

Research Article
Volume-1 Issue-1, 2026
Comparison of Three Therapeutic Methods of Transcutaneous Electrical Nerve Stimulation, Embedding Acupuncture, and Drug Therapy on Interleukin-6 and Pain Levels in Patients with Knee Osteoarthritis
-
Received Date: January 05, 2026
-
Accepted Date: January 20, 2026
-
Published Date: January 23, 2026
Journal Information
Switch to Full Text Menu
Abstract
Introduction: Knee osteoarthritis, one of the most prevalent musculoskeletal disorders, affects 8.9% of the global adult population, significantly impairing their quality of life (QoL). Consequently, a definitive treatment with minimal adverse effects is urgently needed to improve these patients’ QoL. Some of the drug treatments for osteoarthritis include analgesics, non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, etc., with numerous adverse effects. Traditional Chinese Medicine (TCM) is a holistic branch of medicine and a complementary therapy to conventional medicine. Thread embedding acupuncture (TEA), a relatively new technique in acupuncture, has gained widespread use, particularly in the treatment of chronic pain conditions, such as knee osteoarthritis. TEA, as an alternative to acupuncture, a branch of TCM, has recently gained popularity. In this study, in addition to standard treatment, patients were compared in three therapeutic groups: Transcutaneous electrical nerve stimulation (TENS), TEA, and drug therapy. Furthermore, the efficacy of these treatments was evaluated by comparing interleukin-6 (IL-6) levels, pain levels, and QoL among patients.
Method: Seventy-two patients with knee osteoarthritis were selected from among individuals visiting specialized outpatient clinics at hospitals in the city of Sabzevar. After obtaining informed consent, patients were randomly assigned to three groups of 24 participants each, using the randomization software. The study was conducted in a single-blind manner. All three groups were assessed over four weeks of treatment and up to 12 weeks post-treatment. Group A received TEA, Group B received TENS, and Group C received ibuprofen, with all three groups receiving acetaminophen as well. Pain levels, QoL, and IL-6 levels were assessed at baseline, week 4, and week 12. Paired and independent samples t-tests were conducted using SPSS 16 for data analysis.
Results: Significant changes were observed in pain and QoL scores over the treatment course in both TEA and TENS groups (P < 0.001), while no significant changes were found in the classical treatment group (P=0.68). Additionally, both TENS and TEA therapies had significant impacts on IL-6 levels over time, whereas classical treatment did not induce any significant changes.
Conclusion: The three treatment methods demonstrated significant differences in pain reduction and performance improvement among patients. The TEA group exhibited superior efficacy in alleviating pain and improving QoL, and induced a greater change in IL-6 levels compared to the other two groups.
Key words
Knee Osteoarthritis, Interleukin-6, Traditional Chinese Medicine, Embedding Acupuncture
| Variable | TENS GroupMean ± SDN (%) | TEA GroupMean ± SDN (%) | Classical Treatment GroupMean ± SDN (%) | P-Value | |
