

Research Article
Volume-1 Issue-1, 2026
Effects of Acupuncture on Immunoregulation During Prolonged High-Intensity Training Session in Soccer Players
-
Received Date: February 08, 2026
-
Accepted Date: February 18, 2026
-
Published Date: February 21, 2026
Journal Information
Switch to Full Text Menu
Abstract
Objective: This paper aims at estimating the effect of acupuncture therapy on modulate immune parameters during prolong high-intensity training in soccer players.
Method: 28 healthy male soccer players were recruited and randomly divided two groups, acupuncture group (AG) and sham acupuncture group (SG). All subjects had executed prolong, high-intensity training last 4 weeks. Acupuncture therapy had been implemented 3 times every week on bilateral Zusanli (ST 36), Hegu (LI 4), Shenshu (BL 23), and Chize (LU 5), therapy 12 times together. A special “placebo-needle” had been utilized in SG. During pre-test and post-test, used flow cytometry method and Enzyme-Linked ImmunoSorbent Assay (ELISA) method test T-lymphocyte (CD3+, CD4+, CD8+, CD4/CD8), and interleukin (Il-6, IL-10), respectively.
Results: Compare pre-test to post-test, T lymphocyte (CD3+), T helper (CD4+), T cytotoxic/suppressor (CD8+), the IL-6, and the IL-10 have significant difference in sham group (SG), but just IL-6 has a statistical significance in acupuncture therapy group (AG); compare AG to SG, just IL-6 and IL-10 have significant difference.
Conclusion: Prolong, high-intensity training session in soccer players cause by decreased immune functions, increase level of pro-and anti-inflammatory cytokines. Acupuncture therapy could facilitate to restore immune function, inhibition the soccer player’s immunity to further reduce.
Key words
Acupuncture; Sports Fatigue; Physical Therapy; Immunoregulation
|
AG (n=12) |
SG (n=12) |
p |
Age (years) |
21.75±1.76 |
21.75±1.78 |
0.82 |
Weight (kg) |
70.82±4.83 |
72.08±4.99 |
0.534 |
Height (cm) |
176.93±6.97 |
175.44±4.23 |
0.535 |
Training (years) |
6.00±1.31 |
6.46±1.59 |
0.45 |
CD3+ (%) |
70.92±6.95 |
72.88±3.23 |
0.388 |
CD4 (%) |
37.37±6.05 |
38.86±7.03 |
0.874 |
CD8 (%) |
27.79±6.96 |
28.20±5.39 |
0.583 |
IL-6 (pg/ml) |
1.43±0.15 |
1.44±0.23 |
0.87 |
IL-10 (pg/ml) |
3.79±0.70 |
3.71±0.47 |
0.918 |
|
|
AG (n=12) |
|
|
|
SG (n=12) |
|
|
Pre |
Post |
P |
|
Pre |
Post |
P |
CD3+% |
70.92±6.95 |
71.29±6.06 |
0.786 |
|
72.88±3.23 |
69.76±3.21 |
0.025* |
CD4+ % |
37.95±5.53 |
37.44±6.32 |
0.945 |
|
39.11±7.11 |
35.44±6.35 |
0.013* |
CD8+ % |
27.79±6.96 |
29.58±7.54 |
0.057 |
|
28.20±5.39 |
30.40±5.04 |
0.002** |
CD4/CD8 |
1.44±0.44 |
1.36±0.45 |
0.172 |
|
1.47±0.48 |
1.25±0.40 |
0.023* |
IL-6 pg/ml |
1.43±0.15 |
1.55±0.17 |
0.049* |
|
1.38±0.30 |
1.85±0.35 |
0.001** |
IL-10 pg/ml |
3.76±0.69 |
3.87±0.53 |
0.333 |
|
3.79±0.67 |
4.33±0.48 |
0.009** |
|
|
Pre |
|
|
|
Post |
|
|
AG (n=12) |
SG (n=12) |
P |
|
AG (n=12) |
SG (n=12) |
P |
CD3+% |
70.92±6.95 |
72.88±3.23 |
