

Review Article
Volume-1 Issue-1, 2025
The Effect of Unsafe Premarital Sexual Practice on The Prevalence of HIV And Other Sexual Transmitted Diseases in Ethiopia: A Cross Sectional Study
Received Date: May 03, 2025
Accepted Date: May 21, 2025
Published Date: May 28, 2025
Journal Information
Abstract
Background: According to the UNAIDS 2007 report, there are an estimated 33.2 million people living with HIV and 2.5 million became newly infected with the virus while 2.1 million lost their lives because of HIV. Therefore, the aim of this study is to assess the effects of traditional premarital sexual practice on the prevalence of HIV and other sexual transmitted diseases.
Methods: Community based cross-sectional study was conducted from April to June 2018 G.C at Gambella Peoples’ National Regional State. A sample of 151 youth of age between 15-24 from three kebles and 9 elders and 8 officers were taken for the study using simple random sampling and purposive sampling technique. It was analyzed using simple statistical techniques and chisquare and logistic regression.
Results: The results of this study indicated that 100% of the respondents were practiced sex starting with the minimum age of first sexual intercourse 10 and maximum age of 19. Having multiple sexual partners and the elders’ response/ encouragement of the tradition had shown high positive relationship and effect with prevalence rate of STDs.
Conclusion: Prevalence of HIV and sexual transmitted diseases were relatively high. Therefore, it is better to be designed appropriate interventions and working together with deferent stakeholders for the implementation of the intervention and as well as to reduce the transmission rate.
Key words
Traditional Premarital Sexual Practice; Multi Sexual Partners; Ethiopia
List of abbreviations: AIDs: Acquired Immunodeficiency Syndrome; ANC: Anti Natal Care; ART: Anti Retro Viral Therapy; CDC: Centre for Disease Control; CSAE: Central Statistical Agency of Ethiopia; EDHS: Ethiopian Demographic Health surveys; FMOH: Federal Ministry of Health; GAMET: Global HIV/AIDS Monitoring and Evaluation Team; GPNRS: Gambella Peoples National Regional State; HAPCO: HIV/AIDS Prevention and Control Office; HIV: Human Immunodeficiency Virus; MOH: Ministry of Health; PEPFAR: President's Emergency Plan for AIDS Relief; SNNPR: Southern Nations Nationalities People Region; SSA: Sub Saharan Africa; STDs: Sexually Transmitted Diseases; UNAIDS: The joint United Nations programme on HIV/AIDs; WHO: World Health Organization
No |
Kebele |
Total population un married youth |
Proportion |
Sample size |
||||
Youth(random |
Elders(purposive |
officers(purposive |
||||||
Male |
Female |
Total |
||||||
1 |
Godriemishin |
59 |
39 |
98 |
39.7% |
98 |
3 |
8 |
2 |
Dushi |
34 |
22 |
56 |
22.7% |
56 |
3 |
0 |
3 |
Kumi |
56 |
37 |
93 |
37.6% |
93 |
3 |
0 |
|
Tatal |
149 |
98 |
247 |
100% |
151(m=91,F=60) |
9 |
8 |
No. |
Variables |
Category |
Frequency |
Percent |
1 |
Sex |
Male |
89 |
60.1 |
Female |
59 |
39.9 |
||
Total |
148 |
100 |
||
2 |
Age |
15-19 |
88 |
59.5 |
20-24 |
60 |
40.5 |
||
Total |
148 |
100 |
||
3 |
Educational back ground |
Primary level |
50 |
33.8 |
Secondary level |
30 |
20.3 |
||
Certificate& above |
17 |
11.5 |
||
Read &write only |
32 |
21.6 |
||
Not read and write |
19 |
12.8 |
||
Total |
148 |
100 |
||
4 |
Occupation |
Student |
73 |
49.3 |
Farmer |
12 |
8.1 |
||
Daily laborer |
11 |
7.4 |
||
Civil servant |
19 |
12.8 |
||
Un employed |
33 |
22.3 |
||
Total |
148 |
100 |
No. |
Variables |
Frequency |
percent |
1 |
Place for sexual practice Traditional house (Depo) |
88 |
59.5 |
2 |
Duration of years of respondents in practicing sex One year and less |
4 144 |
2.7 97.3 |
3 |
Time when the respondents are going to stop practicing sex with multiple sexual partners |
110 24 14 |
74.3 16.2 9.5 |
4 |
Time of the respondents in practicing sex Weekly during market day |
74 74 |
50 50 |
No. |
Variables |
Frequency |
Percent |
1 |
Source of information for youth about HIV&STDs Partner/relatives |
23 88 8 12 2 6 8 147 |
15.5 59.5 5.4 8.1 1.4 4.1 5.4 99.4 |
2 |
Mode of transmission Unprotected sex Mother to child Circumcision Tonsillectomy |
47 6 1 3 147 |
31.8 4.1 0.7 2 99.4 |
3 |
Willing to participate in VCT and other STDs test Yes |
138 10 |
92.6% 7.4% |
4 |
Discussing about HIV and STDs with family/friends Yes |
103 45 |
69.6% 30.4% |
Variables |
Infected by STDs |
Chi-Square (x²) |
|||
N |
Infected |
Not infected |
|||
Sex |
Male |
89 |
28% |
72% |
0.101 |
female |
59 |
31% |
69% |
||
Age |
15-19 |
88 |
20% |
80% |
7.788* |
20-24 |
60 |
42% |
58% |
||
education |
Literate |
129 |
27% |
73% |
1.801 |
Illiterate |
19 |
42% |
58% |
||
Job |
Student |
73 |
25% |
75% |
1.351 |
Others |
75 |
33% |
67% |
||
Variables |
Infected by STDs |
Chi-Square (x²) |
p-value |
|
Yes |
No |
|||
Ever heard about STDs |
|
|
|
|
Yes |
41 |
88 |
|
|
No Total |
2 |
17 |
3.630 |
0.057 |
Variables |
Infected by STDs |
C hi-s q u a r e (x²) |
p-value |
|||
Yes |
No |
|||||
Freq. |
% |
Freq. |
% |
|||
Age that sexual intercourse begun |
|
|
|
|
|
|
10-14 |
23 |
38 |
38 |
62 |
|
|
15-19 Total |
20 43 |
23 29 |
67 105 |
77 71 |
3.768 |
0.052 |
Having multiple sexual partner |
|
|
|
|
|
|
Yes |
40 |
43 |
54 |
57 |
|
|
No Total |
3 43 |
6 29 |
51 105 |
94 71 |
22.776 |
0.000 |
Having regular sexual partner Yes Total |
20 23 43 |
24 35 29 |
62 43 105 |
76 65 71 |
1.94 |
0.164 |
Having Casual sex Yes Total |
40 3 43 |
42 6 29 |
55 50 105 |
58 94 71 |
21.922 |
0.000 |
Use of condom during sexual practice Yes |
10 |
18 |
46 |
82 |
5.479 |
0.019 |
Parents response for sex practice Encourage Total |
37 6 43 |
37 12 29 |
62 43 105 |
63 88 71 |
10.041 |
0.002 |
Elders response for sex practice Encourage Total |
42 1 43 |
34 4 29 |
80 25 105 |
66 96 71 |
9.723 |
0.002 |
Variables |
B |
S.E. |
Wald |
df |
Sig. |
Exp(B) |
Use of condom during sexual practice |
-1.137 |
.454 |
6.268 |
1 |
.012 |
.321 |
2.419 |
1.070 |
5.115 |
1 |
.024 |
11.234 |
|
2.499 |
.647 |
14.920 |
1 |
.000 |
12.169 |
|
-4.074 |
1.353 |
9.067 |
1 |
.003 |
.017 |
Introduction
Background: According to the UNAIDS 2007 report, in the world, there are an estimated 33.2 million people living with HIV and 2.5 million became newly infected with the virus while 2.1 million lost their lives due to HIV/AIDS [1]. Similarly, sexually transmitted diseases are the major cause of acute illness, infertility, long-term disability, and death [1].