| Age (year) | 57.54 ± 5.27 | 58.33 ± 6.49 | 63.92 ± 6.83 | 0.002* | |
| BMI | 25.2 ± 2.71 | 25.50 ± 1.59 | 24.60 ± 1.70 | 0.33* | |
| Gender | Male | 6 (25) | 2 (8.3) | 4 (16.7) | 0.30** |
| Female | 20 (83.3) | 22 (91.7) | 18 (75) | ||
| Time | TENS GroupMean ± SD | TEA GroupMean ± SD | Classical Treatment GroupMean ± SD | P-Value* |
| Baseline - VAS | 5.91 ± 1.21 | 5.66 ± 0.96 | 5.33 ± 1.12 | 0.19 |
| Week 4 - VAS | 4.20 ± 1.02 | 3.91 ± 1.79 | 4.83 ± 1.55 | 0.10 |
| Week 12 - VAS | 5.20 ± 1.38 | 3.91 ± 1.41 | 5.66 ± 1.73 | <0.001 |
| P-value** | <0.001 | <0.001 | 0.68 |
| Time | TENS GroupMean ± SD | TEA GroupMean ± SD | Classical Treatment GroupMean ± SD | P-Value* |
| Baseline - WOMAC | 55.12 ± 9.12 | 45.91 ± 8.06 | 48 ± 8.915 | 0.001 |
| Week 4 - WOMAC | 38.41 ± 6.72 | 30.66 ± 13.07 | 43 ± 11.19 | <0.001 |
| Week 12 - WOMAC | 43.79 ± 9.97 | 29.33 ± 10.56 | 51.70 ± 14.34 | <0.001 |
| P-value** | <0.001 | 0.001 | 0.053 |
| Time | TENS GroupMean ± SD | TEA GroupMean ± SD | Classical Treatment GroupMean ± SD | P-Value* |
| Baseline - IL | 4.39 ± 2.16 | 6.55 ± 4.19 | 7.35 ± 3.79 | 0.01 |
| Week 4 - IL | 7.47 ± 1.84 | 9.41 ± 4.54 | 7.47 ± 4.09 | 0.11 |
| Week 12 - IL | 5.21 ± 2.92 | 9.75 ± 4.54 | 6.65 ± 5.37 | 0.002 |
| P-value** | <0.001 | 0.001 | 0.42 |
| Time | TENS GroupMean ± SD | TEA GroupMean ± SD | Classical Treatment GroupMean ± SD | P-Value* |
| Baseline - QoL | 47.20 ± 9.77 | 52.16 ± 8.77 | 49.08 ± 6.76 | 0.13 |
| Week 4 - QoL | 57.75 ± 7.42 | 67.41 ± 13.52 | 51.41 ± 12.41 | <0.001 |
| Week 12 - QoL | 52.41 ± 11.32 | 65.00 ± 12.08 | 47.83 ± 12.65 | <0.001 |
| P-value** | <0.001 | <0.001 | 0.33 |
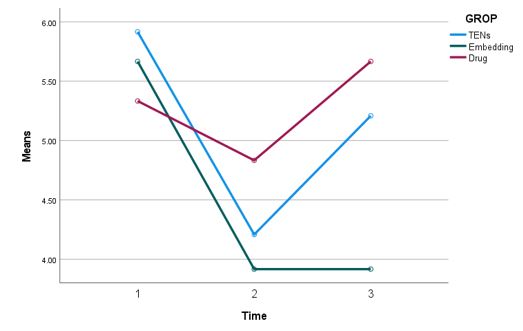 |
| Figure 1: Comparison of mean pain scores at baseline, week 4, and week 12 across study groups |
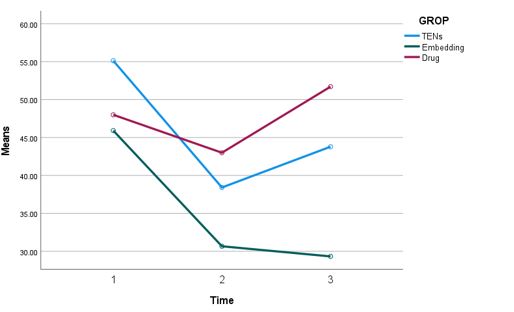 |
| Figure 2: Comparison of mean Western Ontario and McMaster Universities [WOMAC] Osteoarthritis Index Scores at baseline, week 4, and week 12 based on the study groups |
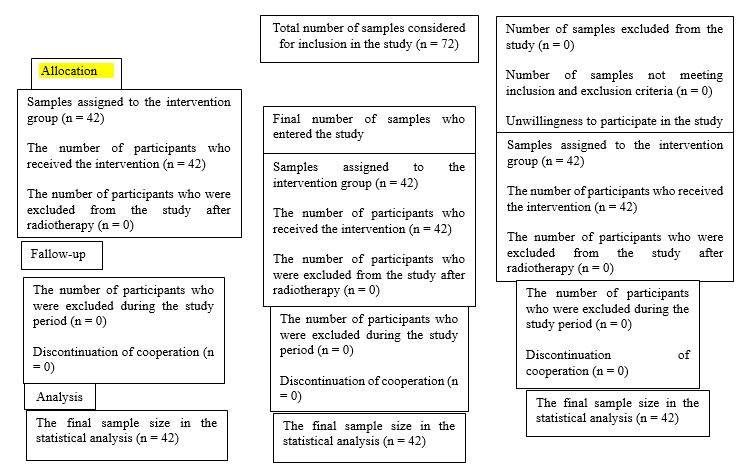 |
| Figure 3: The clinical trial process based on the Consolidated Standards of Reporting Trials (CONSORT) Statement |
Introduction
Knee osteoarthritis, one of the most prevalent musculoskeletal disorders, affects 8.9% of the global adult population [1,2]. In Iran, the prevalence of knee osteoarthritis has also been reported to be between 9.76% and 19.3% in urban and rural areas, respectively (3, 5). These statistics underscore the high prevalence of this disorder both worldwide and in Iran (1 in every 6.5 individuals) [3]. According to a recent report by the World Health Organization (WHO), the number of individuals over 65 years of age afflicted with this disease is 17%, imposing an annual cost of €4.5 billion on the healthcare system [4].
In a study SHI et al.’s study, the prevalence of symptomatic knee osteoarthritis in the United States was reported to be 7% [5]. Additionally, another meta-analysis reported a prevalence of 14.6% for symptomatic knee osteoarthritis in China [6]. In a study, MAXINE estimated the lifetime prevalence of disabling symptomatic knee osteoarthritis to be between 14% and 45% across different groups [7].