0.388 |
|
71.29±6.06 |
69.76±3.21 |
0.449 |
CD4+ % |
37.95±5.53 |
39.11±7.11 |
0.661 |
|
37.44±6.32 |
35.44±6.35 |
0.447 |
CD8+ % |
27.79±6.96 |
28.20±5.39 |
0.874 |
|
29.58±7.54 |
30.40±5.04 |
0.759 |
CD4/CD8 |
1.44±0.44 |
1.47±0.48 |
0.885 |
|
1.36±0.45 |
1.25±0.40 |
0.567 |
IL-6 pg/ml |
1.43±0.15 |
1.38±0.30 |
0.722 |
|
1.55±0.17 |
1.85±0.35 |
0.019* |
IL-10 pg/ml |
3.76±0.68 |
3.79±0.67 |
0.905 |
|
3.87±0.53 |
4.33±0.48 |
0.037* |
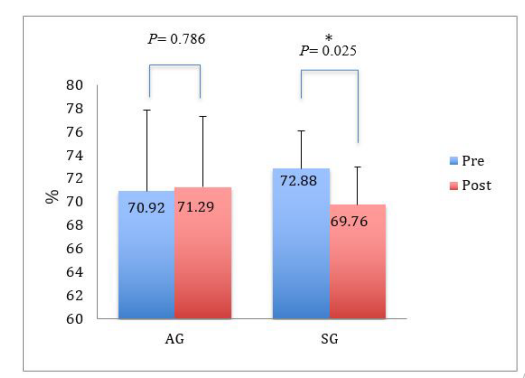 |
| Figure 1:CD3+ intra compare in pre-test and post-test. AG means acupuncture group, SG means sham acupuncture group. CD3+: cluster of differentiation 3. Values presented as mean ± SD. * mean P < 0.05; ** mean P < 0.01 |
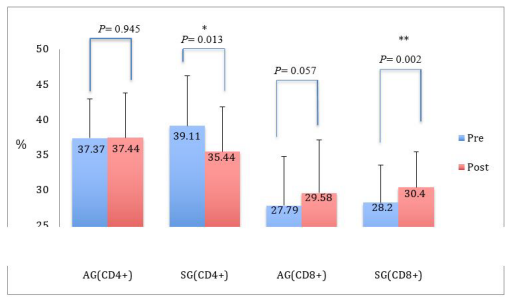 |
| Figure 2:CD4, CD8 intra compare in pre-test and post-test. AG means acupuncture group, SG means sham acupuncture group. CD: cluster of differentiation. Values presented as mean ± SD. * mean P < 0.05; ** mean P< 0.01 |
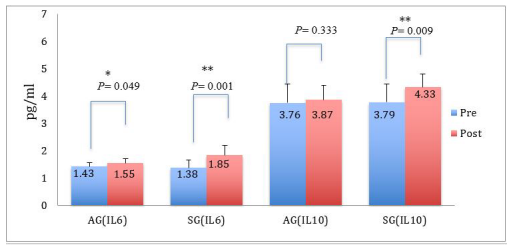 |
| Figure 3: IL-6, IL-10 intra compare in pre-test and post-test. AG means acupuncture group, SG means sham acupuncture group. IL: interleukin (pg/ml). Values presented as mean ± SD. * mean P < 0.05; ** mean P < 0.01 |
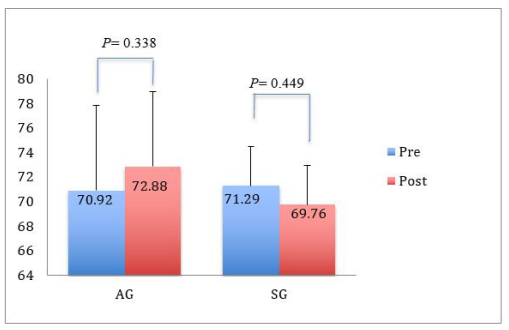 |
| Figure 4: CD3+ intra compare in pre-test and post-test. AG means acupuncture group, SG means sham acupuncture group. CD3+: cluster of differentiation 3. Values presented as mean ± SD. * mean P< 0.05; ** mean P< 0.01 |
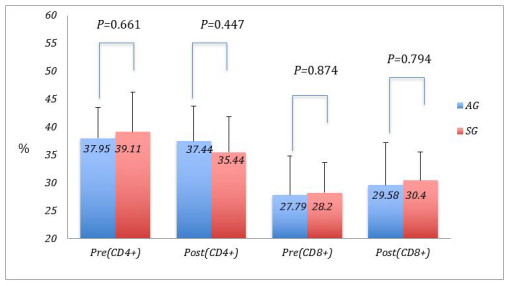 |
| Figure 5: CD4, CD8 inter compare in pre-test and post-test. AG means acupuncture group, SG means sham acupuncture group. CD: cluster of differentiation. Values presented as mean ± SD. * mean P < 0.05; ** mean P < 0.01 |
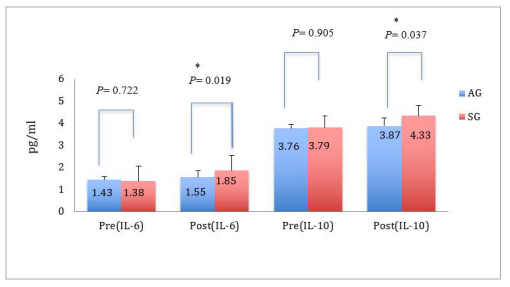 |
| Figure 6: IL-6, IL-10 inters compare in pre-test and post-test. AG means acupuncture group, SG means sham acupuncture group. IL: interleukin (pg/ml). Values presented as mean ± SD. * mean P < 0.05; ** mean P < 0.01 |
Introduction
Acupuncture, one of the traditional Chinese medi- cine (TCM) techniques, has long been used in clinic to treat illnesses or release pain, can be traced back to at least 2500 years ago. The most basic pattern is that uses hair-thin metal needles to puncture the skin at specific points on the body to remove blockages in the flow of Qi. The mechanism of acupuncture remains unclear, its effect is often dificult to gain wide acceptance, and modern medicine is hardly specific explain the term of TCM, for instance the meridians, acupoints, Yin and Yang, energy and Qi [1-3]. The mechanism of acupuncture is not clear, but many scholars had demonstrated various possible mechanisms from different rsearch fields, for example, gate control theory; release natural painkillers such as endorphin, encephalin, and dynorphin; involvement of serotonin and norepinephrine inhibition of pain [4-7].