Africa is the region critically suffered by the spread of HIV/AIDS and within this continent; 70% of people who are living with HIV found in Sub-Saharan Africa [3]. Sub-Saharan Africa (SSA) is one of the hot spots where HIV/AIDS and STDs is widely spread and it is harder hit by the consequences of the epidemic than other parts of the world(4). Similarly, STDs are amongst the top five disease categories in developing countries [2] but Peoples in different social groups will not have equal exposure to STDs and HIV/AIDS because of the culture that they have practiced [5].
Ethiopia has one of the lowest HIV prevalence rates in East Africa, but there are still more than one million people estimated to be living with HIV [6].
Gambella peoples’ national regional state/GPNRS/ which has a small and sparsely populated region have the highest regional prevalence from all regions of Ethiopia (6.5%) and with little distinction between urban and rural prevalence [7].
Having sex with multiple partners, especially without using a condom, puts women and men at risk of acquiring HIV and other STDs. Multiple sexual partnerships were very rare among women, less than 1% in Ethiopia reported having more than one sexual partner in the year before the survey. The one exception is women in Gambella, where 11% report having had more than one sexual partner in the year before the survey. Multiple sexual partnerships are slightly more common among men (4%) in Ethiopia, in Gambella; multiple sexual partnerships were the most common among men (9%) [6].
In the study area, there were no refuges, there is no female genital mutilation, there was no traditional practice called levirate marriage and there is no big town in the woreda which facilitates the STDs infection by motivating the youth to casual sex. Therefore, what is the main reason for this tragedy? In 2005 an estimated 3.2 million people in the region became newly infected, while 2.4 million were died by AIDS. Among the younger generation particularly the age between 15 and 24 years, women infected by HIV accounted 4.6% and men accounted for 1.7% [8].
Supporting the above idea research was conducted in South Africa stated that the HIV/AIDS pandemic has taken a grave toll on sub-Saharan-Africa [9], where AIDS is now the prime cause of death despite a range of prevention strategies.
The epidemiology of each STDs is different and is influenced by various factors, including sexual mixing patterns (moderated by protective behaviors), the transmissibility of each pathogen, and the duration of infectiousness (moderated by access to effective treatment), demographics, and social circumstances. The highest rates of incident STDs have been reported for adolescents and young adults [10,11].
The estimation of prevalence rate of HIV from EDHS’s in 2005 shows that 1.4% in country level which is 6% and 0.7% in urban and in rural areas respectively [12]. Federal ministry of health of Ethiopia (FMOH) database of antenatal care (ANC) survey for the same year shows that the estimated prevalence rate of HIV was 3.5% in country level, 10.5% urban and 1.9% in rural areas [12,13].
The true magnitude of STDs in developing countries including Ethiopia was not well known; data on the prevalence and incidence of STDs and their complications were limited and STDs were often under-reported because of failure to identify asymptomatic cases or because infected individuals do not disclose symptoms due to the social stigma associated having an STDs [14]. Even though there is little information on the incidence and prevalence of STDs in Ethiopia. According to Ethiopian 2011 Demographic Health Survey, 1%, of each Ethiopian women and men reported having had sexually transmitted infections in the past 12 months before the survey. Three percent of women and 2% of men reported having had an abnormal genital discharge. In addition, 1% of each women and men reported having had a genital sore or ulcer in the 12 months before the survey. These numbers may be underestimated because respondents could be embarrassed or ashamed to admit having STDs [15].
According to 2011 Ethiopia Demographic and Health Survey, the prevalence rate of HIV/AIDS ranges from the highest prevalence rate 6.5% (Gambella region) to the lowest level of 0.9% in South Nation Nationality People (SNNP) region. There is also significant discrepancy among place of residence, women who live in urban areas are 6.5 times higher than the women who are living in rural areas [16]. Similarly, the prevalence rate of STDs in Ethiopia varies across regions because of different factors. The prevalence rate of neisseria gonorrhea among suspected STD patients in Gambella was 11.3% which is higher than 5.1% reported in Hawassa [17] and 8.2% in Bahirdar [18]. Relatively higher rate of STD in Gambella region might be due to risky cultural practices in the region where there are polygamy and levirate marriage [19]. The prevalence rate of adult HIV/AIDS infection of Gambella regional state in 2007 was 2.4%. moreover according to Federal HIV/AIDS prevention and control office of Ethiopia, 2017 projection, the prevalence rate of adult HIV/AIDS infection in Gambella region will be estimated as 4.01% in 2015, 4.0% in 2016, 4.09% in 2017, 4.2% in 2018, 4.3% in 2019, 4.39% in 2020, and 4.49% in 2021[20]. Hence from this estimation data, we can see that the prevalence rate of adult HIV/AIDS infection in this region increases continuously starting from 2016 up to 2021.