Osteoarthritis can affect any joint in the body, but it is most commonly found in the joints of the hands, knees, hips, and spine [8,9]. Common symptoms of knee osteoarthritis include pain, stiffness, decreased range of motion, and swelling [1,2,10]. A study revealed that 69.5% of patients with knee osteoarthritis were aged 60 years and above, with 63% of them being women. Overweight, with its metabolic effects and excessive pressure on the joints, leads to the development of osteoarthritis or degenerative joint disease. Genetics also contributes to the development of this disease [2,7,9]. Inflammation plays a substantial role in the pathogenesis of knee osteoarthritis, and pro-inflammatory cytokine markers, such as Tumor necrosis factor-alpha (TNF-α), IL-1 beta (IL-1β), and IL-6, are elevated in the blood at least five years before the onset of radiological signs of the disease, impact the function of the joint surrounding nerves and muscles, and consequently lead to pain [11]. As a result of inflammation, cytokines contribute to cartilage degeneration [12,13]. Changes in IL-6 levels are a significant basis for the treatment of rheumatoid arthritis, juvenile idiopathic arthritis, giant cell arteritis, etc. [14]. The synovium of the infrapatellar fat pad (IFP) is a major source of IL-6, and inflammation in this synovium culminates in an increase in IL-6. The present study delves into the role of IL-6 as a critical factor in the dynamic equilibrium of osteoarthritis pathology and explores therapeutic approaches targeting IL-6 alteration signaling.
In classical medicine, knee pain is attributed to osteoarthritis, rheumatoid fever, rheumatoid arthritis, injuries to the internal and external ligaments, etc. [15]. However, from the perspective of traditional Chinese medicine (TCM), pathogens are categorized into two main groups: External and internal. It is believed in TCM that joint pain is attributed to attacks from wind, heat, cold, or damp: Wind stems from the liver dysfunction; heat corresponds to inflammation in classical medicine; cold is equivalent to decreased basal metabolism in classical medicine; and damp is indicative of pathological fluid in classical medicine. Deficiencies in organs, particularly the liver, kidneys, or stagnation in Qi and blood, can also cause joint pain.
Excessive stress, chronic illness, and advanced age can give rise to a deficiency in liver and kidney energy. Due to this deficiency, tendons are not adequately nourished by the liver, and bones are not properly nourished by the kidneys, culminating in pain [15].
Numerous therapeutic approaches exist for the management of knee osteoarthritis, including physical therapy, weight loss, the use of analgesics and non-steroidal anti-inflammatory drugs (NSAIDs), etc. However, long-term use of these medications causes a multitude of adverse effects, such as gastrointestinal ulcers, sleep disturbances, drug dependence, and an increased risk of cardiovascular and cerebrovascular events [2,10,6]. Approximately $7 billion is spent annually around the world on the use of NSAIDs for osteoarthritis treatment. Thus, the use of a method with no adverse effects, such as complementary medicine, could be extremely beneficial in reduce inflammation, pain and managing this condition [17,18]. The WHO has declared osteoarthritis among the illnesses for which the efficacy of acupuncture has been confirmed in clinical trials, [19,20]. Thread embedding acupuncture (TEA), a specific form of acupuncture involving the placement of absorbable threads subcutaneously for long-term therapeutic effects, is derived from cutgut-embedding and is one of the newest and extensively used acupuncture techniques [21]. Research has demonstrated that stimulating acupuncture points culminates in changes in opioid and endocrine levels [8,21]. In a meta-analysis, wei et al. reported a positive impact of acupuncture in the treatment of musculoskeletal pains [21]. Shi et al. also reported a significant effect of acupuncture in the treatment of knee osteoarthritis [5]. Compared to acupuncture, TEA can produce a more potent and long-lasting effect. A controlled clinical trial in China proved that TEA was more effective than acupuncture in treating frozen shoulder and intervertebral disc herniation [22].
The most precise method for determining the efficacy of various treatments in improving knee osteoarthritis is by measuring inflammatory factors in the bloodstream before and after treatment [23]. The current study aimed to compare the effectiveness of three therapeutic approaches: TENS, TEA, and drug therapy, on IL-6 and pain levels in patients with knee osteoarthritis. Given the heavy healthcare and economic burden imposed by this disease, conducting such research appears to be essential for developing effective treatment strategies.
Method
The present research is an experimental study of a randomized controlled trial (RCT) type. The study population consisted of all individuals with knee osteoarthritis referring to the outpatient clinics at hospitals in the city of Sabzevar. In this study, 72 people from the study population who had the characteristics of the research units were regarded as the research sample. Sample size was calculated based on previous studies [5] using G*Power software. Considering a 95% confidence level, a test power of 85%, and a large effect size of 0.4, a total sample size of 72 participants (24 participants per group) was determined for this study (α = 5%, confidence level (1- α) = 95%, test power (1-β) = 15%, effect size = 4.0). Consequently, a sample size of 24 participants per group was determined, considering a 10% dropout rate. These patients were diagnosed with osteoarthritis based on a Kellgren-Lawrence score of 2-3 and a Visual Analogue Scale (VAS) pain score of higher than/equal to 4 to lower than/equal to 7 (indicating moderate pain level).
In this study, 72 eligible patients were selected from among the target population and were randomly assigned to three equal groups (n = 24) after providing written informed consent. Simple randomization using coded envelopes, which were opened at the beginning of the treatment, was employed to allocate participants to either Group A (TENS), Group B (TEA), or Group C (drug therapy).