Competition becomes increasingly fierce with the rapid development of sports science in the current athletic field. The “overload principle” or “super-compensation” is a common training modal used by coaches and athletes. An essential component of the model is that high-intensity exercise leads a disturbance in cellular homeostasis, so stimulus that initiate physiological responses to restore homeo- stasis and induce training adaptations. But the physiological endurance of sportsmen is limited, highintensity training and fierce competitive season would induce insufficiency recovery, fatigue accumulation, decline performance, chronic fatigue, sports injuries and immune dysfunction. An intensive schedule of training and competition leaded to immune system be impaired, especially increased the risk of upper respiratory tract infections (URTI) [8]. The relationship between exercise and upper respiratory tract infections (URTI) may be modeled in the form of a “Jcurve” [9,10]. Several authors have suggested that viruses and bacteria may easy gain a foothold during this “open windows” which should last between 3 and 72 hours after duration and intensity of exercise [11]. One good exercise recovery model should be able to shorten the recovery time, prevention of injuries, and avoid immunodeficiency.
Recently, acupuncture, one of effective, safe, ethical and legal practiced as alternative medical enhancer of sports performance had been applied to make one method of recovery [12]. The essence of traditional Chinese medicine (TCM) has been used to modulate the physical wellbeing of various athletes, refer to alleviation of muscle tension, improvement of local blood flow, increase of pain threshold, modulation of autonomic nervous system and readjust the immune systems [13].
To date, the effects of acupuncture therapy on rebalance immune functions during prolong high-intensity training session in soccer players are less known. This research would estimate the effect of acupuncture therapy to modulate immune para- meters during prolong high-intensity training in soccer players. We should try to provide theoretical and clinical guidance on the research of enhance recovery during prolonged high-intensive exercise with acupuncture therapy.
Method
Design and protocol:
This design for this study had been allocated into 2 parallel groups randomized controlled clinical trial (RCT). To determine the feasibility of conducting a clinical trial of acupuncture vs. mini sham acupuncture in these elite soccer players in university, assessing: a) It provides tight scientific control over threats to internal validity, the strength of the scientific inference supported by a study depends on its internal validity; b) 28 elite soccer players would be recruited from East China University of Political science and Law, be known the safety and efficacy of acupuncture therapy. The subjects will implement acupuncture and sham acupuncture intervention 3 times every week. Acupuncture therapy have more thousands history in China and the subject’s acceptability and compliance with protocols; c) the acupuncturist physician have over 10 years of experience, graduated from the Shanghai University of Chinese Medicine, acupuncture treated over 1000 cases.
SubjectsTwenty-eight male elite soccer players in East China of Political science and Law University, the subjects had been randomized equal to assign into acup- uncture group (AG) and sham group (SG) by a computer program basis on the list from the soccer coach. Coach and volunteers did not know who was divided into AG or SG. All of them were in good health based on clinical and physical examination, and no smoking, no alcohol, no history of hormone therapy, and no injury and acupuncture therapy during the last 6 months. All subjects underwent 6 times/week for 2 hour/session of high intensity, a large amount of exercise training, last 4 weeks. The acupuncture group had been carried out 3 times and continuing 20 min every time acupuncture stimulation in bilateral ST36 (Zusanli), IL4 (Hegu), BL23 (Shenshu), and LU5 (Chize) and delay 4 weeks. In this study, a special “placebo-needle” had been designed by Streitberger (1998) had been utilized and changed [14]. The sham needle tip was blunt and just touch the subject’s skin and a small pricking sensation be felt. Short needles had been applied in the SG, long needles had been applied in the AG. (See figure 1)
The baseline features of subjects were as follows: the average age was 22.6±3.5 years, the average weight was 68.7±14.6 kg, the average height was 176.8±36.1 cm. For the soccer players, the average duration of training experiences was 6.5±0.5 years. Two groups were evaluated during the same time at 7am-8am pre-experiment and post-experiment. The experimental room temperature kept 25 °C and kept relative air humidity between 50% and 60%. Every subject was instructed to rest more than 20 minutes before measurement, empty stomach and kept supine position during measurement.