In a report to the BBC Radio on 01 December 2004, Kofi Annan, the former United Nations Secretary-General, reported that sub-Saharan Africa has the highest rate of HIV/ AIDS and STDs infections and the young women and men are the most affected by this pandemic. This leads to the question of what factors may help to explain the spread of HIV and other STDs in sub-Saharan Africa [20].
The common modes of transmission of HIV in developed countries homosexual sex and intravenous drug injection are usually considered to be the means of transmission of HIV/ AIDS. On the other hand, in developing countries, heterosexual contact is the main mode of transmission [21]. Factors thought to influence this sexual transmission in the content include promiscuity, with a high prevalence of sexually transmitted disease; and cultural practices that are possibly connected with increased virus transmission like female "circumcision"/ infibulations/ and others [22].
The recent spread of AIDS throughout Africa raises the question of whether the mode of transmission of human immunodeficiency virus (HIV) in Africa is different from that in the United States and other Western countries. Because of the absence of risk factors of intravenous drug abuse and homosexuality in subSaharan Africa the patterns of transmission of HIV/AIDS are different from those in Western society. The difference is especially apparent because the male-to-female ratio of affected individuals is 1:1 in Africa vs. 19:1 in the United States and Europe. This report briefly examines cultural practices that may contribute to the spread of AIDS in Africa and highlights areas that require further research [22-25]. Generally, from the above empirical studies we can understand that cultural practice is one of the main factors for high prevalence rate of STDs in Africa. Therefore, the main aim of this study is assessing the effects of traditional premarital sexual practice on the prevalence of HIV and other STDs among youths’ in Gambella Peoples’ National Regional State, Southwest Ethiopia.
Methods
Research Approach and design
Community based cross-sectional study was conducted from April to June 2018 G.C at Gambella Peoples’ National Regional State.
The study employed both qualitative and quantitative research approach. Descriptive research design was used to describe the back ground of the respondents. Explanatory research design was also used particularly chi-square and logistic-regression to analyze the association between variables and to assess the effects of traditional premarital sexual practice on the prevalence of HIV/AIDS and other STDs.
The Study Area
Gambella Peoples’ National Regional State/GPNRS/ is one of the regions among the ten regional states in Ethiopia. It is located in the south-west of Ethiopia between the geographical coordinates of 6º,28',38" to 8º,34' north latitude and 33º to 35º,11',11" east longitude covering an area about 34,063km2.The GPNRS is bounded to the south and south-east by the southern nations and nationalities peoples regional state, to the north and northeast and east by Oromia national regional state, south-west, west, and north-west by the Republic of South Sudan.
Data Type and Sources
Quantitative data was collected from Youths (15-24 years old) living in Gambella and the data which showed the prevalence of HIV in the region was taken from region health office. Qualitative data was collected from nine elders who were drawn from selected Mengesh woreda, and four officers from governmental office positions were the major source of the data.
Methods of Data Collection
Face to face interview was applied for collecting the data.
Sampling Design
Population, Sampling Unit and Sampling Frame
The target population of this study was youth’s between15 and 24 ages in Gambella at Mengesh woreda which consists of 247 listed in kebele administration and 8 officers from four selected sectors and nine elders from three kebles was included. The age between 15 up to 24 of youths was taken because women were married at a median age of 16.5 and men at 23.2 years old.
Method of Sampling
Both probability and non-probability sampling methods were applied due to the nature of the study. In probability sampling, we used simple random sampling method and from non-probability sampling such as purposive sampling was used to select the participants and interviewees selected from health offices, women affairs, youth and culture and tourism office, heads and process owners.
Sampling Procedure
151 youths were selected from 247 populations from the list found in the selected woreda by using simple random sampling and also used a purposive sampling technique to select 8 respondents from four offices and 9 elders from 3 kebles in Mengesh woreda. The three kebles were selected purposively because from 13 kebles there were only four kebles which had a market day in which unsafe premarital sexual practice took place weekly.
Sample Size determination
Sample size was determined using single population proportion
formula assuming that p-value =50% with 95%CI and 5% margin
error was used to select a sample of youth that is living in Mengesh
woreda. Hence the required sample size was determined by using
the formula if N is finite then the sample size n, but to
get n,
but to
get n,  where: -
where: -
N = Population size
n = Desired sample size factor
z = Standard normal variable at 95% required confidence level
p = Estimated characteristics of target population
Since p is actually what we are trying to estimate, then one method may be to take the value of p=0.5 in which “n” will be the maximum and the sample will yield at least the desire precision.
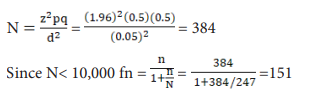
So, the sample size was derived from the target population of 247 youths. On the other hand, by applying purposive sampling technique 4 leaders and 4 experts were identified from institutions of health offices, culture and tourism, women affairs and youth office and 9 elders from three kebeles. Therefore, the total sample size of this study was constituted 168 respondents (Table S1).
Method of data analysis
Quantitative data analysis
After the quantitative data collected the relevant data was coded, summarized and transferred to SPSS-20 to analyzed and presented. The Statistical Package for Social Science Computer software (SPSS) was used for the numerical data analysis in terms of descriptive statistics such as frequency, percentage, graphs, charts and tables. Descriptive statistics was used to measure the awareness of the respondents towards HIV/AIDS and STDs and to find out to what extents the respondents were practicing premarital sex practice.
In addition to the above, we used both chi-square test and logistic regression. Chi-square test was applied to explore the relationships between, knowledge on STDs including HIV and traditional premarital sex practice with HIV/AIDS and STDs prevalence. For multivariable analysis logistic regression model used to analyze the association between the outcome variable with independent variable. The strength of association was measured using Chi-square and level of statistical significance was declared at p-value less than 0.05.
Qualitative data analysis
The qualitative data collected from open ended interviews was also analyzed qualitatively by categorizing and forming themes. Accordingly, the recorded data were transcribed into words and fallowing categories were made under thematic area on the bases of research questions. This analysis was used to see the extent of the practice of traditional premarital sex and to describe its’ effect on the prevalence of STDs and to see the awareness of youths about HIV and other types of STDs. The results from qualitative analysis were used to substantiate the result of quantitative analysis.