This study was single-blind. All three groups underwent treatment for 4 weeks and were followed up for 12 weeks post-treatment. Group A received TEA. TEA in these patients was performed using polydioxanone (PDO) threads, size 0, with yellow 20-gauge needles (Vekto), and blue angiocatheters (Alborz) as guides. Initially, anesthesia was performed using 5% lidocaine ointment, and after 20 minutes, the ten-point locations (ST-36-----GB-34-----ST-44-----ST-35-----LI4----- SP-9-----SP-10-----KID-3-----ST-34 - -- EX-LE2) were sterilized and embedding (thread placement) was carried out for one session. It is worth noting that cephalexin 500 mg capsules were prescribed as prophylaxis for all patients for 2 days. Group B underwent high-frequency TENS (Arman Pouya Company) 4 times a week, each time 30 minutes, for 4 weeks, with 50-100 Hz using an Med400 device.
Group C received 400 mg of ibuprofen (Dana Pharmaceutical Company) twice daily for 4 weeks. It is important to note that all patients also received one 325 mg acetaminophen (Jalinus) tablet daily.
IL-6, pain (measured using the VAS), knee limited range of motion (measured using the Western Ontario and McMaster Universities [WOMAC] Osteoarthritis Index), and quality of life (QoL) (measured using the WHOQoL - Brief Version [WHOQOL-BREF] questionnaire) [24] were assessed at baseline (before the study) to determine the initial status of patients, and were also measured as baseline. These measures were reassessed 4 weeks after the completion of treatment to evaluate the efficacy of various treatment methods in reducing pain levels and limited range of motion associated with knee osteoarthritis, to examine pain levels and limited range of motion, and to assess IL-6 levels and QoL.
In week 12, all variables were explored and measured to assess treatment methods in the long run. It is worth noting that in order to determine and analyze IL-6 levels, 0.5 cc of venous blood was collected from all participants. The blood samples were transferred to (EDTA) tubes, maintained in a cold chain, and transported to the immunology laboratory. IL-6 levels were then measured using an IMMULITE 2000 XPi device (Siemens Company).
Inclusion criteria included patients diagnosed with knee osteoarthritis according to the American College of Rheumatology (ACR) criteria, aged 50-65 years, with involvement of only one knee, a VAS pain score of higher than/equal to 4 and lower than 8, reading and writing literacy, and willingness to participate in the study.
Non-inclusion criteria consisted of involvement of both knees, a history of or candidacy for knee joint surgery, a history of knee arthroscopy within the past year, any therapeutic interventions (such as intra-articular injections or acupuncture) within the past six months, any disease that impairs the immune system (such as autoimmune diseases, connective tissue diseases, diabetes, cancer, etc.) or severe physical (epilepsy, peptic ulcer, etc.) or psychological and cognitive diseases that prevent continued cooperation, the presence of a pacemaker, a body mass index (BMI) greater than 30 and addiction to drugs or alcohol. Exclusion criteria comprised non-cooperation during the study, development of infectious or inflammatory diseases during the study (such as coronavirus disease 2019 [COVID-19], influenza, inflammatory and skin diseases of the knee and surrounding area), and any mandatory changes to the treatment regimen.
The Kellgren-Lawrence scale, a commonly used grading tool, quantifies the severity of osteoarthritis by measuring joint space narrowing, osteophyte formation, and subchondral sclerosis on a 0 to 4 scale [25].
The WOMAC index, a commonly used in clinical settings to reflect the severity of the disease, allows for a reliable assessment of the degree of damage, pain, and loss of function [26]. This index is the most widely used specific tool for assessing osteoarthritis of the hip or knee joint, which is also recommended in clinical trials.
The WOMAC index is classified to measure dysfunction and pain associated with lower limb osteoarthritis by assessing 17 functional activities, five pain-related activities, and two stiffness-related categories [27].
The VAS, a common tool for measuring pain severity, is a method used to analyze and measure outcomes. In this tool, a 100 mm line is presented with the endpoints labeled ‘no pain’ and ‘worst possible pain.’ Patients mark on the line to indicate their perceived pain severity, ranging from the left endpoint to the right endpoint [28].
Descriptive and inferential statistics were employed for data analysis. Data were described using frequency tables, coupled with mean, standard deviation, median, and interquartile range indices. For analytical section, the paired and independent samples t-tests were used for normally distributed data, while Wilcoxon and Mann-Whitney U tests were employed for non-normally distributed data. Analysis of covariance (ANCOVA) was used to control for confounding variables. Data were analyzed using SPSS version 16, and the significance level was set at 0.05.
Results
Demographic Characteristics
The demographic variables of the participants are summarized in Table 1. The mean age was significantly higher in the classical treatment group (63.92 ± 6.83 years) compared to the TEA (58.33 ± 6.49 years) and TENS groups (57.54 ± 5.27 years) (P = 0.002). There was no significant difference in BMI among the groups (P = 0.33), with mean values of 24.60 ± 1.70, 25.50 ± 1.59, and 25.20 ± 2.71 kg/m2 for the classical, TEA, and TENS groups, respectively. Gender distribution did not differ significantly (P = 0.30). Baseline demographic characteristics were well-balanced across the groups, except for age, which was accounted for in subsequent analyses.