Calculate the sample sizeThe sample size of each group in the main study was calculated according to the sample size formula for analysis of covariance (Borm et al., 2007) [15]. This study, we should apply type I error α=0.05, type II error ® = 0.1 power = 1- ® = P,bilateral alternative, for a power of 90% at a 5% significance and a dropout rate 10% will be allowed, calculate the sample size.
n/group =2σ2(Z1-α/2+Z1-β)2(1-ρ2)/(μ1-μ2)2
σ2 =[(n1-1)(SD1)2+(n2-1)(SD2)2]/(n1+n2-2)
Z1-α/2 =1.96, Z1-β =1.28
Refer to the previous study by Zhu et al. (2007) [16] had used AG and CG (control group) treatment the marathon athletes, collected blood to measure CK before match 1 day and after match 28 h, respective. The sample size in each group is be calculated as follows:
n1 =6, n2=6, SD1=10.25, SD2=13.29, μ1=50.92, μ2=65.32,
ρ=μ1/μ2=0.7795
σ2 =[(6−1)(10.25)2+(6-1)(13.29)2]/(6+6−2)=276.6
n =2×276.6× (1.96+1.28)2 × (1−0.77952)/ (65.32−50.92)2
n = 2265.35/207.36=10.924≈11
Dropout 10%, n adj= n/(1-R)2 n=sample size, R=ratio of % dropout
n/group=11/ (1-0.1)2=13.58≈14
We will confirm the sample size, only male, the acupuncture group, n=14, and control group, n=14.
Ethical approvalAll subjects had been informed that acupuncture therapy is a safety and efficacy treatment, and possible risks. The soccer coach and all subjects had been informed verbally and review the experimental protocol, and signing the consent form to participation in this experiment. The research protocol had been approved from the Ethical Committee of Khon Kean University (HE582343).
Acupuncture TherapyIn this study, a special “placebo-needle” had been utilized, detailed description of the following Figure. Acupuncture group (AG) will use 0.25/40 mm disposable stainless steel needles (Maanshan Bond Medical Instruments Co. Ltd, China) insert into the acupoints (Zusanli ST 36, Hegu IL 4, Shenshu BL 23, and Chize LU 5) on preceding part of text. Sham group will apply special technique (placebo-needle) to touch the near dermatome. Acupuncture intervention had been implemented between 8 pm to 9 pm on Monday, Wednesday and Friday every week, 4 weeks 12 times session together. Two groups had been arranged in different laboratory, different acupuncturist had operated, respectively. Before operated, need use 75% alcohol to disinfect the acupoints, needles and hands of acupuncturists. Needles had been continuous stimulated 20 min in both groups.
Main Outcomes Measure BiomarkersThe data from this study main include total T lymphocyte (CD3+), T helper (CD4+), T cytotoxic/suppressor (CD8+) (use a flow cytometry analysis); the pro-inflammatory and anti-inflammatory cytokine (IL-6), the anti-inflammatory cytokine (IL-10) (use Enzyme-Linked ImmunoSorbent Assay, ELISA analysis) had been measure by the experts before they had been trained and ability to proficient manipulate these test projects. The biomarkers had been test by the laboratory technicians of hospital. The first time test had been arranged in one week prior to this experiment, the second time test had been arranged in more than 36 h after intensity exercise or fierce match (next same).
Statistical AnalysisThe outcome measures had been analyzed and presented as mean ± standard deviations (SD). Two parallel groups, intragroups and inter-group compare and the numbers of sample (n/group< 30), 95% confidence level, a paired (intra-group) ttest and an unpaired (inter-group) t-test will be applied in this study. Analyses will be performed using SPSS 22 for mac. The level of statistical significance is set to p< 0.05.
Results
Compare Intra-Up the Effects of Acupuncture Therapy on Regulation CD3+, CD4+, and CD8+
In this study, CD3+ (the total T cell counts, cluster of differentiation 3), one T-cell co-receptor helps to activate the cytotoxic T-Cell, no statistically significant (P=0.786) between the baseline and post-test to compare in AG after 4 weeks, yet has a significant decrease in SG (P=0.025) (Table 2 and Figure 1). CD4+, T-lymphocyte help cell, has no significant change compare the baseline to post-test either in intra-up paired AG (P=0.945), but in SG, has significant decrease (P=0.013) (Table 2 and Figure 2). Meanwhile, CD8+, T-lymphocyte suppressor cell, was no significant higher compare the baseline to post-test (P=0.057) in intraup paired AG after 4 high-intensity training, but has an evident statistical significance higher in SG (P=0.002) (Table 2 and Figure 2). The ratios of CD4/CD8 have no statistically significant compare the pre-test to the post-test in AG (P=0.303); however, the ratio of CD4/CD8 have statistical significant different in SG (P=0.023) (Table 2). We believed that 4 weeks of high-intensity training had resulted to significant decrease in subjects’ CD3+, and acupuncture therapy were able to prevent further reduction. As well, 4 weeks high-intensity exercise had caused to significant in subjects’ CD4+, and acupuncture therapy could prevent further reduction for the CD4+ count. Whereas, CD8+ have increased trend though 4 weeks high-intensity training, acupuncture therapy could inhibit further increase.