Triangulation
Both the quantitative and the qualitative data analysed had been triangulated in discussion and interpretation part and the mixed result also related with existed research findings.
Data Quality assurance
The following activities were done to ensure the quality of data and reduce errors as much as possible.
• Training was given for one supervisor and for three data collectors for three days.
• A pre-test conducted in Newi keble with 20 youth respondents to check consistency and vagueness.
• Explanation was given to the individuals how to fill the questionnaire by the data collectors.
Finally, editing and proper coding activities have been carried out after data collection.
Result
For the quantitative data, a sample of 151 unmarried youth selected from three kebles in Menegesh Woreda. A total of 148 questionnaires were filled and returned with 98% response rate. In addition to the above, eight officers of four selected offices were interviewed and nine elders from three kebles. These individuals discussed with open-ended questions to complement the result gained in quantitative sections.
Demographic Information of the Respondents
The study sought to find out the demographic information of the respondents concerning their gender, age, education, and job (Table S2).
Age distribution of the respondents
The ages of the respondents were categorized into two age groups: 15-19 years (adolescence) and 20-24 years age group. As shown from table-2, we can see that 88(59.5%) of the respondent were between 15 and 19 years, while 60(40.5%) of the respondents were between 20 and 24 years. This result revealed that most of the youths especially females most of the time started sexual intercourse and have got married before 19 years old.
Educational Background of the Respondents
Among respondents 50(33.8%) of were found with primary level of education, 30(20.3%) of the respondents were secondary level, 32(21.6%) of the respondents could only be able to read and write, 17(11.5%) of the respondents were found with certificate and above and 19(12.8%) of the respondents had no formal education and couldn’t able to read and write.
Occupation of the respondents
Majority of the respondents (51.4%) were students, 22.3% of the respondents were unemployed, 12.8% were civil servants, 7.4% were daily laborer and 6.1% of the respondents were farmer.
Sexual behavior and sexual practice of the respondents
The whole respondents practice sex starting with the minimum age of first sexual intercourse 10 and maximum age of 19 years. The mean age at first sexual intercourse was 14.8 years.
When the respondents were asked about the number of their sexual partners, 54 (36.5%) had not practiced with multiple sexual partners, 94 (63.5%) had practiced with multiple sexual partners. It was reported that 82(55.4%) of the respondents had a regular sexual partner while 66(44.6%) of them didn ot have regular sexual partners. The 95(64.2%) of the respondents of those who had regular sexual partners and who had not regular sexual partners had practiced premarital sexual practice with unknown sexual partners. From this, we can see that 29(19.6%) of the respondents practiced sex with unknown partners in addition to their regular sexual partners.
Concerning preventive methods of HIV and STDs particularly using of a condom during premarital sex practice, only 13(8.8%) of the respondents had used condom frequently during premarital sex practice and 43(29%) had used it occasionally when their sex partner forced to use it. In relation to reasons for not using condom, 49 (33.1%) said that having sex with condom did not have pleasure, 50(33.8%) were replied that condom is not culturally supported, 18(12.2%) said that condom was not available and 17(11.5%) of the respondents reported that using of condom did not have any value.
Key respondents from health offices replied that youths in the study area were practicing premarital sex with multiple sexual partners without using condom. This is because boys believed that it was not comfortable and there is no pleasure in making sex using a condom while girls believed that making sex with a condom would have an effect on their womb.
Similarly, interviewees from women affairs office replied that most of the time the young girls were affected by HIV virus. Since youths were practicing unsafe sex during the market day and during a funeral ceremony. Most of the time girls were not interested in making sex using a condom. In addition, the girls were not familiar with other contraceptives; if they became pregnant during their sexual practice the boy would be forced by the girl’s parents through elders to marry her. In general, officers said that most of the girls denied about the presence of STDs and HIV virus.
The majority of girls began sexual contact in the age between 10 up to 14 while the majority of boys began sexual intercourse in the age between 15 up to 19. This implies that majority of girls began sexual practice earlier than boys.
Elders replied that most of the time girls started sexual practice at the age of 13 years and boys started at 15 years old.
As shown in Table-4 below when the respondents asked to respond concerning the place that sexual practice took place, 88(59.5%) of the respondents practiced sex within the small house called “Depo” which is a traditional small house constructed by an adolescent boy for the purpose of practicing sex and 60(40.5%) of the respondents practiced sex in other places.
Similarly, the respondents were asked to respond concerning the main reason for practicing sex and the majority 121(81.8%) of the respondents replied that they were participating because premarital sex practice is a tradition in that area where as 27(18.2%) said that they were participating to simply satisfy their sexual feelings.
From the sample of the respondents, the majority which was 97.3% reported that they had been practicing premarital sex for about two and more than two years, and only 4(2.7%) of the respondent had been practicing for about one year and less. In addition, 50% of the respondents practiced premarital sex weekly during the market days and the rest 50% practiced any time.
Officers interviewed from youth office replied that most of the time premarital sex practice was practiced weekly in the market day after the boys playing football game. It is common to see couples walking together and at night they were practicing traditional sex practicing in the traditional house called “Depo” or other places. In addition to the above according to the officers, the youth had been practicing traditional premarital sex practice during religious conferences when the girls and boys travel far from their keble to reach the conference and at night the youth practiced sex.
Concerning the time that the youth were going to stop practicing premarital sex practice, 110(74.3%) responded that they will stop practicing as soon as they have got married, 24(16.2%) of the respondents replied that they will stop when they become old and 14(9.5%) of the respondents said they will never stop practicing sex with multiple sexual partners (Table S3).
With regard to parents’ and elders’ response concerning the premarital sexual practice, 92 (62.2%) of the respondents replied that the parents were encouraging the premarital sex practice while 37.8% of the respondents said that they were discouraging the practice. Similarly, 77.7% of the respondents reported that the elders encourage the premarital sexual practice and the rest 22.3% of the respondents replied that the elders were discouraging the practice.
From the culture and tourism office, the interviewees responded that the traditional practice had been practicing for many generations. Most of the time the boys construct a small house near to the big family house called “Depo”, for the purpose of practicing premarital sex inside this small house. The youth did not use a condom during sexual intercourse and they were practicing with multiple sexual partners. According to the officers, one of the main reasons for practicing premarital sex practices without using a condom was to have children and to increase the population of the ethnic group. The elders believe that the number of the population of is very small and it needs to increase. If the girl became pregnant then the boy would marry that girl after paying some money to her parents in the form of bride money
In addition to the above key respondents from elders replied that the boys constructed a small house when they became adolescent to imitate their father and they had practiced sex in that house. According to their report, parents as well as the elders were not discouraging this tradition and this is one of the ways of making marriage among the youth.
