% to 8% in Tunisia (1%), Algeria (2%), Libya (2%), Djibouti (5%) and Jordan (8%); from 10% to 20% in Morocco (13%), Egypt (17%), Syria (18%) and Palestine (19%); and from 20% to 45% in Yemen (32%), Sudan (33) and Somalia (45%) [18].
Consequently, Morocco has a relatively low prevalence of early marriage compared with countries in the Arab region and subSaharan Africa.
As indicated by UNFPA in its report on “Advancing the Evidence Base Strategies to End Child Marriage”, girls living in the poorest and rural communities cumulate vulnerabilities and are unlikely to be reached by interventions. Consequently, they are the most affected by early marriage and adolescent pregnancy [19].
In 2021, the UNFPA-UNICEF Global Programme to End Child Marriage carried out a scoping review of the evidence base on child marriage during two decades (2000-2019), focusing on four research topics: (1) prevalence and measurement, (2) determinants, correlates and context, (3) consequences and (4)interventions (UNFPA). Globally, the 386 publications reviewed showed an exponential increase of publications from 11 in 2000- 2003 to 107 in 2012-2015 and 193 in 2016-2019. Regionally, nearly 70% of evidence base was provided by studies in the two regions with highest prevalence rates and burden of child marriage, namely: Sub-Saharan Africa (35%) and South Asia (34%) [20]. In terms of research topics, the second topic known as “drivers” (determinants, correlates and context) was the most frequent with 181 publications, representing nearly 50% of all research topics in the publications reviewed by 2019 [20].
According to the study cited earlier [17], the prevalence of child marriage in sub-Saharan African countries shows large disparities between rural areas (45.3%) and urban zones (24.6%). A huge gap is seen between no educated women (61.7%) and women with primary level (45.4%), secondary level (18.1%) and higher education level (4.1%). Finally, prevalence of child marriage follows an exponential increase with the decrease of wealth quintiles, varying from 19.2% in the richest quintile to nearly 53% in the poorest quintile [17].
In Morocco, rural zones lag behind urban zones according to the quasi totality of health indicators [13-15,21]. For example, the maternal mortality rate (MMR) decreased significantly in both urban and rural areas during the last three decades. However, the ratio Rural/Urban increased regularly from 1.27 in 1985-91 to 2 in 2009-10 and to 2.5 in 2015-16 (Figure 5).
According to the World Health Organization, “education is a major protective factor for early pregnancy: the more years of schooling, the fewer early pregnancies” [2]. This statement is well confirmed globally and the variation of early marriage by education level in Morocco is comparable to similar variations in the Arab region and sub-Saharan Africa.
Early marriage by wealth quintiles shows also that the inequitable distribution in Morocco is comparable to that of Arab countries and sub-Saharan African countries.
In terms of adolescent childbearing, variations by milieu of residence (urban-rural), level of education and wealth quintiles in Morocco can be compared to the ones provided by data from Demographic Health Surveys in Egypt (2014) [22], Jordan (2017- 18) [23] and Yemen (2013) [24]; and data from Mixed Indicator Cluster Surveys in Iraq (2018) [25], Palestine (2014) [26], Qatar (2012) [27], Sudan (2014) [28] and Tunisia (2018) [29].
By milieu of residence, inequity in the percentage of women who had begun childbearing is more pronounced in Morocco than in Egypt, Jordan, Iraq, Palestine, Sudan, Yemen and Tunisia.
By education level, the inequity distribution in Morocco is comparable to that seen in Egypt, Palestine, Tunisia and Yemen while Jordan, Iraq, Qatar and Sudan have more accentuated iniquities.
Finally, the distribution by wealth quintile of adolescent girls who had begun childbearing in Morocco and Yemen is less inequitable than in Egypt, Jordan, Iraq, Palestine, Sudan and Tunisia.