Compare Intra-Up the Effects of Acupuncture on Regulation IL-6, IL-10
IL-6, an interleukin, acts as both a pro-inflammatory cytokine and an anti-inflammatory cytokine. The concentration of IL-6 has a significant increase compare the pre-test to the post-test in AG (P=0.049); and has a significant statistical significance in SG (P=0.001) (Table 2 and Figure 3). These revealed that prolong high-intensity exercise resulted to significant increase the concentration of IL-6 both AG and SG. However, compare between the pre-test to post-test, IL-10 has no statistical significance in AG (P=0.333), but has high correlation in SG (P=0.009) (Table 2 and Figure 3). We sugested that 4 weeks high-intensity training may induce IL-6, IL-10 to increase the secretion, and acupuncture therapy may be beneficial IL-6 and IL-10, especially IL-10 to generate.
Compare Inter-Group the Effects of Acupuncture Therapy on Regulation CD3+, CD4+, and CD8+In this study, no statistical significance either the markers of CD3+(pre, P=0.388; post, P=0.449), CD4+(pre, P=0.661; post, P=0.447) and CD8+(pre, P=0.874; post, P=0.759), and the ratios of CD4/CD8 (pre, P=0.885; post, P=0.567), compare the pre-test or post-test (Table 3, Figure 4, and Figure 5).
Compare Inter-Group the Effects of Acupuncture Therapy on Regulation IL-6, IL-10
The concentration of IL-6 has no statistical significance compare AG and SG in pre-test (P=0.722), but has significant difference in post-test (P=0.019). And well, IL-10 has no significant compare AG and SG in pre-test (P=0.905), but has significant increase in post-test (P=0.037) (Table 3 and Figure 6). These revealed that acupuncture therapy could inhibit these inflammatory cytokines further generate.
Discussions
This study aimed at investigating that the effects of acupuncture therapy compare to sham acupuncture on immune-regulation during prolong high-intensity exercise in soccer players. Our main finding was that acupuncture therapy may inhibit the total T cell to further decrease because prolong high-intensity exercise cause decrease. In addition, acupuncture therapy may delay CD8+ excessive increase to induce CD4/CD8 to further imbalance. Especially, acupuncture therapy may inhibit inflammatory cytokines (main investigating IL-6, IL-10) further secration, indicated that acupuncture therapy has the efficacy of both proinflammatory and anti-inflammatory.
Prolonged, high-intensity exercise due to neither percentage percentages nor absolute cell counts of the major immune cell lines (B, NK cells, total T, T helper/inducer, T suppressor/cytotoxic) change compare pre-training to posttraining [17]. T cell cytokine plays a major role in the immune responses against invading pathogens. Two distinct cytokine-producing CD4+ T helper and CD8+ T cytotoxic cell have been distinguished to type 1 and type 2, which through direct contact between or the release of cytokines, leading to stimulating or inhibiting effect, and the rules of immune response bidirectional appropriate strength. Each effect of CD4+ and CD8+ maintain the main immune balance of body’s, two subsets disorders due to immune dysfunction [18]. Many researchers had demonstrated that strenuous, exhaustive, and high-intensity training or competition could induce the absolute numbers of CD3+ and CD4+ cells decreased, CD8+ cells increased, and the ratio of CD4/CD8 decreased [19-22], The T-lymphocyte CD4+/CD8+ (helper/suppressor) easily influenced by CD8+ cells, and believed the ratio less than 1.5 being mean an increased susceptibility to infection [21]. Several previous researches reported that CD4+ T-lymphocyte counts decreased, and CD8+ cell counts increased at the end of season in soccer players [24,25], These results are consistent with our current research, especially in line this SG’ results.