Knowledge of youth about HIV & other types of STDs
Among the respondents, 147 (99.3%) had heard about HIV/AIDS and 129(87.2%) the respondents know about other types of STDs.
When the respondents asked about the curability of HIV, majority (60.8%) of the respondents replied that HIV is not curable. Concerning the possibility of a healthy-looking person to have HIV and STDs positive, 60.2% of the respondents reported that STDs status of an individual cannot be detected by observing physically so that a healthy-looking person may have the possibility to be HIV and other types of STDs. Lastly, 58.8% of the respondents said that it is possible to prevent STDs including HIV by changing risky sexual behavior. Hence from the above finding, we can say that majority of the respondents are aware of STDs including HIV.
The interviewees from health officials said that most of the youth in Mengesh woreda had awareness on HIV/AIDS and other STDs infections. They reported that most of the youth knew about the ways of transmission and even the prevention methods. The main problem of youth was the problem of attitudinal change, they do not care about HIV virus and other STDs whether they are infected or not. Especially HIV was taken as a harmless disease by the society and the community of the study area said it “love disease”. Every quarter there was a campaign of voluntary testing and counseling (VCT) in the woreda at different keble, and most of the youth were interested to participate in the campaign. However, they were not happy when they became HIV negative and feel nothing when they became positive and even, they are not voluntary to take antiretroviral therapy (ART) after they knew they are HIV positive. The respondents replied that the youths are afraid of Tuberculosis rather than HIV.
For those who heard of HIV, the main source of information was health workers 88 (59.5%), friends/relatives 23 (15.5%), school 12(8.1%), social gathering 8(5.4%), religious leaders 8(5.4%), media/TV/radio 6(4.1%), and Leaflets or brochures 2(1.4%).
The major ways of HIV/AIDS transmission as replied by respondents were having unprotected sex 47 (31.8%), unsafe injection 22 (14.9%), sharing razor 17 (11.5%), mother to child 20 (13.5%) and circumcision 19(12.8%), Tonsillectomy 7(4.7%), blood transfusion 6(4.1%), and milk teeth Extraction 5(3.4%). Despite the knowledge about HIV/AIDS, 3 (2%) of the respondents said that it is transmitted by eating raw meat and 1(0.7%) by an insect bite.
In relation to voluntary testing and counseling and other STDs tests 138(92.6%) of the respondents said that they were willing to test their HIV and STDs status while 10(7.4%) were not willing to test.
The reason for not voluntary in the testing of HIV and STDs were, 5(3.4%) replied that it was because of fear of social stigma were as the rest 5(3.4%) said that they were not practicing sex with multiple sex partners so that they do not need any test. From the sample of the study 103(69.6%) were discussing with their friends/family members about HIV and STDs (Table S4).
The prevalence rate of HIV/AIDs and other type of STDs
The prevalence of HIV infection of the youth of age between 15 and 24 were 15.9% and among girls it was (16.8%) which was greater than the prevalence of HIV infection of boys (14.8%). Similarly, the prevalence of the respondents of STDs infection is 29.1% and the prevalence among boys was (28.1%) was less than the prevalence of STDs among girls was (30.5%). Hence from this we can see that girls in the study area were more affected by STDs and HIV than boys.
Supporting the above idea interviewees from woreda health office reported that HIV/AIDs were the major health and development problem in Mengesh woreda.
Bivariable and Multivariate Result of Infection of Youth by STDs and it’s Correlated Factors
In this section, an attempt made to identify some demographic variables, awareness of youth towards HIV and STDs and socio-cultural variables like traditional premarital sex practice of youth were correlated with the prevalence rate of STDs and HIV by applying both bivariable and multivariate analysis. Bivariable analysis was done applying the Chi-square test, while the multivariate analysis was performed using binary logistic regression model.
Prevalence rate of STDs and HIV/AIDs across demographic variables
The bivariable analysis for the youth demographic characteristics revealed that only the variable age had a significant relationship with respondents infected by STDs. As can be observed from table-4, showing the cross-classification of age with STDs, of 88 adolescents in the age group 15-19, about only 20 % reported having had infected by STDs. Among youth in the age group 20-24, about 42 % admitted having had infected by STDs. The Pearson chi-square result has also depicted that age of STDs infection is significantly associated with one another with a p-value less than or equal to 0.05. This shows that as the age of the respondents’ increases the prevalence rate of STDs also increases. The rest demographic variables, like sex of the respondents, educational level and respondents’ field of occupation did not have a significant association with the prevalence of STDs.
The main mode of transmission of both HIV and other STDs is sexual intercourse and STDs facilitate HIV transmission by increasing both HIV infectiousness and HIV susceptibility(26) and according to Kenyon there is strong positive association (with r=0.85, p< 0.0001) between prevalence rate of STDs and HIV/ AIDs(27). Therefore, if ages of the respondents have the significant relationship with respondents infected by STDs then the variable age will have a significant relationship with the prevalence rate of HIV/AIDs (Table S5).
Knowledge about STDs and HIV and prevalence rate
Since the expected count in chi-square was less than five the variable awareness about HIV/AIDs could not be included in the chi-square test, while concerning the awareness of youth about STDs, the chi-square test shows that there was no significant association with the prevalence rate of STDs. Most of the respondents were aware of HIV as well as other types of STDs infections but the prevalence was still high. During the interview, the officers from health office replied that the youth were aware of STDs and HIV, but they were not preventing themselves from this infection because of lack of attitudinal change and because of cultural factors particularly the traditional premarital sex practices (Table S6).
Socio-cultural variables and prevalence of STDs and HIV/AIDs
As it is shown in Table S6 below the socio-cultural variables such as, having multiple sexual partners, having casual sex, using of condom during sexual practice, parents and elders positive response towards premarital sex practice were found to be a statistically significant association with the prevalence of STDs infection of youth, while the variables such as age that sexual intercourse begin and having regular sexual partner did not have significant association with prevalence rate of STDs infection. 42.6% of those who had practiced premarital sex with multiple sexual partners and those who had practiced sex with unknown sex partners have infected by STDs, while only 5.6% of those who were not practicing sex with multiple sexual partners and was not made casual sex were infected by STDs.