Pain Severity (Visual Analogue Scale [VAS] Scores)
Baseline pain scores were similar across the groups (P = 0.19), as shown in Table 2 and Figure 1, with mean values of 5.33 ± 1.12, 5.66 ± 0.96, and 5.91 ± 1.21 in the classical, TEA, and TENS groups, respectively. By week 12, a significant reduction in pain severity was observed in the TEA group (3.91 ± 1.41), compared to the classical (5.66 ± 1.73) and TENS (5.20 ± 1.38) groups (P < 0.001). Within-group analysis revealed a significant reduction over time for the TEA and TENS groups (P < 0.001), while no significant change was observed in the classical group (P=0.68). ANCOVA, controlling for baseline VAS scores, confirmed that the TEA group achieved the greatest pain reduction (F=17.1, P < 0.001).
Functional Disability (The Western Ontario and McMaster Universities [WOMAC] Osteoarthritis Index Scores)
The WOMAC scores at baseline were highest in the TENS group (55.12 ± 9.12), followed by the classical (48.00 ± 8.91) and TEA groups (45.91± 8.06) (P = 0.001). As shown in Table 3 and Figure 2, significant improvements were observed in all groups by week 4, with the TEA group exhibiting the largest reduction (30.66 ± 13.07). At week 12, the TEA group maintained the greatest improvement (29.33 ± 10.56), whereas the TENS (43.79 ± 9.97) and classical (51.70 ± 14.34) groups demonstrated less pronounced changes (P < 0.001). Repeated-measures ANCOVA showed that the TEA group consistently outperformed the other groups, with the effect being independent of baseline WOMAC scores (F=6.703, P=0.002).
Serum Interleukin-6 Levels
Baseline IL-6 levels differed significantly between groups (P = 0.01), with the highest levels in the classical group (7.35 ± 3.35 pg/mL), followed by TEA (6.55 ± 4.19 pg/mL) and TENS (4.39 ± 2.16 pg/mL). At week 4, no significant differences were detected among the groups (P = 0.11); however, by week 12, the TEA group exhibited the largest reduction (9.75 ± 4.54 pg/mL), followed by TENS (5.21 ± 2.92 pg/mL), while the classical group showed no significant change (P = 0.42). As highlighted in Table 4, ANCOVA revealed significant time-by-treatment interactions (F = 4.996, P = 0.009) and confirmed that the TEA treatment yielded the greatest reduction in IL-6 levels.
Quality of Life (QoL)
As presented in Table 5, baseline QoL scores did not differ significantly among the groups (P = 0.13), with mean values of 49.08 ± 6.76, 52.16 ± 8.77, and 47.20 ± 9.77 for the classical, TEA, and TENS groups, respectively. By week 4, the TEA group showed the greatest improvement in QoL (67.41 ± 13.52), which was sustained through week 12 (65.00 ± 12.08). In comparison, the TENS and classical groups demonstrated lesser improvements, with final scores of 52.41 ± 11.32 and 47.83 ± 12.65, respectively (P < 0.001). ANCOVA confirmed that these improvements were significantly associated with the type of treatment, independent of baseline QoL scores (F=17.889, P < 0.001).
Discussion
Given the significance of inflammation control and its role in improving the clinical and psychological conditions of patients, this study was designed to compare the efficacy of classical, TEA, and TENS treatment methods. Data analysis revealed significant differences in IL-6 levels and QoL over time, as well as across the different treatment groups. Notably, the TEA treatment method demonstrated remarkable results in terms of IL-6 levels, pain control, and improved QoL, suggesting its potential as an effective approach in clinical management.
A study conducted by tian et al. (2022) revealed that non-pharmacological methods, such as acupuncture, were more effective in alleviating pain, particularly in long-term follow-ups, compared to pharmaceutical treatments. These findings align with the present study results, where the TEA method demonstrated a significantly greater pain reduction at week 12 compared to the other two methods [29].
Vance CGT et al.’s study(2012) demonstrated a positive effect of the TENS technique on pain reduction, corroborating the findings of this study, particularly in the TEA and TENS groups [30].
Oluwaf et al.’s study (2012) indicated that drug therapies, such as NSAIDs, only provide temporary and short-term pain relief and have a lesser effect in long-term follow-ups. These results align with the findings of the present study, which indicated that classical drug therapy had no significant impact on reducing pain over time [31].
Diller ML et al. (2023) indicated that non-pharmacological methods, such as cryotherapy and acupuncture, can be beneficial in managing symptoms and improving the QoL of patients experiencing acute and chronic pains [32].