Earlier an article had demonstrated that high-intensity eccentric exercise caused a more pronounced increase in the plasma level of IL-6, and that existed a significant correlation between the concentration of CK and IL-6 in the following days, suggested that cytokine more production was related to skeletal muscle damage [26]. Ostrowski et al. summarized the strenuous exercise induces the increase in the proinflammatory cytokines TNFα, IL-1β and a dramatic increase in the inflammation responsive cytokine IL-6, and released the cytokine inhibitors and the ant-inflammatory cytokine IL-10 to maintain the immune balance [27], Furthermore, Adam et al. (2003) demonstrated that a transient increase in plasma IL-6 induced an anti-inflammatory environment, for example, enhances the anti-inflammatory cytokine of IL-1 and IL-6, as well as induces an increase in cortisol [28] Gokhale R and his colleagues (2007) believed that physical training could modulate cytokine response [29].
Many previous papers had demonstrated the effect of acupuncture therapy on immune in human. Yamaguchi et al. suggested that acupuncture treatment could regulate the immune system and promote the activities of hormonal and cellular immunity as well as NK cell activity [30]. Johnston et al. demonstrated acupuncture enhances anti-cancer immune functions and first put forward the argument of “acupuncture immune-enhancement hypothesis” [31]. The mechanisms of acupuncture on immune regulation had been demonstrated from several factors, for example modulation Th1/Th2 [32-34]. improve the activity/cytotocix of T cells, B cells and NK cells [35-37] activity or inhibit the autonomic nervous system modulate immune system [38-40] and increase or decrease endocrine system β-adrenergic [41], cortical modulate leukocyte and lymphocyte values [42]. Gao et al. had evaluated the effect of acupuncture pretreatment on the wrestling athletes in CD3+, CD4+, CD8+ and the CD4+/CD8+ ratio during high-intensity training, demonstrated that acupuncture pretreatment possessed to delay and prevent the decline of immunity [43]. Carneiro et al. showed that this beneficial effect of EA increased the release of IL1 cytokines, IL-1 and IFN-γ, decreased the release of IL2 cytokines, IL-4 and IL-10. They demonstrated that EA is related to the regulation of the balance of the IL1/IL2 response and the beneficial anti-inflammatory and immune-regulation [44]. Lundeberg et al. demonstrated that acupuncture enhanced the immune reaction to belong to stimulate of the sympathetic nervous system to release βadrenergic and activate the non-specific helper T lymphocytes [41]. Mori et al. suggested that acupuncture stimulate the autonomic nervous system due to decrease blood pressure induce immunomodulation and the mechanism of acupuncture may improve the condition of patients with many chronic diseases [45]. Ben K & B Evan Ross (2007) had verified the electro-acupuncture stimulation of the vagus nerve inhibits macrophage activation and the production of TNF, IL-1, IL-6, IL-18, and other proinflammatory cytokines through a confirming experimentation [46].
We believed that prolonged, high-intensity training could decrease the athletes’ immunity, and the higher CD8+ T cell counts in SG response the subjects’ immunity decrease. Meanwhile, we had well found that the CD8+ T cell counts increase was the major factors induce to the CD4/CD8 ratios decrease. Furthermore, we had found that acupuncture treatment was provided to prevent the exercise-induce immunity decrease. Results of this study corresponded with other researches [43,47].
IL-6 has clearly statistical significance compare pre-test with post-test in two groups. However, IL-10 (anti-inflammatory responsive cytokine) just has a significant higher in SG, no statistical significance. Furthermore, we found that both IL-6 and IL-10 have significant difference compare two groups after 4 weeks high-intensity training. The complex phenomenon completely corresponded with previous studies [27,48]. The results showed prolonged high-intensity exercise cause muscle damage to release large of IL-6 cytokine, and induce the large release IL-10. On the other hand, acupuncture treatment may inhibit the cytokines, main include pro-inflammatory IL-6 and anti-inflammatory IL-10 to further release.
Conclusion
Prolong, high-intensity training session in soccer players cause by decreased immune functions, increase level of proand anti-inflammatory cytokines. Acupuncture therapy could facilitate to restore immune function, inhibition the soccer player’s immunity to further reduce. One the other hand, acupuncture therapy could inhibit inflammatory cytokines (main investigating IL-6, IL-10) further generation, indicated that acupuncture therapy has the efficacy of both pro- and anti-inflammatory. On the other words, acupuncture therapy may decrease high-intensity induce muscle damage, alleviative inflammatory, delay or prevent immunodeficiency and maintain the steady status of immune function.
Funding
This research was funded by Ministry of Science and Technology of China, [2020YFC2007205].
Acknowledgments
We would like to make a grateful acknowledgement to all persons who have helped us with this study
Conflicts of Interest
The authors declare that there is no conflict of interests regarding the publication of the paper.
References
- Aung SKH, Chen WPD (2007) “Clinical Introduction to Medical Acupuncture,” New York, NY: Thieme Medical Publishers, Inc.
- Ernst E (2006) “Acupuncture–a critical analysis,” Journal of internal medicine 259: 125-137.