Similarly, concerning the use of a condom during sexual practice, from those who have been frequently using condom during sexual contact, none of them had infected by STDs, while 23.3% of the respondents of those who have been using a condom rarely during sexual practice had infected by STDs. Moreover 86% and 97.6% of STDs infected respondents are those who had been encouraged to practice sex by parents and elders respectively.
On the other hand, having a regular sexual partner did not have a significant association with the prevalence of STDs. Youth in the study area practice sex with unknown sexual partners in addition to their regular sexual partners. Concerning the age that sexual practice begins, statistically, the chi-square test shows that there was no significant association with the prevalence of STDs but mathematically large number youth (38%) who started sexual practice earlier (10-14) have infected by STDs. There was only 23% of those who started sexual practice lately (15-19 years) infected by STDs. As far as there is strong positive association (with r=0.85, p< 0.0001) between the prevalence rate of STIs and HIV/AIDs the five variables which has significant correlation with the prevalence rate of STIs infection would have a statistically significant association with the prevalence rate of HIV/AIDs (Table S7).
Multivariate Analysis of Results
In the multivariate analysis binary logistic regression model was used for further analysis of the subject matter
As it is shown in Table S8, the sig. value was less than 0.05 which means we reject Ho which says B=0. Hence uses of condom during sexual practice, elders’ positive response towards traditional premarital sexual practice and traditional premarital sexual practice with multiple sexual partners have a significant effect on the prevalence of STDs. Since as it was stated in the above there was strong positive association between the prevalence rate of STDs and HIV, the three variables have also a significant effect on the prevalence of HIV.
When we interpreted the coefficient β of the three independent variables, B1= -1.137 implies that use of condom during sexual intercourse frequently had significant negative effect on the prevalence of STDs, B2=2.419 and B3=2.499 implies that elders’ encouragement of the practice and youths’ practicing sex with multiple sexual partners had significant positive effect on the prevalence of STDs (Table S8).
Discussion/Interpretation
It was found that 100 % of respondents have practiced premarital sex in their lifetime. Experience of sexual intercourse in this study was higher than the previous studies conducted in West Gojjam Zone, Ethiopia among youths which was 19% of the respondents ever had sexual premarital sexual intercourse [28]. This implies that the proportion of sexually experienced youth in the study area was greater than the proportion of sexually experienced youth of other areas of the region which has studied before.
This study has also found that all of the sexually experienced youth started their first sexual intercourse between 10-19 years old. The mean age at first sexual intercourse was 14.8 years. Majority of girls began sexual contact in the age of 10 up to 14, whereas the majority of boys began sexual intercourse in the age between 15 up to 19. This implies that girls in the study area started premarital sexual practice earlier than boys. Concerning this idea, interviewees from elders reported that traditionally girls started premarital sex earlier than boys. If girls started sex earlier, they will have a high probability to have sex with multiple sexual partners which causes HIV and other types of STDs. This idea was consistent with the epidemiological studies done in Africa cultural practice on effect of HIV/AIDS, which says girls begin to have sex at an earlier age are more likely to be infected with HIV and STDs [22,24].
The current study shows that unlike other parts of Ethiopia, in Mengesh woreda multiple sexual partnerships were more common. It was found that 64% of boys and 61% of the girls had multiple sexual partners.
This result is greater than the findings reported by Ethiopia Demographic and Health Survey in 2011, which shows 9% of men and 11% of women, had multiple sexual partners. In general, from current study, we can see that girls and boys within age between 15 and 24 had averagely 2 and 3 sexual partners respectively. Having unsafe sex with multiple sexual partners was one of the main factors for high transmission of HIV and other types of STDs. In relation to this idea the study done in Ethiopia revealed that multiple sexual partnerships were widely believed to be one of the main drivers of the HIV and other STDs epidemic in sub-Saharan Africa [29]. In addition, this finding was also consistent with the idea which says the main cause for the high prevalence rate of HIV in Gambella region was because premarital sex with multiple sexual partners was common in that region [30].
In the study area, adolescent boys construct small houses near to their parents’ house for the purpose traditional premarital sexual practices. As it was stated in the analysis section above, interviewees from elders reported that traditional risky sexual practice was not discouraged by elders as well as parents, because elders believe that the traditional practice was very important for boys’ and girls’ relationship and marriage. They replied that most of the time marriage took place after the girl getting pregnant through this practice.
Traditionally individuals were expected to stop the sexual practice as soon as getting married. From this idea, we can see that girls and boys practice sex with multiple sexual partners because they were encouraged by parents and elders and this can be one of the main causes for HIV and other types of STDs infections. This idea was consistent with idea says that the main reason for the high prevalence of HIV/AIDS and other types of STDs in Gambella region was socially accepted the risky premarital sexual practice [31].
The prevalence of HIV and STDs infection of the youth age between 15 and 24 years old in Gambella region of Mengeshi woreda was 15.9% and 29.1% respectively. This shows that the prevalence of HIV infection of youth in the current study was higher than the prevalence that previously reported by the Ethiopia Demographic Health Survey (EDHS) by the year 2011 which was 6.5% and the overall prevalence of HIV infection (8.5%) in Gambella Hospital among patients visited the PIHCT and VCT(31). Similarly, the prevalence of STDs in this study was greater than the prevalence of Gambella that previously reported which was 11.3% [19].
High prevalence of HIV and STDs infection in Mengesh woreda was demonstrated among respondents that had information about HIV and STDs transmission and prevention. This means that knowledge about HIV/AIDS and other STDs and its mode of transmission and prevention had not brought significant behavioral change in the study area.
The influence of culture based risky sexual practices particularly premarital sex practice of youth could be possible contributors for such unexpected outcomes. During the interview the respondents from woreda health office replied that most of youth in Mengesh woreda had information about HIV/AIDS and STDs. They reported that most of the youth knew about the ways of transmission and even the prevention methods. The main problem of youth was the problem of attitudinal change, they do not care about HIV virus and other STDs whether they are infected or not. HIV and other types of STDs are considered by the youth as well as by the community as harmless diseases and they called it “love diseases”. Supporting these ideas with book critical psychology clearly stated that even though individual factors such as knowledge and confidence play a key role in sexual behavior and the spread of HIV and STDs, these and other individual factors are shaped by individual’s social context [32]. From this study, only 10.8% of the respondents used condom frequently during their sexual practice. This implies that 91.2 % of the respondents were practicing premarital sex without using a condom. Key respondents from health office during interview replied that youth were not using a condom during their sexual practice because boys believe that it is not comfortable and there is no pleasure in making sex using a condom. Similarly, girls believe that making sex with a condom will have an effect on their womb.