Dailey DL et al 2022 confirmed the efficacy and feasibility of adding TENS to conventional physical therapy in patients with fibromyalgia (FM). Their findings aligned with our study's results, as both emphasized the positive impact of TENS on pain relief [33]. David Beckwée et al.’s article (2022) suggested that both TEA and acupuncture groups exhibited significant improvements in pain assessment scores. Moreover, our study indicates that the TEA method yielded better outcomes compared to the other two methods [34]. A study conducted by Majnik et al. (2022) demonstrated a positive impact of non-pharmacological treatments on reducing interleukin levels in patients with arthritis. The findings of this study suggest that non-pharmacological interventions, particularly in the early stages of arthritis, can contribute to reducing inflammation levels and improving patients’ QoL [35]. Helmark et al. (2010) demonstrated that the application of physical therapy and electrical stimulation techniques can significantly reduce interleukin levels, thereby alleviating pain and improving patient outcomes [36]. In another study conducted by Tomazoni et al. (2017), the impacts of combined therapies on interleukin levels in patients with knee osteoarthritis were investigated. This study demonstrated that a combination of physical and drug therapies could significantly reduce IL-6 and IL-1β levels, ultimately culminating in improved function and pain reduction in patients [37]. The results of these studies were inconsistent with our research.
Resnik et al. (2020) indicated that the elevated IL-6 levels in the synovial fluid and serum of patients with osteoarthritis was inversely correlated with pain severity and joint damage.This article highlights that under conditions of elevated IL-6 levels, classical IL-6 signaling in articular tissues can exert protective effects and contribute to reduced structural damage. In other words, although IL-6 is recognized as an inflammatory molecule, under certain circumstances, it can contribute to maintaining cartilage health and alleviating pain in patients with osteoarthritis. In this regard, precise regulation of IL-6 levels and control of its signaling activities may represent an effective therapeutic strategy for managing pain and inflammation in patients with arthritis, which aligns with our findings of increased IL-6 levels [38].
Hadjistavropoulos et al. (2019) demonstrated that novel methods, such as TEA, effectively improved function and reduced pain levels [40]. Lastly, El-Tallawy et al. (2021) reported comparable results in a study comparing traditional and novel treatments for pain relief and functional improvement [41].
Overall, the results of this study denote the positive and sustained impacts of the TEA method in alleviating pain, improving function, decreasing interleukin levels, and enhancing QoL in patients compared to two other treatment methods (TENS and classical treatment).
Ultimately, the lack of a significant interaction effect between age and baseline interleukin levels with changes in interleukin levels over time (P = 0.562) indicates that the efficacy of these treatments was independent of these factors. In other words, the observed differences in interleukin levels were primarily attributable to the type of treatment, and factors such as age or initial levels of inflammation did not significantly affect the final outcomes.
Studies have revealed that IL-6 assists in regulating immune and inflammatory responses, and can stimulate the production of anti-inflammatory cytokines, ultimately leading to pain reduction [42]. Additionally, IL-6 contributes to tissue repair and wound healing processes, and can enhance growth factors and tissue regeneration factors [14]. These findings align with our results, suggesting that increased IL-6 levels may positively impact pain relief in patients with knee osteoarthritis.
Rouhi et al.’s research (2020) highlights the importance of pain reduction-based interventions in improving QoL [43], which aligns with the findings of this study. Finally, Wojcieszek et al.’s study (2022) explored the link between daily activities and QoL in patients with knee osteoarthritis, demonstrating that increased physical and social activities led to significant improvements in their QoL [44]. These results further underscore the importance of viewing QoL as a primary goal of clinical interventions.
Conclusion
The results of this research revealed a significant difference between the TENS and TEA treatment methods in alleviating pain and improving patient function (QoL). While there was no significant difference across the groups in terms of pain at the beginning of the study, over time, the TEA method, particularly at week 12, had a significantly greater effect on pain relief compared to TENS. Overall, the findings indicate that the TEA method was more effective and sustained compared to the other two methods. The positive impact of the TEA group on interleukin levels and patients’ QoL suggests a high potential for this method in improving patients’ health. Given the positive and effective impact of TEA, this treatment appears to be effective in treating osteoarthritis pain in other joints of the body as well.
Limitations
Limited sample size and short follow-up duration were some limitations of this study. Future research is recommended with a larger sample size and longer follow-up period to assess the long-term effects of various treatment methods on QoL and interleukin levels.
References
- Hunter and Bierma-Zeinstra (2019) Hunter, D. J., and S. Bierma-Zeinstra. 2019. 'Osteoarthritis', Lancet, 393: 1745-59.
- Jordan, KM, NK Arden, M Doherty, B Bannwarth, JW Bijlsma, P Dieppe, et al. (2003) 'EULAR Recommendations 2003: an evidence-based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT)', Ann Rheum Dis, 62: 1145-55.
- Jalali Jeivan S, Asadi T, Shariati Z, Tavakol Afshari J, Ghasemi A, Hamidi Alamdari D (2015) Platlete-Rich plasma. medical journal of mashhad university of medical sciences. 58: 74-9.
- Allen KD, Thoma LM, Golightly YM (2022) Epidemiology of osteoarthritis. Osteoarthritis and cartilage. 30: 184-95.
- Shi, Guang-Xia, Jian-Feng Tu, Tian-Qi Wang, Jing-Wen Yang, Li-Qiong Wang, Lu-Lu Lin, Yu Wang, Yong-Ting Li, and Cun-Zhi Liu. (2020) 'Effect of electro-acupuncture (EA) and manual acupuncture (MA) on markers of inflammation in knee osteoarthritis', Journal of Pain Research: 21: 71-9.