- Cao X (2002) “Scientific bases of acupuncture analgesia.” Acupuncture & electro-therapeutics research 27: 1-14.
- Anderson SA, Holmgren E (1975) “On Acupuncture Analgeisa and the Mechanism of Pain.” The American journal of Chinese medicine 3: 311-34.
- Han JS, Terenius L (1982) “Neurochemical basis of acupuncture analgesia.” Annual review of pharmacology and toxicology 22: 193-220.
- Huang C, Wang Y, Chang JK, Han JS (2000) “Endomorphin and μ-opioid receptors in mouse brain mediate the analgesic effect induced by 2 Hz but not 100 Hz electroacupuncture stimulation.” Neuroscience letters 294: 159-62.
- Han JS (2003) “Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies.” Trends in neurosciences 26: 17-22.
- Peters EM (1990) “the effect of altitude on the incidence of upper respiratory tract infections following participation in ultramarathon events.” S Afr Sports Med 5: 4-8.
- Nieman DC (1994) “Exercise, upper respiratory tract infection, and the immune system,” Med Sci Sports Exerc 26: 128-39.
- Nieman DC (1997) “Risk of Upper Respiratory Tract Infection in Athletes: An Epidemiologic and Immunologic Perspective,” J Journal of Athletic Training 32: 344-8.
- Pedersen BK, Rohde T, Ostrowski K (1998) Recovery of the immune system after exercise. J Acta Physiol Scand 162: 325-32.
- Ahmedov S (2010) “Ergogenic effect of acupuncture in sport and exercise: A brief review,” J Strength Cond Res 24: 1421-7.
- Peltham TW, LE Holt, R Salker (2001) “Acupuncture in human performance,” J. Strength Cond. Res 15:266-71.
- Streitberger K, J Kleinhenz (1998) “Introducing a placebo needle into acupuncture research,” Lancet 352: 364-5.
- Borm GF, Fransen J, Lemmens W (2007) A sample size formula for analysis of covariance in randomized clinical trials. J Cli Epidemiol 60: 1234-8.
- Zhu Z, Yang YT, Yang JT, Wei FG, Chen PJ (2007) Acupuncture effect on the medium - long distance athlete’s physical efficiency recovery after half- marathon race. Journal of Chendu Sport University 3: 83-6.
- Holger HWG, U Axel V. Gunter et al. (1998) “Overtraining and immune system: a prospective longitudinal study in endurance athletes,” J the American College of Sports Medicine 30: 1151-7.
- BK Pedersen, T Rohde, K Ostrowski (1998) “Recovery of the immune system after exercise,” J Acta Physiol Scand 162: 325-32.
- DC Nieman, DA Henson, MD Austin, VA Brown (2005) “Immune response to 30-minute walk,” Med Sci Sports Exerc 37: 57-62.
- Z Baj, J Kantorski, E Majewska et al. (1994) “Immunological status of competitive cyclists before and after the training season,” Int J Sports Med 15: 319-24.
- LS Berk, SA Ton, DC Nieman, EC Eby (1986) “The suppressive effect of stress from acute exhaustive exercise on T-lymphocyte helper/suppressor ratio in athletes and nonathletes,” Med Sci Sports Exerc 18: 706-10.
- GI Lancaster, SL Halson, Q Khan et al. (2004) “the effects of acute exhaustive exercise and intensified training on type 1/type 2 T cell distribution and cytokine production,” Exerc Immunol Rev 10: 91-106.
- A Kendall, L Hoffman-Goetz, M Houston et al. (1990) “Exercise and blood lymphocyte subset responses: intensity, duration, and subject fitness effects,” J Appl Physiol 69: 251-60.
- T Bury, R Marechal, P Mahieu, F Pirnay (1998) “Immunological status of competitive football players during the training season,” Int J Sports Med 19: 364-8.
- AN Rebelo, JR Candeias, MM Fraga et al. (1998) “the impact of soccer training on the immune system,” J Sports Med Phys Fitness 38: 258-61.
- H Bruunsgaard, H Galbo, J Halkjaer-Kristensen, TL Johansen, DA MacLean, BK Pedersen (1997) “Exerciseinduced increase in serum interleukin-6 in humans is related to muscle damage,” The Journal of physiology 499: 833-41.
- K Ostrowski, C Hermann, A Bangash et al. (1998) “A trauma-like elevation of plasma cytokines in humans in response to treadmill running,” J Physiol 513: 889-94.
- S Adam, PF Christian, K Charlotte et al. (2003) “IL-6 enhances plasma IL-1ra, IL-10, and cortisol in humans,” Am J Physiol Endocrinol Metab 285: 433-7.
- R Gokhale, S Chandrashekara, KC Vasanthakumar (2007) “Cytokine response to strenuous exercise in athletes and nonathletes—an adaptive response Cytokine,” 40: 123-7.