The significant association between premarital sexual practice and prevalence rate of HIV and STDs in the study area seems due to the youth were practicing sex with multiple sexual partners without using a condom. This traditional practice mostly encourages the youth to show risky sexual behavior which causes high risk of contracting HIV and other sexually transmitted infections (STDs). This finding was also consistent with the theory which says specific customary practices and habits like resistance to the use of condoms as a result of specific sexual and cultural norms and values; social norms which allow or promote high numbers of sexual partners facilitate the spreading of STDs and HIV [9].
Most of the time parents and elders encourage premarital sexual practice in the study area. As it was stated in the above elders encourage unsafe sexual practice because they believed that it is important for relationship and marriage and the number of their ethnic group will increase through this practice. Similarly, parents also encourage this practice through motivating the boys to construct the small traditional house called “Depo” and giving sexual freedom for boys and girls.
According to the DHS-2005data the variation in prevalence of STDs and HIV across different regions of Ethiopia are because of the presence of the regional variation in sexual behavior. According to the report, areas with high STDs and HIV prevalence rates tend to exhibit a relatively high proportion of their population never married-sexually active, with a high number of sexual partners and having high-risk sexual behavior [33]. Therefore, from this, we can imply that one of the major factors for the high prevalence rate of HIV and STDs in the study area seems the presence of risky sexual behavior.
In Ethiopia, there are different traditions and cultural norms in different parts of the region. These traditions have their own degree of influence on risky sexual behavior. The main driving force for the risky sexual behavior of youth in Mengesh woreda according to the primary data collected from the study area seems traditional premarital sexual practice. Hence it is important that policy makers and researchers consider and understand these traditions in order to design effective solutions to the problem found in Gambella region.
Conclusion
The STDs have been a well-known health problem in Ethiopia for a long period of time, but due to lack of sufficient research conducted on the area the true magnitude remains unknown in Ethiopia. There were marked regional variations, in terms of the prevalence of HIV and other types of STDs in Ethiopia. The prevalence of HIV of Gambella regional state was the highest from all regions in Ethiopia which was greater than 6%. Whether one could identify specific hot spots within the region or not does not call into question, the inescapable fact that something is happening within the region to push its HIV and STDs prevalence far above the national average. Hence conducting a research and collecting data in the district level in order to identify the hot spots and communities at risk is very important to minimize regional disparities of the prevalence of HIV and STDs.
The prevalence of HIV and STDs in the study area was very high even greater than the regional average which was indicating that the importance of STDs and HIV prevention was yet to be promoted and implemented. The STDs and HIV infection were high among youth whose age between 15 and 24 in the study area. In bivariable analysis, practicing sex with multiple sexual partners, having casual sex, practicing sex without using condom, parents and elder’s response to wards premarital sexual practice were found significantly associated with the prevalence rate of STDs and HIV infection in the study area. However, the youths’ awareness towards STDs was not found a significant association with the prevalence rate of HIV and STDs. In addition to the above in multivariate analysis the variables, sexual practice with multiple sexual partners, using of a condom during sexual practice and elders’ encouragement of the traditional practice had a significant effect on the prevalence rate of HIV and STDs. Moreover, the study has shown that safe sex practices are less common as compared with the observed level of knowledge on prevention and transmission of STDs.
Generally, from this study, we can conclude that the prevalence of HIV and STDs infection among youth in the study area was relatively higher than any other parts of Ethiopia. One of the main reasons for this catastrophe according to the finding seems to be the traditional practice called premarital sex practice. This traditional practice was the main motivating factor for the occurrence of the risky sexual behavior of youth in the study area and this tradition even influences the attitude of the youth towards HIV and other STDs.
Key messages
• Among respondents 63.5% had premarital sexual practice with multiple sexual partner simply high risk for STDs.
• Only 13(8.8%) of the respondents had used condom frequently during premarital sex practice.
• The prevalence of HIV infection among the youths with age of15 to 24 years was 15.9%.
• Prevalence of HIV was high (16.8%) among girls than among boys (14.8%) from the total study participants.
Strength and Limitation of the Study
This study assesses the effect of traditional premarital sexual practice on the prevalence of HIV and other STDs which is important to develop culturally based interventional strategy in case of minimizing the HIV virus. This study had also 98% response rate. In this study area, there is high STDs and HIV prevalence and there was premarital sexual practice with multiple sexual partners. We didn’t conduct laboratory to check the HIV and STDs status of the respondents. Due to high social desirability bias, the quality of the data may be compromised. Since the study design was cross-sectional may not show cause and effect relationship.
Original protocol of study
Both probability and non-probability sampling method was applied due to the nature of the study. In probability sampling, we used simple random sampling method and from non-probability sampling, purposive sampling was used to select the three kebles and interviewees from Health office, women affairs, youth and culture and tourism office, heads and process owners and to select elders from three kebles.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
All authors read and approved the final manuscript.
Authors' contributions
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Declarations
Ethics approval and consent to participate
A letter from school of public policy of Ethiopian Civil Service University was used, to have permission of the selected offices leaders and keble leaders to collect data from youths and four office officials to collect data from the office. Prior to filling the questionnaire each of the respondents was given detail explanation about the objective and significance of the study. Then youths were asked for their informed assent to participate by explaining the fact that they had the right to decline to fill the questionnaire. In addition, the sensitive nature of the study was explained to the youth when obtaining their assent. The officials were granted about the confidentiality of the information by explaining the fact that interviews were held in private with them and no names was recorded on the individual interviews. Moreover, confidentiality on the information was kept after the completion of the interview and was not transferred to any other third party or used for any other purpose.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request both in hardcopy as well as electronics based.
References
- Organization WH UNAIDS U (2007) Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress report. Geneva: WHO.
- Organization WH (2001) Global prevalence and incidence of selected curable sexually transmitted infections: overview and estimates. Geneva: World Health Organization.
- Morison L (2001) The global epidemiology of HIV/AIDS. British Medical Bulletin 58: 7-18.