Last but not least, it is necessary to point out the effect of cumulative deprivation on early marriage and adolescent childbearing in Morocco. Indeed, a recent study of the National Observatory on Human Development (NOHD) on ‘‘Intersectional discrimination of women in Morocco’’ analysed the accumulation of deprivations among women who have been married before the age of 18 years. In addition to the effect of each of the sociodemographic factors (milieu of residence, standard of living and region), the combined effect of two or three of these factors were considered. The result is illustrated in Figure 6 below, showing that a rural girl, belonging to the poorest quintile and living in the most disadvantaged region, has 3 deprivations and is therefore 3.5 times more exposed to early marriage (38.2%) than an urban girl, belonging to the richest quintile and living in the most advantaged region (10.9%) [30].
Conclusion
The analysis carried out in this paper shows clearly that action on social determinants of health is the best way to reduce avoidable and unfair inequalities and also to end or at least to limit the persisting intolerable phenomenon of early marriage and adolescent childbearing.
Decision makers should act on social determinants by targeting disadvantaged populations burdened by poverty, illiteracy and generally living in remote areas [31-33]. Pragmatic actions should compensate the insufficiency of theoretical conventions and laws as underlined in the introduction section. Indeed, according to the UNICEF report on child marriage in the Middle East and North Africa, ‘‘there is often a contradiction between national law and customary and religious law under which many marriages are conducted. Many national constitutions provide exceptions for personal or family law, facilitating many other avenues for child marriages to be practised’’ [34].
In fact, the inequitable distributions of early marriage and adolescent childbearing revealed in this paper are part of a more structural problem of socioeconomic inequalities, territorial disparities and health iniquities in Morocco which slowed down the country's development for decades [35-39].
Ethical Approval Statement
This paper does not need ethical approval since it uses secondary data published by DHS and PAPFAM which all allow utilisation of data by just referring to the data source.
Competing interest
The author has no competing interest
Financial support
This work had no financial support
References
- W1. UNICEF (2021) Child marriage, USA.
- United Nations Human Rights (1989) Convention on the Rights of the Child (1989), Geneva, Switzerland.
- United Nations (1924) Geneva Declaration of the Rights of the Child (1924), Geneva, Switzerland.
- United Nations Human Rights (1959) Declaration of the Rights of the Child (1959), Geneva, Switzerland.
- United Nations Human Rights (1966) International Covenant on Civil and Political Rights (1966), Geneva, Switzerland.
- World Health Organization (2012) Sixty-Fifth World Health Assembly A65/13 (2012) Early marriages, adolescent and young pregnancies, Geneva, Switzerland.
- Kingdom of Morocco, Ministry of Justice (2004) Family Code ‘‘Moudawana’’, Morocco.
- Economic, Social and Environmental Council (2019) What to do about the persistence of child marriage in Morocco. Selfreferral No. 41/2019, Morocco.
- Public Ministry in partnership with UNICEF (2021) Diagnosis on child marriage [Diagnostic sur le mariage des enfants.
- World Health Organization (2008) CSDH (2008) Closing the gap in a generation: health equity through action on the social determinants of health, Final Report of the Commission on Social Determinants of Health, Geneva, Switzerland.
- Boutayeb A (2020) Social Determinants of Health and Health Equity in the WHO African Region In: Disease Prevention and Health Promotion, Springer Nature Switzerland.
- CSDH-EMR (2021) Build back fairer: achieving health equity in the Eastern Mediterranean Region. Report of the Commission on the Social Determinants of Health in the Eastern Mediterranean Region, Morocco.
- Demographic Health Surveys (2004) Population and Family Health Survey (EPSF) [Enquête sur la Population et la Santé Familiale (EPSF)]. Morocco DHS 2003-2004, Morocco.
- Morocco PAPFAM (2011) Population and Family Health Survey. [Enquête sur la Population et la Santé Familiale], Morocco.
- Morocco PAPFAM (2018) Population and Family Health Survey [Enquête sur la Population et la Santé Familiale], Morocco.
- United Nations Children’s Fund (UNICEF) 2018 Child marriage around the world, 2018, USA.