- N Yamaguchi, T Takahashi, M Sakuma et al. (2007) “Acupuncture regulates leukocyte subpopulations in human peripheral blood,” Evidence-Based Complementary and Alternative Medicine 4: 447-53.
- MF Johnston, ES Ortiz, NL Vujanovic, W Li (2011) “Acupuncture may stimulate anticancer immunity via activation of natural killer cells,” Evidence-Based Complementary and Alternative Medicine.
- HS Park, KS Kim, HK Min, DW Kim (2004) “Prevention of postoperative sore throat using capsicum plaster applied at the Korean hand acupuncture point,” Anaesthesia 59: 647-51.
- Y Lee, SK Kim, Y Kim, et al. (2007) “The adrenoceptor mediation of the immunomodulatory effects of electroacupuncture in DNP-KLH immunized mice,” Neuroscience Letters 423: 149-52.
- YK Yim, H Lee, KE Hong et al. (2010) “Antiinflammatory and Immune-regulatory Effects of Subcutaneous Perillae Fructus Extract Injections on OVAinduced Asthma in Mice,” Evid based Complement Altermat Med 7: 79-86.
- Y Yu, T Kasahara, K Sato et al. (1998) “Role of endogenous interferon-γ on the enhancement of splenic NK cell activity by electro acupuncture stimulation in mice,” Journal of Neuroimmunology 90: 176-86.
- I Pais, N Correia, I Pimentel et al. (2014) “Effects of acupuncture on leucopenia, neutropenia, NK, and B cells in cancer patients: a randomized pilot study,” Evidence-Based Complementary and Alternative Medicine.
- ME Wechsler, JM Kelley, IO Boyd et al. (2011) “Active albuterol or placebo, sham acupuncture, or no intervention in asthma,” New England Journal of Medicine 365: 119-26.
- EM Friedman, MR Irwin (1997) “Modulation of immune cell function by the autonomic nervous system,” Pharmacology & therapeutics 74: 27-38.
- JE Downing, JA Miyan (2000) “Neural immunoregulation: emerging roles for nerves in immune homeostasis and disease,” Immunology today 21: 281-9.
- CJ Czura, KJ Tracey (2005) “Autonomic neural regulation of immunity,” Journal of Internal Medicine 257: 156-66.
- T Lundeberg, SV Eriksson (1991) “Theodorsson Neuroimmunomodulatory effects of acupuncture in mice,” Neuroscience Letters 128: 161-4.
- W Kou, JD Bell, I Gareus et al. (2005) “Repeated acupuncture treatment affects leukocyte circulation in healthy young male subjects: a randomized single-blind twoperiod crossover study,” Brain, behavior, and immunity 19: 318-24.
- M Gao, Y Wu, ZT Sheng et al. (2014) “Effect on NK Cells and T Lymphocyte Subgroup of Wrestlers during the Course of Heavy Load Training of Acupuncture Pretreatment,” J Shanghai University of Sport 38: 67-72.
- ER Carneiro, RAN Xavier, DP Castro, CO Nascimento (2010) “Electroacupuncture promotes a decrease in inflammatory response associated with Th1/Th2 cytokines, nitric oxide and leukotriene B4 modulation in experimental asthma,” Cytokine 50: 335-40.
- H Mori, K Nishijo, H Kawamura, T Abo (2002) “Unique immunomodulation by electro-acupuncture in humans possibly via stimulation of the autonomic nervous system,” Neuroscience letters 320: 21-4.
- B Kavoussi, B Evan Ross (2007) “The Neuroimmune Basis of Anti-inflammatory Acupuncture.,” Integrative Cancer Therapies 6: 251-7.
- CQ Hong, MH Xie, X Yan (2015) “Effect of High-Load Resistance Training on the Amount of Immune Cell Surface Markers in Lifters,” J Shanghai University of Sport 39: 46-9.
- R Gokhale, S Chandrashekara, KC Vasanthakuma (2007) “Cytokine response to strenuous exercise in athletes and nonathletes—an adaptive response,” Cytokine 40: 123-7.
Article Information
Research Article
Received Date: February 08, 2026
Accepted Date: February 18, 2026
Published Date: February 21, 2026
Comparison of Three Therapeutic Methods of Transcutaneous Electrical Nerve Stimulation, Embedding Acupuncture, and Drug Therapy on Interleukin-6 and Pain Levels in Patients with Knee Osteoarthritis
Volume 1 | Issue 1
Citation
Shihang Lin, Xingze Wang, Somchai Rattanathongkom, Wichai Eungpinichpon (2026) Effects of Acupuncture on Immunoregulation During Prolonged High-Intensity Training Session in Soccer Players. J Traditional Complement Altern Med 1:105
Copyright
©2026 Xingze Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

doi: jtca.2026.1.105