- Tian, Hao, Liuyang Huang, Mingsheng Sun, Guixing Xu, Jiamei He, Zhuo Zhou, Fengyuan Huang, Yilin Liu, and Fanrong Liang. (2022) '[Retracted] Acupuncture for Knee Osteoarthritis: A Systematic Review of Randomized Clinical Trials with Meta‐Analyses and Trial Sequential Analyses', BioMed Research International, 2022: 6561633.
- Papadakis, Maxine A, Stephen J McPhee, and Michael W Rabow (2019) Current medical diagnosis and treatment (Mc. Graw-Hill).
- Breedveld FC (2004) Osteoarthritis--the impact of a serious disease. Rheumatology (Oxford) 2004; 43Suppl 1: i4-8.
- Kerkhof HJ, Bierma-Zeinstra SM, Arden NK, et al. (2014) Prediction model for knee osteoarthritis incidence, including clinical, genetic and biochemical risk factors. Ann Rheum Dis. 73: 2116-21.
- Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines'. 2000. Arthritis Rheum, 43: 1905-15.
- Laine L (2003) 'Gastrointestinal effects of NSAIDs and coxibs', J Pain Symptom Manage, 25: S32-40.
- Kapoor, Mohit, Johanne Martel-Pelletier, Daniel Lajeunesse, Jean-Pierre Pelletier, and Hassan Fahmi (2011) 'Role of proinflammatory cytokines in the pathophysiology of osteoarthritis', Nature Reviews Rheumatology, 7: 33-42.
- Berenbaum F (2013) 'Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!)', Osteoarthritis Cartilage, 21: 16-21.
- Kang, Sujin, Toshio Tanaka, Masashi Narazaki, and Tadamitsu Kishimoto (2019) 'Targeting interleukin-6 signaling in clinic', Immunity, 50: 1007-23.
- PEILIN, SUN. (2002) THE TREATMEANT OF PAIN WITH CHIENES HERBS AND ACUPUNCTURE.
- Zhao HY, S Kim, MJ Son (2022) 'Comparing acupoint catgut embedding and acupuncture therapies for simple obesity: A protocol for systematic review and meta-analysis', Medicine (Baltimore), 101: e31531.
- Moghadam MY, Nemat-Shahi M, Soroosh D, Nemat-Shahi M, Asadi A (2020) Effect of evening primrose oil on postoperative pain after appendectomy: A double-blind, randomized, clinical trial. Biomedicine (Taipei). 10: 28-32.
- Bijlsma JW, Berenbaum F, Lafeber FP (2011) Osteoarthritis: an update with relevance for clinical practice. Lancet. 377: 2115–26
- Felson, David T (2006) 'Osteoarthritis of the knee', New England Journal of Medicine, 354: 841-48.
- Guo, Jing, Yang Chen, Zhengjie Li, Shirui Cheng, Chenjian Tang, Xiaohui Dong, Wenhua He, Yong Huang, Bao Yin, and Yu Sheng. (2019) 'The cerebral mechanism of acupuncture for treating knee osteoarthritis: study protocol for a randomized controlled trial', Trials, 20: 1-10.
- Wei, Ying, Nairong Yuan, Jiru Ding, Lixia Wang, Yan Dong, Lu Deng, and Qi Yang. (2020) 'Efficacy and safety of warm needle acupuncture in knee osteoarthritis: a protocol for systematic review and meta-analysis', Medicine (Baltimore), 99: e23596.
- Huo, J., J. Zhao, Y. Yuan, J Wang (2017) '[Research status of the effect mechanism on catgut-point embedding therapy]', Zhongguo Zhen Jiu, 37: 1251-4.
- Wiegertjes, Renske, Fons AJ van de Loo, Esmeralda N Blaney Davidson (2020) 'A roadmap to target interleukin-6 in osteoarthritis', Rheumatology, 59: 2681-94.
- Nejat Saharnaz, Montazeri Ali, Holakoui Naini Kourosh, Mohammad Kazem, Majdzadeh Seyed Reza (2006) Standardization of the World Health Organization Quality of Life Questionnaire (WHOQOL-BREF): Translation and Psychometric Evaluation of the Iranian Version. Journal of the School of Public Health and Health Research Institute. 4: 1-12.
- Olsson, Simon, Ehsan Akbarian, Anna Lind, Ali Sharif Razavian, Max Gordon (2021) 'Automating classification of osteoarthritis according to Kellgren-Lawrence in the knee using deep learning in an unfiltered adult population', BMC Musculoskeletal Disorders, 22: 1-8.
- Michael, Joern W-P, Klaus U Schlüter-Brust, Peer Eysel (2010) 'The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee', Deutsches Arzteblatt International, 107: 152.
- Salaffi, Fausto, G Leardini, B Canesi, A Mannoni, A Fioravanti, R obo Caporali, Giovanni Lapadula, and L Punzi. (2003) 'Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in Italian patients with osteoarthritis of the knee', Osteoarthritis Cartilage, 11: 551-60.