- HIV/AIDS JUNPo (2010) Global report: UNAIDS report on the global AIDS epidemic 2010: Unaids.
- Merso F (2008) Women & girls and HIV/AIDS in Ethiopia: UNFPA 2008.
- Lakew Y, Benedict S, Haile D (2015) Social determinants of HIV infection, hotspot areas and subpopulation groups in Ethiopia: evidence from the National Demographic and Health Survey in 2011. BMJ open 5: e008669.
- Chimdessa A, Olayemi O, Akpa OM (2017) Factors Associated with Vulnerability to HIV and Sexually Transmitted Infections among Street Children in Selected Towns of Ethiopia, 2016. World J AIDS 7: 230.
- HIV/AIDS. JUNPo, UNAIDS (2005) Monitoring the declaration of commitment on HIV/AIDS: guidelines on construction of core indicators: World Health Organization.
- Mswela M (2009) Cultural practices and HIV in South Africa: a legal perspective. Potchefstroom Electronic Law J Potchefstroomse Elektroniese Regsblad. 2009: 12.
- Ramjee G, Abbai NS, Naidoo S (2015) Women and sexually transmitted infections in Africa. Open Journal of Obstetrics and Gynecology 5: 385.
- Hladik W, Shabbir I, Jelaludin A, Woldu A, Tsehaynesh M, et al. (2006) HIV/AIDS in Ethiopia: where is the epidemic heading? Sexually transmitted infections 82: i32-i5.
- Mishra V, Hong R, Govindasamy P. Evaluating HIV seroprevalence estimates from Ethiopia. Further analysis of the 2005 Ethiopia Demographic and Health Survey. 2008.
- Fontanet AL, Messele T, Dejene A, Enquselassie F, Abebe A, Cutts FT, et al. Age-and sex-specific HIV-1 prevalence in the urban community setting of Addis Ababa, Ethiopia. Aids. 1998;12(3):315-22.
- Organization WH. Estimation of the incidence and prevalence of sexually transmitted infections: report of a WHO consultation, Treviso, Italy, 27 February-1 March 2002. World Health Organization, 2002.
- Alamrew Z, Bedimo M, Azage M. Risky sexual practices and associated factors for HIV/AIDS infection among private college students in Bahir Dar City, Northwest Ethiopia. ISRN Public Health. 2013;2013.
- Fortson JG. Mortality risk and human capital investment: The Impact of HIV/AIDS in Sub-Saharan Africa. The Review of Economics and Statistics. 2011;93(1):1-15.
- Tadele A, Hussen S, Shimelis T. Prevalence and associated factors of Chlamydia trachomatis and Neisseria gonorrhoeae among female commercial sex workers in Hawassa City, Southern Ethiopia. BMC infectious diseases. 2019;19(1):61.
- Tibebu M, Shibabaw A, Medhin G, Kassu A. N eisseria gonorrhoeae non-susceptible to cephalosporins and quinolones in Northwest E thiopia. BMC infectious diseases. 2013;13(1):415.
- Ali S, Sewunet T, Sahlemariam Z, Kibru G. Neisseria gonorrhoeae among suspects of sexually transmitted infection in Gambella hospital, Ethiopia: risk factors and drug resistance. BMC research notes. 2016;9(1):439.
- Federal H. AIDS Prevention and Control Office, Federal Republic of Ethiopia. Country progress report on HIV/AIDS response. Addis Ababa; 2012. 2017.
- Woldemariame SH. Factors Determining the Prevalence of HIV/AIDS in Ethiopia: Master’s Thesis in Mathematical Statistics: Stockholms universitet; 2013.
- Hrdy DB. Cultural practices contributing to the transmission of human immunodeficiency virus in Africa. Reviews of infectious diseases. 1987;9(6):1109-19.
- Gurven M, Zanolini A, Schniter E. Culture sometimes matters: Intra-cultural variation in pro-social behavior among Tsimane Amerindians. Journal of Economic Behavior & Organization. 2008;67(3-4):587-607.
- Packard RM, Epstein P. Epidemiologists, social scientists, and the structure of medical research on AIDS in Africa. Social Science & Medicine. 1991;33(7):771-83.
- Caldwell JC, Caldwell P, Quiggin P. The social context of AIDS in sub-Saharan Africa. Population and development review. 1989:185-234.
- Hemelaar J, Gouws E, Ghys PD, Osmanov S. Global and regional distribution of HIV-1 genetic subtypes and recombinants in 2004. Aids. 2006;20(16):W13-W23.
- Kenyon C. Strong associations between national prevalence of various STIs suggests sexual network connectivity is a common underpinning risk factor. BMC infectious diseases. 2017;17(1):682.
- Bogale A, Seme A. Premarital sexual practices and its predictors among in-school youths of shendi town, west Gojjam zone, North Western Ethiopia. Reproductive health. 2014;11(1):49.
- Woldemariame SH. Factors Determining the Prevalence of HIV/AIDS in Ethiopia. Masters in Mathematical Statistics, Stockholm University Stockholm; 2013.
- Gurmu E. Differentials and determinants of men’s sexual behavior in Ethiopia. Ethiopian Journal of Health Development. 2017;31(1):36-43.
- Kabeta T, Belina M, Nigatu M. HIV Voluntary Counseling and Testing Uptake and Associated Factors Among Sexually Active Men in Ethiopia: Analysis of the 2016 Ethiopian Demographic and Health Survey Data. HIV/AIDS (Auckland, NZ). 2020;12:351.
- Hook D. Foucault, disciplinary power and the critical prehistory of psychology. Critical psychology. 2004:210-38.
- Kassie GM, Mariam DH, Tsui AO. Patterns of knowledge and condom use among population groups: results from the 2005 Ethiopian behavioral surveillance surveys on HIV. BMC Public Health. 2008;8(1):429.
Artcle Information
Review Article
Received Date: May 03, 2025
Accepted Date: May 21, 2025
Published Date: May 28, 2025
Annals of Public Health and Preservative Medicine
Volume 1 | Issue 1
Citation
Demeke Demilew (2025) The Effect of Unsafe Premarital Sexual Practice on The Prevalence of HIV And Other Sexual Transmitted Diseases in Ethiopia: A Cross Sectional Study. Ann Public Health Preservative Med 1: 105
Copyright
©2025 Demeke Demilew. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: appm.2025.1.105