- Yaya S, Odusina E.K, Bishwajit G (2019) Prevalence of child marriage and its impact on fertility outcomes in 34 sub-Saharan African countries. BMC International Health and Human Rights 19: 33.
- Roudi-Fahimi F, Ibrahim S (2013) Ending child marriage in the Arab region, Kenya.
- UNFPA (2020) Advancing the Evidence Base Strategies to End Child Marriage and Support Married Girls Meeting Report, Kenya.
- UNFPA-UNICEF (2021) Evolution in the evidence-base on child marriage 2000-2019, USA.
- Boutayeb A (2012) Evolution of rural–urban health gaps in Morocco: 1992–2011. BMC Res Notes 5: 381.
- Egypt Demographic and Health Survey (DHS) (2014) Egypt Demographic and Health Survey, Egypt.
- Jordan Demographic and Health Survey (DHS) (2018) Jordan Demographic and Health Survey DHS 2017-18, Jordan.
- Yemen Demographic and Health Survey (DHS) (2013) Yemen Demographic and Health Survey DHS 2013, Yemen.
- Iraq MICS (2018) Surveys, Switzerland.
- Palestine MICS (2021) Palestinian Multiple Indicator Cluster Survey 2019 - 2020 Survey Findings Report, Palestine.
- Qatar MICS (2012) State of Qatar Monitoring the situation of children and women, Qatar.
- Sudan MICS (2014) SUDAN Multiple Indicator Cluster Survey 2014, Sudan.
- Tunisia MICS (2018) TUNISIA Indicator cluster survey multiple (MICS) 2018, Tunisia.
- ONDH (2021) Intersectional discrimination of women in Morocco [Discriminations intersectionnelles des femmes au Maroc], Morocco.
- Boutayeb A, Lamlili M, Boutayeb W (2021) Panoramic review of inequalities and their impact on human capital and human development in Morocco [Revue panoramique des inégalités et leur répercussion sur le capital humain et le développement humain au Maroc]. Publication de l’Université Mohamed Premier, Morocco.
- Sabbe A, Oulami H, Zekraoui W, Hikmat H, Temmerman M, et al. (2013) Determinants of child and forced marriage in Morocco: Stakeholder perspectives on health, policies and human rights. BMC International Health and Human Rights 13: 10.1186/1472-698X-13-43.
- Sabbe A, Oulami H, Hamzali S, Oulami N, Le Hjir FZ, et al. (2015) Women’s perspectives on marriage and rights in Morocco: risk factors for forced and early marriage in the Marrakech region. Culture, health & sexuality 17: 135-49.
- UNICEF (2017) Child marriage in the Middle East and North Africa, Switzerland.
- Boutayeb A, Boutayeb W, Lamlili M (2018) A mini review of health inequity, territorial disparities and socio-economic inequalities in Morocco. International Journal of Management and Applied Science 4: 23-9.
- Boutayeb W, Lamlili M, Ben El Mostafa S, Boutayeb A (2015) Socio-economic inequalities in Morocco: a brake on human development [Inégalités socioéconomiques au Maroc : un frein au développement humain]. Annales des Sciences de Santé 1: 4-12.
- Daush U, Saoudi H (2019) Inequality in Morocco: An International Perspective. Policy Paper 19/13.
- Bakour C, Abahamid MS (2019) Regional disparities in development in Morocco: Statistical analyses using dispersion indicators and multidimensional techniques. MPRA Paper No. 97105.
- Atia M, Said Samlali S (2021) Government Efforts to Reduce Inequality in Morocco Are Only Making Matters Worse, Middle East Report Online, Morocco.
Artcle Information
Review Article
Received Date: March 01, 2025
Accepted Date: March 19, 2025
Published Date: March 26, 2025
Annals of Public Health and Preservative Medicine
Volume 1 | Issue 1
Citation
Boutayeb A (2025) Evolution of Early Marriage and Adolescent Childbearing by Social Determinants of Health in Morocco. Ann Public Health Preservative Med. Ann Public Health Preservative Med 1: 103
Copyright
©2025 Boutayeb A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: appm.2025.1.103