- Heller, Gillian Z, Maurizio Manuguerra, Roberta Chow (2016) 'How to analyze the Visual Analogue Scale: Myths, truths and clinical relevance', Scandinavian journal of pain, 13: 67-75.
- Tian H, Huang L, Sun M, Xu G, He J, Zhou Z, et al. (2022) [Retracted] Acupuncture for Knee Osteoarthritis: A Systematic Review of Randomized Clinical Trials with Meta‐Analyses and Trial Sequential Analyses. BioMed Research International. 2022: 6561633.
- Vance CGT, Rakel BA, Blodgett NP, DeSantana JM, Amendola A, Zimmerman MB, et al. (2012) Effects of transcutaneous electrical nerve stimulation on pain, pain sensitivity, and function in people with knee osteoarthritis: a randomized controlled trial. Physical therapy. 92: 898-910.
- Reichenbach S, Jüni P, Hincapié CA, Schneider C, Meli DN, Schürch R, et al. (2022) Effect of transcutaneous electrical nerve stimulation (TENS) on knee pain and physical function in patients with symptomatic knee osteoarthritis: the ETRELKA randomized clinical trial. Osteoarthritis and cartilage. 30: 426-35.
- Oluwafisayo AJ, Mlenzana NB, Shamila M, Nesto T, Grace M (2014) Side effects of non-steroidal anti-inflammatory drugs: The experience of patients with musculoskeletal disorders. Am J Public Health Res. 2: 106-12.
- Diller ML, Master V (2023) Integrative surgery: embedding complementary and nonpharmacologic therapies into surgical pain management strategies. The American Surgeon. 89: 192-6.
- Beckwée D, De Hertogh W, Lievens P, Bautmans I, Vaes P (2012) Effect of TENS on pain in relation to central sensitization in patients with osteoarthritis of the knee: study protocol of a randomized controlled trial. Trials. 13: 1-7.
- Majnik J, Császár-Nagy N, Böcskei G, Bender T, Nagy G (2022) Non-pharmacological treatment in difficult-to-treat rheumatoid arthritis. Frontiers in Medicine. 9: 991677.
- Helmark IC, Mikkelsen UR, Børglum J, Rothe A, Petersen MCH, Andersen O, et al. (2010) Exercise increases interleukin-10 levels both intraarticularly and peri-synovially in patients with knee osteoarthritis: a randomized controlled trial. Arthritis research & therapy. 12: 1-11.
- Tomazoni SS, Leal-Junior ECP, Pallotta RC, Teixeira S, de Almeida P, Lopes-Martins RÁB (2017) Effects of photobiomodulation therapy, pharmacological therapy, and physical exercise as single and/or combined treatment on the inflammatory response induced by experimental osteoarthritis. Lasers in medical science. 32: 101-8.
- Renske Wiegertjes, Fons A J van de Loo, Esmeralda N Blaney Davidson (2020) A roadmap to target interleukin-6 in osteoarthritis, Rheumatology, 59: 2681–94.
- Hadjistavropoulos T, Makris UE (2022) Pain in older adults: a brief clinical guide. Clinical Pain Management: A Practical Guide. 9: 419-31.
- El-Tallawy SN, Nalamasu R, Salem GI, LeQuang JAK, Pergolizzi JV, Christo PJ (2021) Management of musculoskeletal pain: an update with emphasis on chronic musculoskeletal pain. Pain and therapy. 10: 181-209.
- Wiegertjes R, van de Loo FAJ, Blaney Davidson EN (2020) A roadmap to target interleukin-6 in osteoarthritis. Rheumatology. 59: 2681-94.
- Gatchel RJ, McGeary DD, McGeary CA, Lippe B (2014) Interdisciplinary chronic pain management: past, present, and future. American psychologist. 69: 119.
- Rouhi S, Dadkhah P, Firoozi M, Hashemi M (2020) New model for couple therapy for patients with chronic pain and their caregivers: An attempt to improve quality of life and reduce pain. Clinical Practice and Epidemiology in Mental Health: CP & EMH. 16: 53.
- Wojcieszek A, Kurowska A, Majda A, Liszka H, Gądek A (2022) The impact of chronic pain, stiffness and difficulties in performing daily activities on the quality of life of older patients with knee osteoarthritis. International journal of environmental research and public health. 19: 16815.
Article Information
Research Article
Received Date: January 05, 2026
Accepted Date: January 20, 2026
Published Date: January 23, 2026
Comparison of Three Therapeutic Methods of Transcutaneous Electrical Nerve Stimulation, Embedding Acupuncture, and Drug Therapy on Interleukin-6 and Pain Levels in Patients with Knee Osteoarthritis
Volume 1 | Issue 1
Citation
Bahrami Hamidreza (2026) Comparison of Three Therapeutic Methods of Transcutaneous Electrical Nerve Stimulation, Embedding Acupuncture, and Drug Therapy on Interleukin-6 and Pain Levels in Patients with Knee Osteoarthritis. J Traditional Complement Altern Med 1:102
Copyright
©2026 Bahrami Hamidreza. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jtca.2026.1.102